
Explain to 1st year mbbs student
Cardiology Prescription - Explained for 1st Year MBBS
The Patient at a Glance
| Detail | Value | What it means |
|---|---|---|
| Name | Mrs. Gangurde Minakshi Vijay | 54-year-old female |
| BP | 104/60 mmHg | Low-normal (target achieved on medication) |
| Pulse | 80 bpm | Normal sinus rate |
| SpO2 | 99% | Normal oxygen saturation |
| BMI | 25.26 kg/m² | Normal (18.5-24.9 is normal; she is just at the upper edge) |
Medical History - Understanding the Background
- Ca (Carcinoma) left breast - treated in March 2022. She had breast cancer.
- Angina (diagnosed May 2019) - chest pain due to reduced blood supply to the heart muscle (coronary artery disease).
- Positive stress test + Angiography (2019) - the angiogram showed a Ramus artery with 70% ostial lesion and "otherwise mild plaques." She chose conservative (medical) therapy instead of a stent or surgery.
- Dyslipidaemia (since 2012) - abnormal blood lipid levels (high LDL cholesterol, etc.). This is what causes plaque buildup in arteries.
- Vitamin B12 deficiency - diagnosed around the same time.
- Family history - Father had MI at 40 years, CABG at 55 years, died at 67 from MI. Mother was hypertensive. Grandmother had breast cancer. This is a very strong family history for cardiovascular disease - a major risk factor.
- Lp(a) - July 2025 - Lipoprotein(a) is a special type of cholesterol particle that carries extra cardiovascular risk.
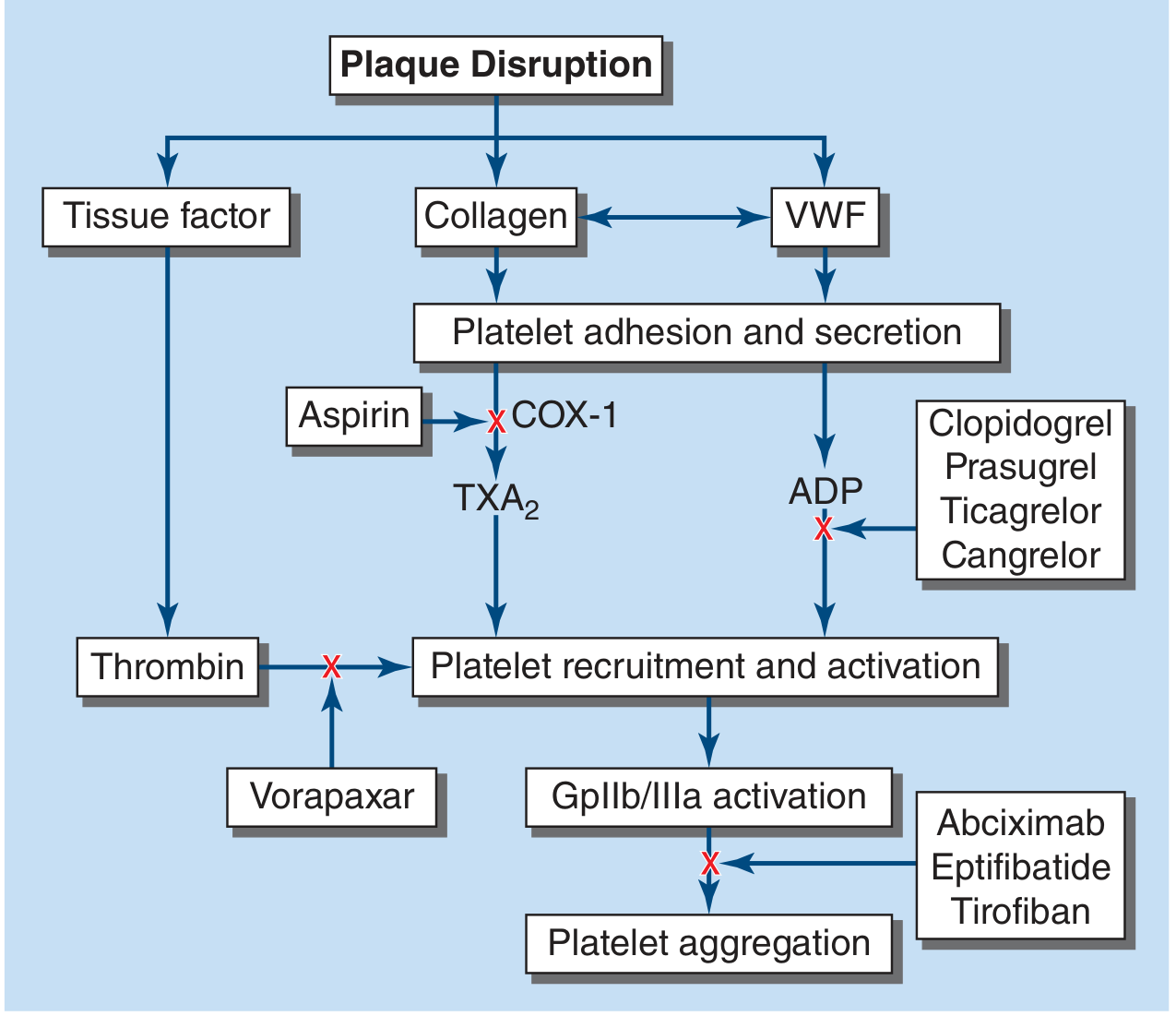
Key concept for 1st year: Atherosclerosis (plaque in arteries) is the root cause here. Risk factors include dyslipidaemia, family history, and age/sex. When a coronary artery gets >70% blocked, it causes angina (chest pain on exertion). A complete blockage causes a heart attack (MI).
