Oesophagus
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have rich content from Schwartz's Principles of Surgery covering major oesophageal surgical conditions and management. Let me compile a comprehensive answer.
Oesophagus: Clinical Management & Surgery
Overview of Surgical Principles
The oesophagus is among the most surgically challenging organs. Key preoperative priorities are:
- Diagnosis - barium swallow, oesophagoscopy, manometry, pH studies
- Nutritional optimisation - malnutrition is "malignant" and directly increases anastomotic leak risk after resection
- Pulmonary preparation - physiotherapy and postural drainage, as aspiration is common
(Pye's Surgical Handicraft, 22nd ed.)
1. Achalasia
Pathophysiology: Loss of inhibitory ganglion cells in the myenteric plexus - failure of LES relaxation and absent peristalsis. Three subtypes on manometry (Types I-III).
Management options:
| Treatment | Notes |
|---|---|
| Pneumatic dilation | First-line in non-surgical candidates; risk of perforation (~1-3%) |
| Laparoscopic Heller myotomy (LHM) | Gold standard surgical treatment; combined with partial fundoplication (Dor or Toupet) to prevent reflux |
| POEM (Per-Oral Endoscopic Myotomy) | Preferred for Type III (vigorous/spastic) achalasia; long submucosal tunnel; outpatient; no anti-reflux wrap |
| Botulinum toxin injection | Temporary; elderly/unfit patients |
- LHM vs. pneumatic dilation: comparable outcomes at 2 years; LHM more durable long-term
- Prior endoscopic therapy (dilation/Botox) before LHM leads to worse outcomes than LHM alone
- POEM results still accumulating but extremely minimally invasive; can divide muscle both above and below diaphragm (useful in Type III)
(Schwartz's Principles of Surgery, 11th ed.; Clinical Gastrointestinal Endoscopy, 3rd ed.; Fischer's Mastery of Surgery, 8th ed.)
2. Oesophageal Diverticula
- Epiphrenic diverticula: excise the neck with a stapler; myotomy on the opposite wall; cannot be treated with POEM
- Midesophageal diverticula: myotomy includes muscle at the neck; diverticulum suspended to paravertebral fascia
- Always endoscope preoperatively to clear food/debris from the diverticulum
- Laparoscopic approach preferred for epiphrenic diverticula + Heller myotomy
3. Gastro-Oesophageal Reflux Disease (GORD/GERD)
Surgical indication: failed medical therapy, large hiatal hernia, patient preference
Approach: Laparoscopic fundoplication (Nissen - 360° wrap; Toupet - 270° posterior; Dor - anterior)
- Nissen fundoplication is the most common antireflux procedure
- When combined with Heller myotomy, partial (Dor or Toupet) fundoplication preferred to avoid dysphagia
- Preoperative manometry mandatory to detect poor oesophageal motility (which favours partial wrap)
4. Oesophageal Carcinoma
Types
- Squamous cell carcinoma (SCC): mid/upper oesophagus; associated with smoking, alcohol
- Adenocarcinoma: lower oesophagus/GOJ; associated with Barrett's oesophagus (GORD-related)
Staging & Investigation
- CT chest/abdomen/pelvis, EUS (endoscopic ultrasound for T/N staging), PET scan
- Staging laparoscopy for lower oesophageal/GOJ tumours
Surgical Options - Oesophagectomy
| Approach | Description |
|---|---|
| Ivor Lewis (two-stage) | Right thoracotomy + laparotomy; intrathoracic anastomosis; for mid/lower oesophagus |
| McKeown (three-stage) | Abdomen + right chest + cervical anastomosis; for upper/mid oesophagus |
| Transhiatal oesophagectomy | No thoracotomy; blunt dissection; cervical anastomosis; less pulmonary morbidity |
| Minimally invasive oesophagectomy (MIE) | Thoracoscopic + laparoscopic; ROMIO trial showed non-inferiority vs. open; less pulmonary morbidity |
Conduit: Gastric tube most common; colon or jejunum if stomach unavailable
Lymphadenectomy: Two-field (abdominal + mediastinal) standard; three-field (+ cervical) for upper SCC
Neoadjuvant Therapy
- Neoadjuvant chemoradiotherapy (CROSS protocol) + surgery - standard of care for locally advanced disease
- Perioperative chemotherapy (FLOT regimen) for adenocarcinoma GOJ
Complications of Oesophagectomy
- Anastomotic leak - most feared complication; malnutrition is a major risk factor; intrathoracic leaks have higher mortality than cervical
- Selective management: cervical leaks can be opened and drained; intrathoracic leaks may need re-operation or stenting
- Pulmonary complications (pneumonia, ARDS) - reduced with protective ventilation strategies and MIE
- Recurrent laryngeal nerve injury
- Chyle leak
(Schwartz's 11th ed.; Mulholland and Greenfield's Surgery, 7th ed.; Maingot's Abdominal Operations; Fischer's Mastery of Surgery 8th ed.)
