What is asd pda and vsd devices how they are deployed and how to measure septal wall hole size to deploy appropriate devise ???
Reading File
Finding Sources
Finding Sources
Searching the Web
ASD VSD PDA occluder device deployment catheterization septal defect sizing
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"septal defect" AND "device closure" AND "sizing"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
ASD VSD PDA occluder device deployment cardiac catheterization
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
ASD, VSD & PDA Device Closure — Devices, Deployment, and Sizing
Overview
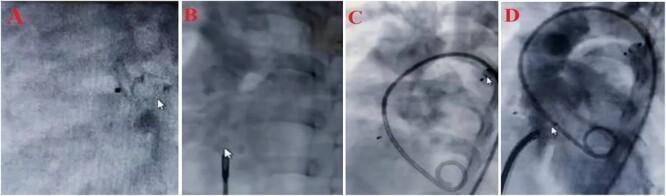
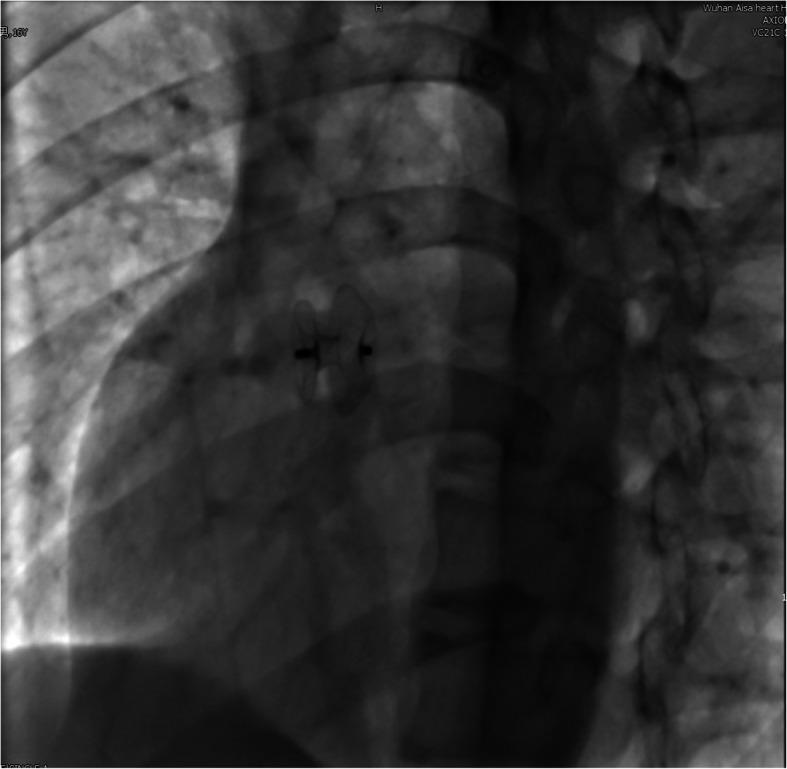
All three defects — Atrial Septal Defect (ASD), Ventricular Septal Defect (VSD), and Patent Ductus Arteriosus (PDA) — can be closed percutaneously via transcatheter (catheterization lab) techniques using self-expanding nitinol mesh occluder devices, avoiding open-heart surgery in eligible patients.
1. Atrial Septal Defect (ASD)
What is it?
An abnormal opening between the two atria (upper chambers). The most common type amenable to device closure is the ostium secundum ASD, which accounts for ~75% of ASDs. Left-to-right shunting causes RV volume overload; if untreated, pulmonary hypertension develops by the 6th decade.