The Drugs - One by One
1. Cap. ECOSPRIN AV 75/20 mg
A. Aspirin 75 mg - Antiplatelet
Since platelets have no nucleus, they cannot make new COX-1. The effect lasts for the platelet's entire lifetime (~7-10 days). This is why aspirin is a permanent, irreversible inhibitor.
B. Atorvastatin 10 mg - Statin (lipid-lowering)
2. Tab. TELMA 20 mg
- Angiotensin II is a potent vasoconstrictor. It works by binding AT1 receptors on blood vessels, causing them to constrict and raising BP.
- Telmisartan blocks the AT1 receptor, so angiotensin II cannot exert its effect.
- Result: blood vessels relax → BP falls.
- It also reduces aldosterone release → less sodium and water retention → further BP reduction.
Concept link: The Renin-Angiotensin-Aldosterone System (RAAS) is one of the most important systems you will study. ARBs and ACE inhibitors both target this pathway but at different steps.
3. Tab. THYRONORM 50 mcg
4. Liq. ARACHITOL NANO Oral Solution 5 mL
- Increases calcium and phosphate absorption from the gut
- Maintains bone mineralisation (prevents osteomalacia/rickets)
- Has immunomodulatory effects
5. Tab. SHELCAL HD
6. Tab. ZOSERT 25 mg
Summary Table for Quick Revision
| Drug | Class | Main Target | Why Given Here |
|---|---|---|---|
| Aspirin 75 mg | Antiplatelet | COX-1 → blocks TXA2 | Coronary artery disease (angina, plaque) |
| Atorvastatin 10 mg | Statin | HMG-CoA reductase | Dyslipidaemia, atherosclerosis |
| Telmisartan 20 mg | ARB | AT1 receptor (RAAS) | Hypertension |
| Levothyroxine 50 mcg | Thyroid hormone | Nuclear T3 receptor | Hypothyroidism |
| Cholecalciferol 60,000 IU | Vitamin supplement | Vitamin D receptor | Vitamin D deficiency |
| Calcium + Vit D (Shelcal) | Mineral supplement | GI calcium absorption | Bone protection |
| Sertraline 25 mg | SSRI | SERT (blocks 5-HT reuptake) | Anxiety/low mood |
Prescription Format - How to Read It
- Rx symbol = from Latin "Recipe" (meaning "take"). It is the universal prescription symbol.
- 0-0-1 = Morning-Afternoon-Night dosing. "1" means one tablet/capsule at that time.
- 1-0-0 = Only in the morning.
- 0-1-0 = Only in the afternoon.
- Qty 30 = 30 tablets for one month's supply ("daroj - 1 mahina" = daily for 1 month).
- Allergies: Nitrate headache = She gets headaches with nitrates (like nitroglycerin), so nitrates are avoided even though they are a common angina treatment. This is why she's on conservative medical management without nitrates.
Connecting Dots - The Big Clinical Picture
Coronary Artery Disease
↓
Aspirin (anti-clot) + Atorvastatin (anti-plaque)
Hypertension
↓
Telmisartan (RAAS blockade)
Hypothyroidism
↓
Levothyroxine
Vitamin D + B12 deficiency + post-breast cancer bone risk
↓
Cholecalciferol + Shelcal HD
Anxiety/Depression (cardiac + cancer-related)
↓
Sertraline
Allergy note: She cannot take nitrates (the usual first-line treatment for angina symptoms), which is why her angina is managed with conservative therapy only - hence the statin and aspirin combination managing the underlying disease process rather than just symptoms.
Search for recent 2024-2025 guidelines on secondary prevention after myocardial infarction
"myocardial infarction"[MeSH Terms] AND "secondary prevention"[MeSH Terms]
secondary prevention myocardial infarction guidelines 2024 2025 AHA ACC ESC
secondary prevention myocardial infarction antiplatelet statin beta-blocker RAAS 2025 guidelines
secondary prevention post-MI antiplatelet lipid RAAS beta-blocker colchicine 2025 ACS guideline recommendations
"acute coronary syndrome"[MeSH Terms] AND "secondary prevention"[MeSH Terms]
Secondary Prevention After Myocardial Infarction: 2024-2025 Guidelines & Evidence
The Governing Documents
- 2025 ACC/AHA Guideline for Management of Patients with Acute Coronary Syndromes - Rao SV et al., JACC 2025;85:2135. This is the primary reference for post-MI secondary prevention in the US.
- 2023 ESC Guidelines for ACS - Still current in Europe for 2024-2025 comparisons; the hvt-journal comparative analysis highlights key differences.
1. Antiplatelet Therapy (DAPT) - Major 2025 Updates
Standard of care: Dual Antiplatelet Therapy (DAPT)
- Aspirin + a P2Y12 inhibitor (prasugrel or ticagrelor preferred over clopidogrel after ACS) for at least 12 months in most patients (Class IIB).
- Preferred P2Y12 inhibitors post-ACS: Ticagrelor (90 mg twice daily) or Prasugrel (over clopidogrel), unless contraindicated.
New in 2025: Early De-escalation Strategies
| Strategy | Recommendation Class | Timing |
|---|---|---|
| Switch to ticagrelor monotherapy after stopping aspirin | Class IA | After ≥1 month of DAPT |
| Switch to clopidogrel or prasugrel monotherapy | Class IIb B-R | After ≥1 month |
| DAPT de-escalation (switch from potent P2Y12 → clopidogrel) | Class IIb B-R | After ≥1 month |
ESC vs. ACC/AHA difference: The 2023 ESC guidelines allow P2Y12 monotherapy after just 1 month (Class IA), while ACC/AHA continues to recommend 12 months of full DAPT as the default with de-escalation permitted. The European approach is more permissive for early switch.