5. Oesophageal Perforation
- Causes: Iatrogenic (oesophagoscopy - most common), spontaneous (Boerhaave syndrome - transmural rupture from sudden pressure rise after vomiting)
- Key principle: Repair within a few hours - early primary suture repair has low risk. Delayed diagnosis dramatically increases morbidity and mortality
- Investigation: Chest X-ray (mediastinal emphysema, pleural effusion), contrast swallow (use thin barium or water-soluble contrast)
- Thoracic perforation: presents with chest pain; confirm with imaging
- Management:
- Early (<24h): primary repair ± tissue reinforcement (pleural flap, intercostal muscle)
- Late/contaminated: drainage, exclusion procedures, or oesophageal stenting
- Boerhaave: aggressive surgical drainage; mortality rises steeply with delay
(Pye's Surgical Handicraft, 22nd ed.)
6. Oesophageal Motor Disorders (Other)
- Diffuse oesophageal spasm / Nutcracker oesophagus / Jackhammer oesophagus: Chest pain + dysphagia; high-amplitude or simultaneous contractions on manometry
- Surgery: Long oesophageal myotomy (from aortic arch to GOJ) - 93% palliation of dysphagia at 5 years when done accurately
- Thoracoscopic approach (right chest) combined with abdominal approach for full myotomy + partial fundoplication
Key Surgical Principles Summary
| Condition | Primary Surgical Procedure |
|---|---|
| Achalasia | Laparoscopic Heller myotomy + partial fundoplication |
| Type III Achalasia | POEM |
| GORD | Laparoscopic Nissen/Toupet/Dor fundoplication |
| SCC/Adenocarcinoma | Oesophagectomy (Ivor Lewis / McKeown / Transhiatal / MIE) |
| Perforation (early) | Primary suture repair |
| Perforation (late) | Drainage ± stenting |
| Motor disorders | Long oesophageal myotomy |
| Epiphrenic diverticulum | Diverticulectomy + myotomy |
According to anatomy
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the anatomical detail needed for a comprehensive response. Let me compile it.
Anatomy of the Oesophagus
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery)
1. Overview
The oesophagus is a 25 cm long, flattened muscular tube that is the direct continuation of the pharynx. It extends from the inferior border of the cricoid cartilage (C6) to the cardiac orifice of the stomach (T11). It is the narrowest part of the digestive tract (excluding the appendix).
It passes anterior to the vertebral column in the neck, then through the superior and posterior mediastinum, and pierces the diaphragm at the oesophageal hiatus (T10).
2. Subdivisions
The oesophagus has three parts:
A. Cervical Oesophagus (C6 - T1)