Devices Available
| Device | Structure | Key Features |
|---|---|---|
| Amplatzer Septal Occluder (ASO) (Abbott) | Woven nitinol, double disc + central waist, filled with Dacron fibers | Self-centering; gold standard; sizes 4–40 mm |
| GORE Cardioform ASD Occluder (GCA) | Nitinol frame + ePTFE membrane, 5-wire design | Non-self-centering; sizes 27–48 mm; treats defects 8–35 mm; no erosion risk even with deficient retroaortic rim |
| GORE Cardioform Septal Occluder (GSO) | Nitinol + ePTFE | Treats defects up to 18 mm |
Deployment Steps (ASO — most widely used)
- Venous access — Right femoral vein; diagnostic catheterization to confirm left-to-right shunt and measure Qp:Qs
- Transseptal positioning — A guidewire is advanced across the defect into the left atrium (LA); the proprietary TorqVue delivery sheath is positioned in the LA
- Sizing (see detailed sizing section below)
- Left atrial disc deployment — The left disc is unsheathed in the LA
- Pull back to septum — Sheath + device are pulled back so the left disc seats against the left side of the septum
- Right atrial disc deployment — The right disc is deployed on the RA side, "sandwiching" the septal wall
- Device testing — Gentle tug ("Minnesota wiggle") confirms secure position; color Doppler confirms no residual shunt
- Release — Device is unscrewed from delivery cable
- Imaging — Fluoroscopy + TEE/ICE confirm position and absence of obstruction to pulmonary veins, AV valves, coronary sinus
Guidance: Transesophageal echocardiography (TEE) or intracardiac echocardiography (ICE) is used throughout
Indications for ASD Device Closure
- RV/RA dilatation with or without symptoms (Class I)
- Qp:Qs ≥ 1.5:1 or RV enlargement on echo
- Paradoxical embolism / platypnea-orthodeoxia (Class IIa)
- Minimum defect diameter >5 mm, maximum <40 mm
- All rims ≥5 mm to coronary sinus, IVC, AV valves, and right upper pulmonary vein
Contraindications
- Sinus venosus or primum ASDs (require surgery)
- Eisenmenger syndrome (irreversible pulmonary hypertension)
- Active infection/sepsis within 1 month
- Intracardiac thrombus on echo
- Rims <5 mm to adjacent critical structures (relative, especially for ASO)
2. Ventricular Septal Defect (VSD)
What is it?
An abnormal communication between the two ventricles. Types: perimembranous (most common, ~80%), muscular, outlet (supracristal), inlet. Muscular and selected perimembranous VSDs are candidates for transcatheter closure.
Devices Available
| Device | Indication |
|---|---|
| Amplatzer Muscular VSD Occluder | Muscular VSDs |
| Amplatzer Membranous VSD Occluder | Perimembranous VSDs (with higher AV block risk) |
| Amplatzer Post-Infarct Muscular VSD Occluder | VSD complicating acute MI (larger, stiffer discs) |
| Amplatzer Septal Occluder (off-label) | Large muscular / post-MI VSDs |
Deployment Steps
- Arteriovenous loop creation — Femoral artery and vein access; a guidewire is passed antegrade from RV → VSD → LV → aorta → captured in femoral artery, creating an arteriovenous loop
- Sheath positioning — A long delivery sheath is advanced from the venous side through the RV across the VSD into the LV
- Left ventricular disc deployment — Device LV disc opened in LV
- Pullback to septum — Device pulled against the LV face of the septum
- Right ventricular disc deployment — RV disc opens on RV side
- Confirmation + release — Fluoroscopy and TEE/ICE verify position; no significant residual shunt; device released
Special Consideration — Post-MI VSD
Post-infarction VSDs are friable and have high operative mortality. Percutaneous closure with the Amplatzer Post-Infarct Muscular VSD device or standard ASO has been attempted, with outcomes for percutaneous closure better than late surgical repair.

Complications — VSD-specific
- Complete heart block — Higher risk with perimembranous VSD devices (proximity to AV node/bundle of His); reported in ~1–5% of perimembranous closures
- Device embolization
- Hemolysis from residual shunt
3. Patent Ductus Arteriosus (PDA)
What is it?
Persistent communication between the main pulmonary artery and the descending aorta, normally closes physiologically after birth. A large PDA causes left-to-right shunt, LV volume overload, pulmonary overcirculation, and eventually pulmonary hypertension.
Devices Available
| Device | Best For |
|---|---|
| Amplatzer Ductal Occluder I (ADO-I) | Moderate-large conical PDAs; nitinol mesh + Dacron; asymmetric retention disc |
| Amplatzer Ductal Occluder II (ADO-II) | Small-moderate PDAs; symmetric retention skirts → can be deployed antegrade or retrograde |
| Amplatzer Vascular Plug II (AVP-II) | Long tubular PDAs; sizes 3–22 mm; very low profile |
| Amplatzer Vascular Plug IV (AVP-IV) | Small tubular PDAs; sizes 4–8 mm; lowest profile |
| Nit-Occlud (PFM Medical) | Single nitinol coil; funnel-shaped; delivered via 4 Fr catheter; controlled release mechanism |
| Gianturco coils | Small PDAs (<2.5 mm) |
Deployment Steps (ADO-I — standard approach)
- Femoral vein access — Catheter advanced RV → pulmonary artery → ductus → descending aorta
- Aortogram — Defines PDA morphology (Type A = conical, commonest; Types B–F = tubular, window, complex)
- Sheath positioning — Delivery sheath positioned in the descending aorta via the PDA
- Retention disc deployment — The aortic retention disc is opened in the descending aorta
- Pull back into ductus — The device is pulled into the PDA; the pulmonary end (plug portion) sits in the PDA ampulla
- Confirmation — Aortogram confirms no protrusion into pulmonary artery or aorta; no significant residual shunt
- Release
ADO-II can also be placed retrograde (arterial approach): catheter from femoral artery → aorta → PDA → pulmonary artery
4. How to Measure Septal/Defect Size to Select the Appropriate Device
This is the most critical step. Accurate sizing prevents under-sizing (residual shunt, device embolization) and over-sizing (erosion, obstruction of adjacent structures).