P2Y12 vs. Aspirin: New Meta-Analysis Evidence
- P2Y12 inhibitors reduced MI risk by 23% (RR 0.77, 95% CI 0.67-0.89) vs. aspirin monotherapy
- Reduced hemorrhagic stroke risk by 47% (RR 0.53)
- No significant difference in major bleeding or all-cause mortality
2. Lipid-Lowering Therapy - Intensified Targets
2025 ACC/AHA Recommendation
- High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) for all post-MI patients regardless of baseline LDL - Class I, Level A
- LDL target: <70 mg/dL (1.8 mmol/L) for established ASCVD (secondary prevention)
- If LDL remains ≥70 mg/dL on maximum-tolerated statin:
- Add ezetimibe (Class I) - simple, cheap, well-tolerated
- Add PCSK9 inhibitor (evolocumab or alirocumab) - Class IIa if LDL still not at goal
- The guideline specifically mentions LDL reduction targets with an emphasis on an "as low as reasonably achievable" principle for very high-risk patients.
BP Target in Post-MI Patients
- SBP target <130 mmHg for secondary prevention of CVD (Class I)
- DBP 70-80 mmHg when SBP is at target
- Preferred agents: ACE inhibitors, ARBs, or beta-blockers especially if reduced LVEF or diabetes present
3. Beta-Blockers - The Big Controversy in 2024-2025
Traditional recommendation (pre-2023)
What the 2024-2025 evidence says
| Patient Group | Beta-blocker Effect |
|---|---|
| Reduced EF (≤40%) or heart failure | Clear mortality benefit - continue BB |
| Preserved EF, 1-year event-free (no death/MI/HF on BB) | No additional mortality benefit (HR 0.99, 95% CI 0.94-1.06) |
| Preserved EF, post-2010 studies | No mortality benefit; trend toward harm (MACCE HR 1.24, 95% CI 1.01-1.52) |
| Mildly reduced EF (40-50%) | Still derive mortality benefit |
4. RAAS Blockade - ACE Inhibitors / ARBs
| Indication | Recommendation (2025) |
|---|---|
| Post-MI with LVEF ≤40% | ACE inhibitor (or ARB if intolerant) - Class I |
| Post-MI with hypertension, diabetes, or CKD | ACE inhibitor/ARB - Class I |
| Post-MI with normal LVEF, no HF, no DM | Class IIa (benefit less certain) |
| Add MRA (eplerenone/spironolactone) | Class I if LVEF ≤40% + symptoms of HF or DM |
5. Colchicine - The Emerging Evidence (2024-2025)
The Evidence
- Colchicine reduced the composite of CV death, MI, or stroke by 12% (RR 0.88, 95% CI 0.81-0.95, p=0.002)
- MI specifically reduced by 16% (RR 0.84)
- Stroke reduced by 10% (RR 0.90, non-significant)
- GI events increased by 35% (the main side effect)
- No increase in pneumonia, cancer, or non-CV death
2025 ACC/AHA Position on Colchicine
6. Anti-inflammatory Biologics (IL-1/IL-6 Blockers) - Still Experimental
- IL-receptor antagonists (canakinumab, anakinra) and TNF inhibitors
- Evidence remains low to very low certainty for cardiovascular prevention
- Canakinumab (CANTOS trial) showed CV benefit but is not approved/used for secondary prevention due to cost and infection risk
- Not yet recommended in routine guidelines
7. Lifestyle and Non-Pharmacological (DASH Diet - 2025 Cochrane)
- DASH dietary pattern reduces BP, LDL, and cardiovascular risk
- Recommended as part of comprehensive secondary prevention programs
Summary: 2025 Post-MI Secondary Prevention Drug Regimen
| Drug Class | Agent | Duration | Level of Evidence |
|---|---|---|---|
| Antiplatelet | Aspirin 75-100 mg + Ticagrelor/Prasugrel | ≥12 months DAPT; then consider P2Y12 monotherapy | Class I |
| High-intensity statin | Atorvastatin 40-80 mg | Lifelong | Class I |
| ACE inhibitor / ARB | Ramipril, Lisinopril, etc. | Lifelong (especially if LVEF ≤40%, DM, HTN) | Class I |
| Beta-blocker | Metoprolol, Carvedilol | Long-term if LVEF ≤40% or HF; re-evaluate after 1 year if preserved EF | Class I (reduced EF) / IIa (preserved EF) |
| MRA | Eplerenone, Spironolactone | If LVEF ≤40% + HF symptoms or DM | Class I |
| Colchicine | 0.5 mg daily | Consider add-on for residual inflammatory risk | Class IIa (new in 2025) |
| Ezetimibe | 10 mg daily | Add if LDL >70 on statin | Class I |
| PCSK9 inhibitor | Evolocumab / Alirocumab | If LDL still >70 on statin + ezetimibe | Class IIa |
Key 2025 Paradigm Shifts to Know
- DAPT de-escalation is now formally endorsed - switching to P2Y12 monotherapy at 1 month is acceptable in HBR patients (Class IA for ticagrelor switch).
- Beta-blockers are no longer universal lifelong therapy - preserved EF patients should be re-evaluated at 1 year.
- Colchicine enters secondary prevention - the anti-inflammatory strategy (not just lipid-lowering) is now evidence-backed and guideline-supported.
- LDL targets have intensified - "lower is better" with combination therapy (statin + ezetimibe + PCSK9i) now a guideline-endorsed cascade.