- Lies immediately posterior to the trachea, attached by loose connective tissue
- Slightly to the left of midline at the level of the thyroid gland
- Posteriorly rests on C6-C7 vertebral bodies and prevertebral fascia (over longus colli)
- Flanked by common carotid arteries and lower poles of thyroid gland
- Recurrent laryngeal nerves run in the groove between oesophagus and trachea on both sides
- The thoracic duct ascends on its left side briefly before draining into the subclavian-jugular confluence
B. Thoracic Oesophagus (T1 - T10)
- In the superior mediastinum: runs slightly left of midline; passes posterior to the aortic arch to enter the posterior inferior mediastinum
- In the posterior mediastinum: descends to the right of the descending aorta, then veers left toward the hiatus
- Anterior relations (posterior mediastinum): left main bronchus, tracheobronchial lymph nodes, pericardium, left atrium
- Posterior relations: thoracic vertebrae T1-T4, thoracic duct (between azygos vein and aorta), right posterior intercostal arteries, hemiazygos veins
- Left side: mediastinal pleura (superior to aortic arch), thoracic duct, left subclavian artery
- Right side: adjacent to mediastinal pleura and lung, with azygos vein intervening
- The oesophageal plexus (vagus + sympathetic fibres) wraps around the lower thoracic oesophagus
C. Abdominal Oesophagus (T10 onward)
- Emerges through the right crus of diaphragm, left of midline at T10
- Lies in the oesophageal groove on the posterior surface of the left lobe of the liver
- Covered by peritoneum; contained within the lesser omentum
- Right border continues as the lesser curvature of the stomach
- Left border is separated from the fundus by the cardiac notch
- Left vagus (2-3 trunks) lies anteriorly; right vagus (single trunk) lies posteriorly
3. Oesophageal Constrictions
The oesophagus has three anatomical constrictions (visible on barium swallow / at endoscopy), plus the cricopharyngeal sphincter at its start:
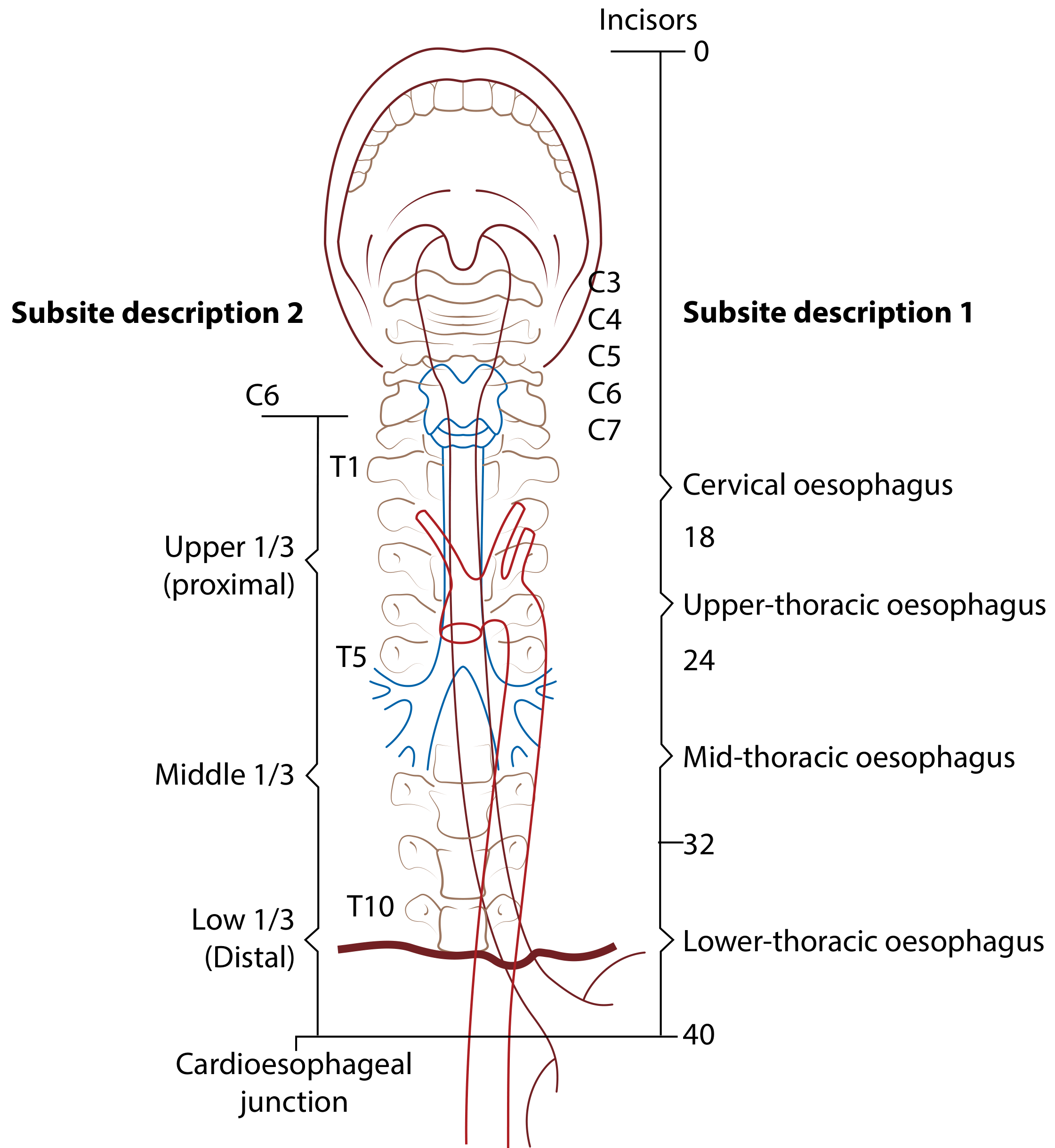
| Constriction | Cause | Distance from Incisors |
|---|---|---|
| Cricopharyngeal sphincter | Junction of pharynx and oesophagus | 15 cm (narrowest point) |
| Aortic arch | Arch of aorta crossing over | 22 cm |
| Left main bronchus | Left main bronchus crossing | 27 cm (often grouped with aortic) |
| Diaphragmatic | Passing through oesophageal hiatus | 38 cm |
Clinical relevance: Foreign bodies lodge at these constrictions. Carcinomas arise more commonly at these sites. Endoscopic instruments risk perforation at each narrowing.