A. Echocardiographic Measurement (First Step — Always)
Modalities used:
- Transthoracic echocardiography (TTE) — Initial assessment, especially in children
- Transesophageal echocardiography (TEE) — Standard of care for intraprocedural guidance; multiplane views at 0°, 45°, 90°, 135°
- Intracardiac echocardiography (ICE) — Increasingly used in adults; allows procedure without general anesthesia
- 3D echocardiography — Most accurate for true defect geometry; allows en face "surgical" view of septum
What to measure on echo:
- Maximum ASD diameter in multiple planes (defects are often oval)
- Rim assessment — Distance from defect edge to: coronary sinus, IVC, SVC, right upper pulmonary vein, AV valves, aorta (retroaortic rim)
- Total septal length — Device disc must not exceed it
- Rims <5 mm to critical structures = relative contraindication for ASO (but GCA can still be used for deficient retroaortic rim)
B. Balloon Sizing — Stretched Diameter (Gold Standard for ASD)
The stretched diameter (SD) is the most important measurement for ASD device selection. The compliant ASD stretches considerably beyond its echocardiographic diameter.
Technique (Stop-Flow Method — preferred):
- A sizing balloon (e.g., NuMED Sizing Balloon) is advanced across the ASD
- The balloon is gradually inflated with dilute contrast under fluoroscopy and echo guidance
- Inflation continues until left-to-right flow ceases (color Doppler shows no flow through defect) — the "stop-flow" endpoint
- The balloon diameter at this point = stretched diameter
- Avoid over-inflation — do not inflate >1.5× the static echocardiographic dimension (to minimize erosion risk)
Device size selection:
- ASO: Choose device = same size OR at most 1 mm larger than the stop-flow stretched diameter
- For defects with deficient retroaortic rim (<5 mm): use stop-flow sizing carefully; GCA is preferred as it carries no erosion risk
- ASD criteria for device closure: minimum diameter >5 mm, maximum stretched diameter <40–41 mm
C. Angiographic Sizing (PDA)
For PDA, sizing is done angiographically:
- Lateral aortogram (90° projection) with catheter in the ampulla of the ductus
- Measure: narrowest PDA diameter (pulmonary end), length of the ductus, and ampulla diameter (aortic end)
- ADO-I device selection: device diameter should be 1–2 mm larger than the narrowest PDA diameter; device length should match PDA length
- ADO-II: device diameter = 2× the narrowest PDA diameter
D. VSD Sizing
- Echo measurement: 2D TTE/TEE measures defect in multiple views
- Balloon sizing may be performed for large muscular VSDs
- Amplatzer muscular VSD occluder size = stretched diameter + 1–2 mm (to ensure adequate coverage of both LV and RV faces)
Summary Table — Device Selection Rules
| Defect | Measure | Method | Device Size Formula |
|---|---|---|---|
| ASD | Stretched diameter (stop-flow) | Balloon sizing + TEE | Device = stretched diameter (same or +1 mm) |
| ASD small | Echo max diameter | 2D/3D echo | Direct echo sizing if <15 mm |
| VSD | Echo + balloon stretched diameter | TEE + balloon | Device = stretched diameter + 1–2 mm |
| PDA | Narrowest diameter + ampulla | Lateral aortogram | ADO-I = narrowest +1–2 mm; ADO-II = narrowest ×2 |
Key Complications Across All Three
| Complication | ASD | VSD | PDA |
|---|---|---|---|
| Device embolization | + | + | + |
| Residual shunt/hemolysis | + | + | + |
| Device erosion | ++ (ASO-specific) | – | – |
| Complete heart block | Rare | ++ (perimembranous) | – |
| Thrombus/stroke | + | – | – |
| LPA/aortic obstruction | – | – | + |
| Arrhythmia | + | + | – |
Sources: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (10e), Chapter 83 — Transcatheter Interventions; Amplatzer device IFU (Abbott Inc.); ACC/AHA congenital heart disease guidelines
This is a shared conversation. Sign in to Orris to start your own chat.