- hsCRP is gaining traction as a residual risk marker alongside LDL, potentially guiding colchicine or statin intensification.
Give me a diet plan for minakshi
Indian diet plan coronary artery disease dyslipidemia hypothyroidism breast cancer survivor 2024
Indian anti-inflammatory Mediterranean diet coronary artery disease food recommendations avoid
Personalised Diet Plan for Mrs. Minakshi (54F)
Her Medical Conditions That Shape This Diet
| Condition | Dietary Goal |
|---|---|
| Coronary artery disease (angina, 70% Ramus lesion) | Reduce LDL, reduce inflammation, prevent clot-promoting foods |
| Dyslipidaemia (since 2012) | Lower saturated fat, increase fibre and omega-3 |
| Hypertension (on Telmisartan) | Restrict sodium, increase potassium/magnesium |
| Hypothyroidism (on Thyronorm) | Time meals correctly, limit goitrogens |
| Vitamin D & B12 deficiency | Foods rich in both |
| Breast cancer survivor | Limit red meat, alcohol; moderate soy |
| BMI 25.26 (upper normal) | Maintain or gently reduce weight; avoid refined carbs |
| Nitrate allergy | Avoid high-nitrate foods (beetroot juice, cold meats) |
| Sertraline (SSRI) | Avoid tyramine-heavy foods; no grapefruit |
Calorie Target
- Target: ~1,600 kcal/day (gentle weight maintenance; not aggressive restriction given cardiac status)
- Macros: ~50-55% carbs (whole grain only), ~20-25% protein, ~25-30% fat (mostly unsaturated)
Daily Meal Plan
⏰ 6:30 AM - On Waking (Empty Stomach)
- 1 glass of plain warm water (no milk, no tea - these block levothyroxine absorption)
- Take Thyronorm 50 mcg tablet with plain water only
Critical: Calcium, iron, coffee, and milk all drastically reduce levothyroxine absorption. She must maintain this 30-45 minute gap every day.
🌅 7:00-7:30 AM - Early Morning
- 5 soaked almonds (unsalted) - good source of Vitamin E, healthy fats
- 2 soaked walnuts - best plant-based omega-3 (ALA), anti-inflammatory
- 1 small amla (Indian gooseberry) or 100 ml fresh amla juice - Vitamin C, antioxidant, shown to reduce LDL in Indian studies
🍳 8:00-8:30 AM - Breakfast
| Day | Option |
|---|---|
| Mon/Thu | 2 jowar or bajra rotis + 1 bowl moong dal (thin, low oil) + cucumber salad |
| Tue/Fri | Oats upma (1 cup rolled oats, vegetables, minimal oil, no salt) + 1 cup low-fat buttermilk |
| Wed/Sat | 2 ragi dosas (no maida) + coconut chutney (small portion) + sambar |
| Sun | Poha (1 bowl, made with flattened rice, peas, carrots) + 1 glass low-fat milk |
- 1 cup green tea or plain black tea (no full-fat milk; no sugar) - polyphenols are cardioprotective
- OR 1 glass low-fat milk (not on the same day as Thyronorm - the gap is already covered)
🍎 10:30-11:00 AM - Mid-Morning Snack
- 1 seasonal fruit: guava, papaya, pomegranate, or apple (fibre, potassium, antioxidants)
- Avoid: mango, banana, chickoo (high glycaemic, can raise triglycerides)
- 1 small bowl roasted chana (Bengal gram) - unsalted, good protein + soluble fibre
🍱 1:00-1:30 PM - Lunch (Main Meal)
- ½ plate: Vegetables (2 sabzis - one green leafy, one other)
- ¼ plate: Whole grain carb (brown rice or 2 rotis)
- ¼ plate: Protein (dal, legume, or low-fat curd)
| Component | Best Choices | Avoid |
|---|---|---|
| Grain | Brown rice (½ cup), bajra/jowar roti (2 nos.) | White rice, maida chapati, paratha |
| Dal | Masoor dal, moong dal, rajma (well-cooked) | Butter dal, cream-based gravies |
| Vegetable | Palak, methi, bhindi, lauki, tinda, karela, tomato | Potato fry, puri bhaji |
| Curd | Low-fat dahi 1 small bowl (supports B12 slightly) | Full-fat cream curd |
1 cup brown rice + 1 bowl masoor dal + palak sabzi (cooked in 1 tsp mustard oil) + 1 small bowl low-fat dahi + 1 medium salad (cucumber, tomato, onion with lemon - no salt)