4. Wall Layers
The oesophageal wall has four layers (no serosa - unique in the GI tract):
(i) Mucosa
- Lined by non-keratinizing stratified squamous epithelium
- Abruptly changes to columnar epithelium at the stomach - this junction is the Z-line (ora serrata) at the gastro-oesophageal junction
- Squamous = greyish-pink and smooth; gastric = reddish-pink with folds
- Sub-layers: stratified squamous epithelium, lamina propria, muscularis mucosae (longitudinal smooth muscle)
- At rest, mucosa arranged in longitudinal folds (flatten on distension)
(ii) Submucosa
- Loosely connects mucosa to muscle layer
- Contains larger blood vessels, Meissner's plexus (parasympathetic), oesophageal mucous glands (tubulo-acinar - important for acid resistance and oesophageal clearance), lymphocytes, plasma cells
- Elastic fibres close the lumen after peristaltic dilation
(iii) Muscularis Propria (Muscularis Externa)
- Outer longitudinal + inner circular layers
- Longitudinal layer covers the whole oesophagus except the upper 4 cm, where it splits into two bands attaching to the cricoid cartilage
- Key composition by region:
- Upper 1/3: striated (skeletal) muscle only
- Middle 1/3: mixed striated + smooth (transition zone)
- Lower 1/3: smooth muscle only
(iv) Adventitia
- Dense connective tissue with elastin fibres, small vessels, nerves, lymphatics
- Connects oesophagus to neighbouring structures
- No serosa - this means:
- Tumour spread is easy (worsens prognosis)
- Perforation repair is more difficult
5. Blood Supply
| Region | Arterial Supply |
|---|---|
| Cervical | Inferior thyroid artery (from thyrocervical trunk) |
| Thoracic | Segmental branches of descending aorta (~5 oesophageal arteries); bronchial arteries |
| Abdominal | Left gastric artery and left inferior phrenic artery |
- The aortic branches form a vascular chain on the oesophagus, anastomosing above and below - this makes the oesophagus virtually immune to infarction
Venous Drainage:
| Region | Venous Drainage |
|---|---|
| Cervical | Inferior thyroid vein → brachiocephalic veins (systemic) |
| Thoracic | Azygos, hemiazygos, intercostal, bronchial veins (systemic) |
| Abdominal | Left gastric vein → portal vein |
Clinical relevance - Oesophageal Varices: The portal-systemic anastomosis at the lower oesophagus (T8 level) between the left gastric vein (portal) and oesophageal veins (systemic) is the site of oesophageal varices in portal hypertension (e.g. liver cirrhosis). Rupture causes life-threatening haemorrhage.
6. Nerve Supply
Extrinsic innervation:
- Sympathetic: spinal segments T1-T10; regulates smooth muscle and glandular secretion
- Parasympathetic (vagus):
- Upper striated muscle: branches of recurrent laryngeal nerves + postganglionic sympathetic fibres from middle cervical ganglia (via inferior thyroid arteries)
- Lower smooth muscle: oesophageal plexus (vagus + recurrent laryngeal nerves below the lung roots)
Intrinsic (enteric) innervation:
- Auerbach's (myenteric) plexus: ganglia between longitudinal and circular muscle layers - regulates contraction of outer muscle
- Meissner's (submucosal) plexus: ganglia in submucosa - regulates secretion and muscularis mucosae peristalsis
- The two plexi are interconnected
Clinical note: Pain from the oesophagus is poorly localised (due to limited mucosal pain perception - more due to stretching of the outer muscular coat), which explains why referred pain is common.
7. Lymphatic Drainage
Extensive submucosal lymphatic channels allow longitudinal spread within the oesophageal wall itself before draining to regional nodes - explaining skip lesions in carcinoma.
| Region | Lymph Nodes |
|---|---|
| Upper oesophagus | Lower deep cervical nodes, paratracheal nodes, upper mediastinal nodes |
| Thoracic | Posterior mediastinal nodes, tracheobronchial nodes |
| Abdominal | Left gastric nodes, coeliac nodes |
| Any level | May drain directly into the thoracic duct |
Clinical relevance: This pattern of lymphatic drainage means oesophageal carcinoma can spread to cervical, mediastinal, and abdominal nodes simultaneously, requiring wide lymphadenectomy.
Summary Table
| Feature | Detail |
|---|---|
| Length | 25 cm |
| Vertebral levels | C6 (cricoid) to T11 (stomach) |
| Hiatus through diaphragm | T10 |
| Parts | Cervical, Thoracic, Abdominal |
| Narrowings | Cricopharyngeus (15 cm), Aorta (22 cm), Left bronchus (27 cm), Diaphragm (38 cm) |
| Wall layers | Mucosa, Submucosa, Muscularis propria, Adventitia (no serosa) |
| Upper 1/3 muscle | Striated |
| Lower 1/3 muscle | Smooth |
| Arterial supply | Inferior thyroid, aortic branches, left gastric |
| Portal-systemic anastomosis | Left gastric vein (portal) ↔ oesophageal veins (systemic) |
| Sphincters | UOS (cricopharyngeus) and LOS (physiological) |
This is a shared conversation. Sign in to Orris to start your own chat.