☕ 4:00-4:30 PM - Evening Snack
- Option A: 1 bowl sprouts salad (moong, chana) with lemon, cumin, green chilli - excellent for cholesterol and B12 absorption
- Option B: Roasted makhana (fox nuts, 1 small bowl) - heart-friendly, low calorie
- Option C: 1 slice whole grain toast with 1 tsp flaxseed powder stirred into low-fat curd
🌙 7:30-8:00 PM - Dinner (Light)
| Day | Dinner |
|---|---|
| Mon/Thu | 2 jowar rotis + lauki/tinda sabzi (low oil) + thin dal soup |
| Tue/Fri | Vegetable daliya (broken wheat khichdi) + salad |
| Wed/Sat | 1 bowl mixed vegetable soup (no cream) + 2 small rotis |
| Sun | Moong dal khichdi (rice + dal cooked together, 1 tsp ghee only) + steamed vegetables |
💊 9:00-9:30 PM - With/After Dinner (Medicine Time)
- Ecosprin AV (Aspirin + Atorvastatin) - with or just after dinner (reduces GI irritation from aspirin; atorvastatin is best at night)
- Zosert 25 mg (Sertraline) - after dinner
- Shelcal HD - already taken at afternoon lunch (calcium needs food for absorption)
Weekly Special Items to Include
| Food | Why | How Often |
|---|---|---|
| Flaxseeds (alsi) | Best plant omega-3, lowers LDL, anti-inflammatory | Daily (1 tbsp ground, add to roti dough or curd) |
| Methi (fenugreek) seeds | Lowers cholesterol, helps glycaemic control | 3-4x/week (soak overnight, eat with water in morning OR add to roti) |
| Garlic (1-2 raw cloves) | Allicin - reduces LDL and BP | Daily (in cooking or chew raw) |
| Turmeric + black pepper | Curcumin is anti-inflammatory (relevant for both CAD and cancer) | Daily in cooking |
| Fatty fish (mackerel/rohu/surmai) | Omega-3 EPA/DHA - cardioprotective | 2x/week if she consumes non-veg |
| Oats (rolled, not instant) | Beta-glucan soluble fibre - proven LDL reduction | 3-4x/week at breakfast |
| Pomegranate | Lowers LDL oxidation, anti-inflammatory, anti-cancer | 3-4x/week |
Foods to AVOID or STRICTLY LIMIT
❌ Avoid Completely
| Food | Reason |
|---|---|
| Vanaspati / dalda / margarine | Trans fats - worsen dyslipidaemia, promote atherosclerosis |
| Pickles, papads, processed snacks | High sodium - worsens hypertension |
| Full-fat cream, butter in excess | Saturated fat raises LDL |
| Maida (refined flour) products - bread, biscuits, naan | Raises triglycerides, worsens dyslipidaemia |
| Cold meats, sausages, processed meat | Nitrates trigger her allergy + raise CV risk |
| Alcohol | Raises triglycerides + interacts with sertraline + breast cancer risk |
| Coconut oil / palm oil in large amounts | Saturated fat |
| Fried foods - puri, bhajia, pakoda | Trans fats from reheated oil |
⚠️ Limit (Not Eliminate)
| Food | Limit To | Reason |
|---|---|---|
| Ghee | ½ tsp/day max | Saturated fat, but some ghee is culturally important - moderate is OK |
| Red meat (mutton) | <2 servings/week | Saturated fat + her cancer history |
| Sugar/jaggery/honey | <2 tsp/day | Raises triglycerides |
| Coconut (fresh) | Small amounts | Saturated fat |
| Salt | <1,500 mg/day (about ½ tsp total) | Hypertension control with Telmisartan |
| Soy products (tofu, soy milk) | Moderate (1 serving/day) | Phytoestrogens - safe in moderation for breast cancer survivors, but not excess |
Special Considerations for Her Conditions
🫀 For Coronary Artery Disease (70% Ramus lesion)
- Strictly no re-heated or repeatedly heated cooking oils - these form trans fats and neo-formed contaminants, especially dangerous in Indians with existing CAD per the Indian dyslipidaemia guidelines
- Use cold-pressed mustard oil (1-2 tsp/meal) - rich in MUFA and ALA omega-3, best for Indian cooking
- The Indian-adapted Mediterranean diet for CAD patients (George Institute/AIIMS 2024) recommends: fish ≥2 serves/week, legumes daily, nuts daily, vegetables 2 serves/meal, limited red meat, no processed meat
🦋 For Hypothyroidism (Thyronorm)
- Goitrogenic foods (raw cruciferous vegetables like cabbage, cauliflower, broccoli, radish) are fine when cooked - cooking deactivates goitrogens. Do not eat these raw in large amounts.
- No soy protein isolate within 4 hours of Thyronorm tablet - soy can reduce T4 absorption
- Adequate iodine - use iodised salt (within the low-sodium limit)
🩺 For Vitamin D & B12 Deficiency
- She already takes Arachitol Nano (60,000 IU monthly) and Shelcal HD - dietary sources are a bonus
- Vitamin D food sources: Low-fat milk (2 glasses/day), eggs (if non-veg), sun-dried mushrooms
- B12 food sources: Low-fat dahi, low-fat milk, eggs, fish - critical since she is documented B12 deficient
🎗️ For Breast Cancer Survivor
- Cruciferous vegetables (cooked) - broccoli, cabbage, cauliflower, broccoli sprouts - contain indole-3-carbinol, which has anti-oestrogenic and anti-cancer properties
- Berries, pomegranate, amla - high antioxidant, anti-inflammatory
- Limit refined sugar and refined carbs - these are pro-inflammatory and linked to cancer recurrence
- Moderate soy is safe (1 serving/day) - meta-analyses show no harm and possibly benefit in breast cancer survivors
💊 Drug-Food Interactions to Know
| Drug | Food Interaction | Action |
|---|---|---|
| Thyronorm (Levothyroxine) | Calcium, iron, coffee, soy, milk | 30-45 min gap before food/supplements |
| Shelcal (Calcium) | Iron absorption competition | Take with food (lunch), not with iron-rich foods at same time |
| Ecosprin (Aspirin) | Empty stomach causes GI irritation | Always take with food |
| Zosert (Sertraline) | Grapefruit juice inhibits metabolism | Avoid grapefruit entirely |
| Telmisartan | High-potassium foods raise K+ risk if combined with MRA | Bananas, oranges fine in moderation |
Cooking Oil Recommendation
| Oil | Amount/Day | Notes |
|---|---|---|
| Cold-pressed mustard oil | 3-4 tsp total/day | Best for Indian cooking - high MUFA + omega-3 ALA |
| Virgin coconut oil | Occasional, very small (½ tsp) | Use sparingly due to saturated fat |
| No vanaspati/dalda/refined palm oil | Zero | Avoid |
Quick Weekly Overview
| Day | Breakfast | Lunch | Dinner |
|---|---|---|---|
| Mon | Oat upma + green tea | Brown rice + masoor dal + palak sabzi + dahi | Jowar roti + lauki sabzi + dal soup |
| Tue | Ragi dosa + sambar | Bajra roti + rajma + methi sabzi + salad | Daliya vegetable khichdi |
| Wed | Bajra roti + moong dal + salad | Brown rice + arhar dal + bhindi + dahi | Vegetable soup + 2 rotis |
| Thu | Oats upma + amla juice | Jowar roti + chana dal + mixed vegetable sabzi | Moong dal khichdi + vegetables |
| Fri | Poha + buttermilk | Brown rice + sambhar + green sabzi | Ragi roti + thin dal + salad |
| Sat | Ragi dosa + coconut chutney | Mixed dal khichdi + dahi + cucumber | Jowar roti + bottle gourd sabzi |
| Sun | Whole grain toast + flaxseed dahi | Brown rice + palak paneer (low fat) + salad | Light moong soup + 2 rotis |
At a Glance: The Golden Rules for Minakshi
- Take Thyronorm first thing - 30-45 min before ANY food or drink (except plain water)
- Take Ecosprin AV and Zosert always with or after dinner - never on empty stomach
- Take Shelcal HD at lunch, not dinner (calcium competes with Thyronorm absorption)
- Cook in mustard oil only - small quantity, never reheated
- No salt at the table - cook with minimal salt
- 2 handfuls of nuts + seeds daily (almonds, walnuts, flaxseeds)
- At least 2 servings of fish per week (if non-vegetarian) for omega-3
- Finish dinner by 8 PM - light meal only
- Walk 30 minutes daily (her cardiologist's conservative therapy relies heavily on lifestyle; she cannot take nitrates for angina symptoms)
- No grapefruit - interacts with Sertraline
2.why
Ecosprin AV (Aspirin 75 mg + Atorvastatin 10 mg) - With Food
Aspirin - Why NOT on empty stomach?
-
Direct topical injury - Aspirin is a weak acid (acetylsalicylic acid). On an empty stomach, it remains in unionised (non-polar) form in the acidic gastric environment, crosses easily into gastric mucosal cells, and becomes ionised (trapped) inside them - this is called ion trapping. It then disrupts the mucosal barrier from within.
-
COX-1 inhibition reduces prostaglandin E2 (PGE2) - Normally, PGE2 produced via COX-1 in the stomach:
- Stimulates mucus secretion
- Stimulates bicarbonate secretion
- Maintains mucosal blood flow
Aspirin irreversibly blocks COX-1 → PGE2 falls → mucus and bicarbonate drop → the stomach lining loses its protective coating → acid attacks the naked mucosa → erosion, gastritis, peptic ulcer, and bleeding risk.
- Food dilutes the aspirin concentration in the stomach
- Food stimulates acid-buffering mechanisms
- Gastric emptying is slowed, reducing direct mucosal contact time
- Risk of GI irritation is significantly reduced
Note: Even enteric-coated aspirin (like Ecosprin) doesn't fully eliminate this risk - the systemic COX-1 inhibition still reduces mucosal PGE2 via the bloodstream. Food still helps.
Atorvastatin - Why at night?
- Cholesterol synthesis follows a circadian rhythm - the rate-limiting enzyme HMG-CoA reductase is most active between midnight and 2 AM
- Atorvastatin has a half-life of ~14 hours (longer than older statins like simvastatin), so timing matters less than for short-acting statins, but nighttime dosing still achieves slightly better LDL reduction
- Taking it with food also reduces mild GI side effects (nausea, dyspepsia) that some patients experience
Zosert (Sertraline 25 mg) - With Food
- On an empty stomach, sertraline is absorbed erratically and peak plasma concentration (Cmax) is lower
- With food, absorption is more consistent and complete, giving a more stable therapeutic effect
- Additionally, sertraline can cause nausea when taken on an empty stomach - this is one of the most common reasons patients stop SSRIs early; taking it with food reduces this significantly
- Sertraline commonly causes mild sedation or drowsiness in the initial weeks (especially at the start of treatment) - nighttime dosing turns this side effect into an advantage
- Avoids daytime drowsiness that could affect her work as a teacher
- Some patients experience mild activating effects instead (insomnia) - if that happens, the timing can be shifted to morning
In Short
| Drug | Reason for "with food" |
|---|---|
| Aspirin | Protects gastric mucosa - reduces ion trapping + preserves some PGE2 protective effect |
| Atorvastatin | Maximises LDL reduction (nighttime = peak cholesterol synthesis); reduces GI side effects |
| Sertraline | Increases bioavailability by ~30%; prevents nausea; nighttime dosing reduces daytime drowsiness |
70 percent ramus lesion
ramus intermedius coronary artery anatomy 70% ostial lesion significance angiography
Ramus Intermedius - 70% Ostial Lesion: Explained
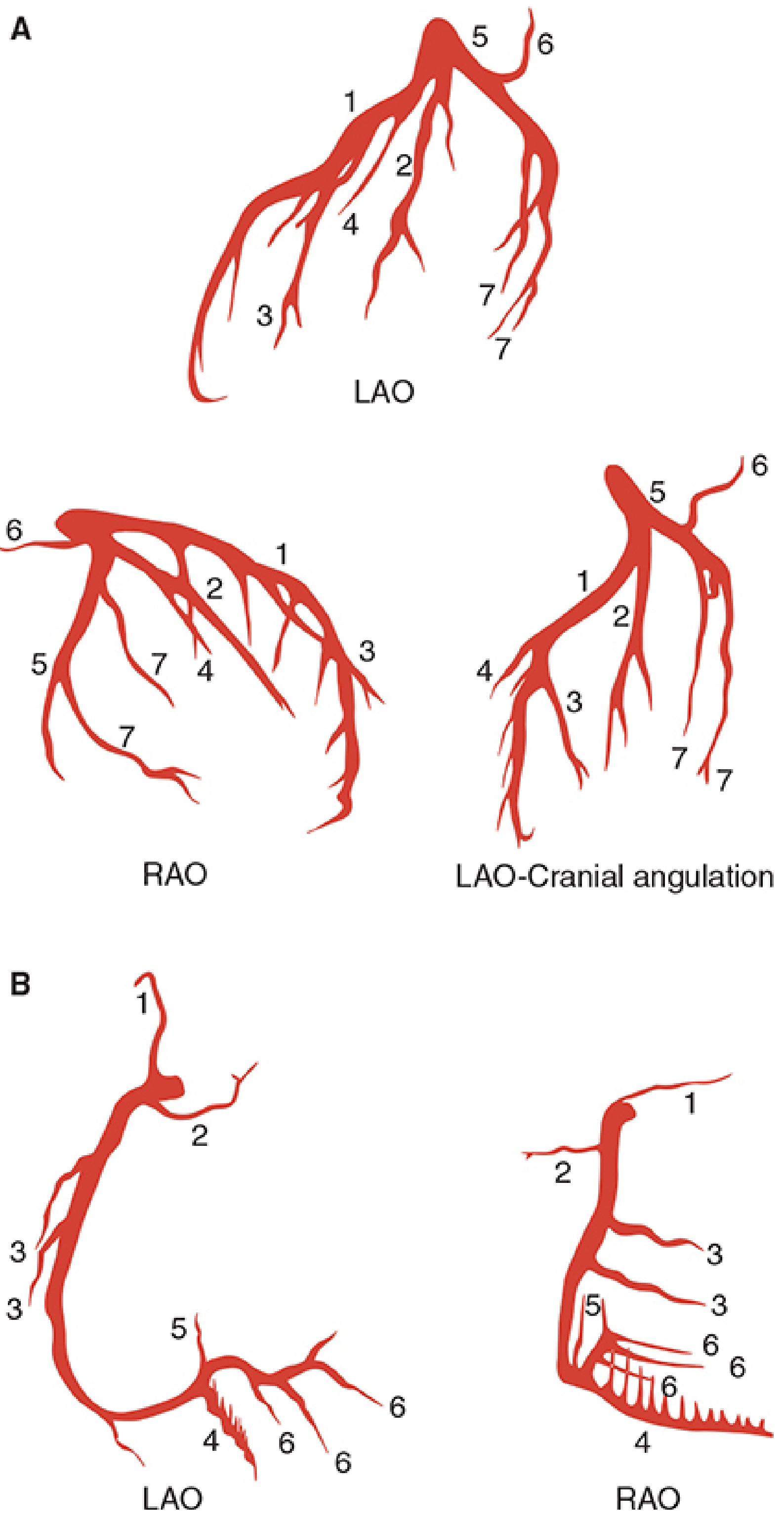
Step 1: Normal Coronary Artery Anatomy First
AORTA
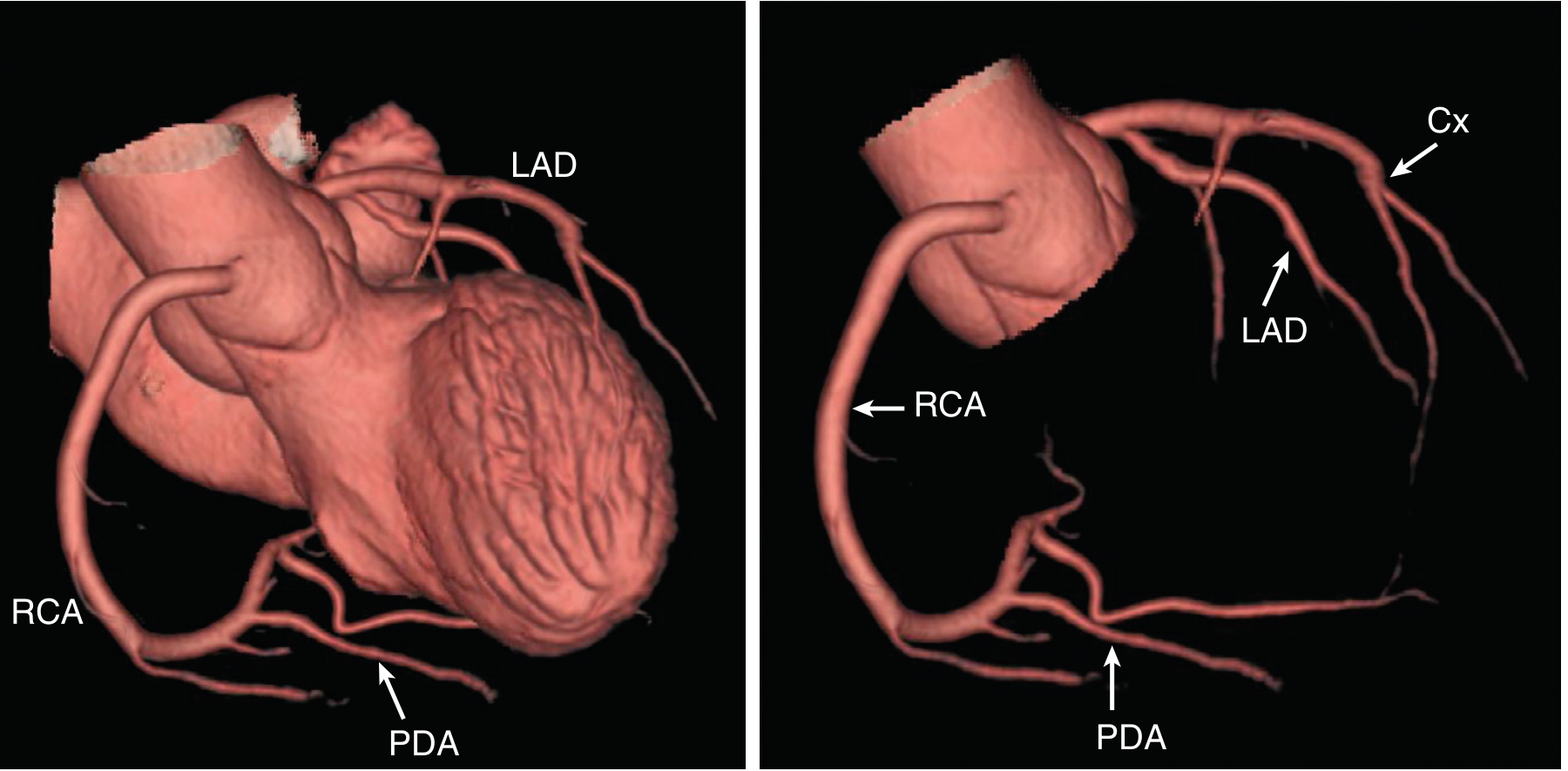
├── Right Coronary Artery (RCA)
│ └── Posterior Descending Artery (PDA) [in 80% - "right dominant"]
│
└── Left Main Coronary Artery (LMCA)
├── Left Anterior Descending (LAD) → anterior wall + septum
└── Left Circumflex (LCx) → lateral wall
Step 2: What is the Ramus Intermedius?
Left Main Coronary Artery (LMCA)
├── LAD (Left Anterior Descending)
├── RAMUS INTERMEDIUS ← the "extra" artery
└── LCx (Left Circumflex)
- Ramus medianus (same vessel, different name)
- Intermediate artery
What does the Ramus supply?
Step 3: What is an "Ostial" Lesion?
LMCA
│
├── LAD
├── RAMUS ←── [PLAQUE HERE at origin = OSTIAL LESION]
└── LCx
- They are technically difficult to stent (the stent can block the adjacent branch)
- They are hemodynamically critical - blockage here affects the entire downstream vessel
- They are prone to elastic recoil after balloon angioplasty
- They are harder to visualise correctly on angiography (the vessel origin may be foreshortened)
Step 4: What Does "70% Lesion" Mean?
Normal vessel lumen: ████████████ (100%)
70% stenosis: ████ (only 30% of lumen is open)
The critical threshold: ≥70% = Hemodynamically significant
| % Stenosis | Classification | Significance |
|---|---|---|
| <50% | Mild | Usually non-obstructive; medically managed |
| 50-69% | Moderate | May be significant; needs functional testing (FFR) |
| ≥70% | Severe / Significant | Hemodynamically obstructive - causes ischaemia |
| ≥90% | Critical | Severely restricted flow |
| 100% | Total occlusion | No flow = territory at risk of infarction |
Step 5: Why Was Conservative (Medical) Therapy Chosen?
Arguments for medical management (her cardiologist's choice):
- Only one vessel significantly affected (ramus) - the LAD and LCx have only mild plaques
- Functional significance not confirmed - at exactly 70%, a FFR (Fractional Flow Reserve) test ideally determines whether flow is truly impaired. FFR <0.8 confirms significance; at borderline stenosis, FFR sometimes guides against stenting
- Ostial location makes PCI technically risky - stenting the ramus ostium can jail the LAD or LCx
- She prefers conservative therapy - patient preference is a valid factor
- Her symptoms were stable angina (not acute MI or unstable angina) - medical therapy is non-inferior to PCI for stable angina in many trials (COURAGE trial, ISCHEMIA trial)
What medical therapy does in this setting:
| Drug | Role in her 70% Ramus Lesion |
|---|---|
| Aspirin 75 mg | Prevents platelet thrombus forming on the plaque surface |
| Atorvastatin 10 mg | Stabilises the plaque, prevents it from rupturing or growing |
| Telmisartan | Lowers BP → reduces shear stress on the vessel wall |
| No nitrates | She is allergic (nitrate headache) - nitrates would normally be used for symptom relief in angina |
The Complete Picture for Minakshi
Dyslipidaemia (since 2012)
↓
LDL deposits in vessel walls → atherosclerotic plaques
↓
Ramus intermedius: 70% plaque at its origin (ostium)
Mild plaques elsewhere (LAD, LCx - not yet significant)
↓
Reduced blood flow to anterolateral LV wall
↓
On exertion → demand exceeds supply → ANGINA
At rest → adequate flow → no symptoms
↓
Positive stress test (2019): confirms ischaemia on exertion
Angiography (2019, Wockhardt): confirms 70% ostial ramus lesion
↓
Decision: Conservative medical therapy
(Aspirin + Statin + ARB instead of stent)
Key concept to remember: A 70% coronary stenosis does NOT mean the heart is in danger at rest. At rest, even a 70% narrowed vessel can deliver enough blood. It is during stress/exertion when oxygen demand rises that the narrowing becomes a bottleneck - this is the mechanism of stable angina. Only when a plaque ruptures (unstable angina / NSTEMI / STEMI) does the situation become a true emergency.