Difference between cholecystitis and cholelithiasis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough comparison based on multiple authoritative medical textbooks.
Cholelithiasis vs. Cholecystitis
Definitions
| Cholelithiasis | Cholecystitis | |
|---|---|---|
| What it is | Presence of stones (calculi) within the gallbladder | Inflammation of the gallbladder |
| Core concept | A structural/metabolic condition | An inflammatory/infectious process |
Relationship Between the Two
More than 95% of biliary tract disease is attributable to gallstones. Cholelithiasis is the primary risk factor for cholecystitis - gallstones are found in 90-95% of patients with cholecystitis. However, they are distinct conditions: you can have gallstones for years without ever developing inflammation, and a minority of cholecystitis cases (~5-12%) occur without any stones at all (acalculous cholecystitis).
Cholelithiasis (Gallstones)
Types of Stones
1. Cholesterol stones (90% in the US/Western Europe)
- Contain >50% crystalline cholesterol monohydrate
- Form when bile becomes supersaturated with cholesterol relative to bile acids and phospholipids
2. Pigment stones
- Black stones - form in the gallbladder; associated with chronic hemolytic anemias (sickle cell, hereditary spherocytosis), older age
- Brown stones - associated with biliary infection; can form anywhere in the biliary tree
Risk Factors ("4 Fs" mnemonic)
- Female sex and female sex hormones (estrogen, OCP, pregnancy)
- Fat (obesity, metabolic syndrome, rapid weight loss)
- Forty (increasing age)
- Fertile (multiparity)
- Also: Native American descent (Pima/Hopi/Navajo), Crohn's disease, cystic fibrosis with pancreatic insufficiency, TPN, drugs (clofibrate, ceftriaxone)
Clinical Features
- Most patients are asymptomatic - only ~25.8% develop biliary colic at 10 years; complications occur in ~3% at 10 years
- Biliary colic: dull, steady RUQ or epigastric pain (not truly "colicky"), radiating to the right scapula/shoulder; nausea/vomiting; triggered by gallbladder contraction against obstructed cystic duct
- Patients appear well, no fever, no guarding/rebound
- No leukocytosis, liver enzymes usually normal
Cholecystitis (Gallbladder Inflammation)
Types
1. Acute Calculous Cholecystitis (most common, ~88-95% of cases)
- Triggered by a stone obstructing the gallbladder neck or cystic duct
- Sequence: obstruction → increased intraluminal pressure → mucosal ischemia → phospholipases hydrolyze biliary lecithin to toxic lysolecithin → disruption of the protective mucus layer → detergent action of bile salts → prostaglandin release → inflammation
- Bacterial superinfection common (E. coli most frequent; anaerobes in up to 40%)
2. Acute Acalculous Cholecystitis (5-12% of cases)
- Caused by gallbladder stasis and ischemia without stones
- Seen in critically ill patients: post-major surgery, severe trauma, burns, sepsis
- Carries a high mortality rate due to underlying illness
3. Chronic Cholecystitis
- May follow repeated acute attacks or develop silently
- Almost always associated with gallstones, but supersaturation of bile (rather than stones per se) appears to drive the inflammation
- E. coli and enterococci cultured in ~1/3 of cases
Clinical Features
- Pain - RUQ pain that starts colicky then becomes constant (distinguishes from uncomplicated biliary colic)
- Fever, nausea, vomiting
- Murphy's sign - inspiratory arrest on deep palpation of RUQ
- Guarding and rebound tenderness (peritoneal signs)
- Leukocytosis (though absent in ~50% of cases)
- Mild elevation of LFTs, alkaline phosphatase; markedly elevated lipase suggests concurrent pancreatitis
Head-to-Head Comparison
| Feature | Cholelithiasis | Cholecystitis |
|---|---|---|
| Definition | Gallstones present | Gallbladder inflamed |
| Cause | Cholesterol/pigment supersaturation | Cystic duct obstruction (usually by a stone) |
| Symptoms | Often none; intermittent biliary colic | Persistent RUQ pain, fever, nausea/vomiting |
| Pain character | Dull, intermittent, self-limiting | Constant, progressive |
| Fever | Absent | Present |
| Murphy's sign | Absent | Positive |
| Guarding/Rebound | Absent | Present (peritoneal irritation) |
| WBC | Normal | Leukocytosis (often with bandemia) |
| LFTs | Normal | May be mildly elevated |
| Ultrasound | Echogenic stones with posterior shadowing | Stones + thickened GB wall (>3 mm) + pericholecystic fluid + sonographic Murphy sign |
| Treatment | Elective; asymptomatic = watchful waiting; symptomatic = cholecystectomy | Urgent cholecystectomy, IV antibiotics, fluids |
| Complications | Cholecystitis, choledocholithiasis, pancreatitis, Mirizzi syndrome | Empyema, perforation, fistula, Mirizzi syndrome |
Ultrasound Findings
The image below shows what acute cholecystitis looks like on ultrasound - note the echogenic stones inside the gallbladder lumen, the thickened gallbladder wall (GBW), and pericholecystic free fluid (FF):
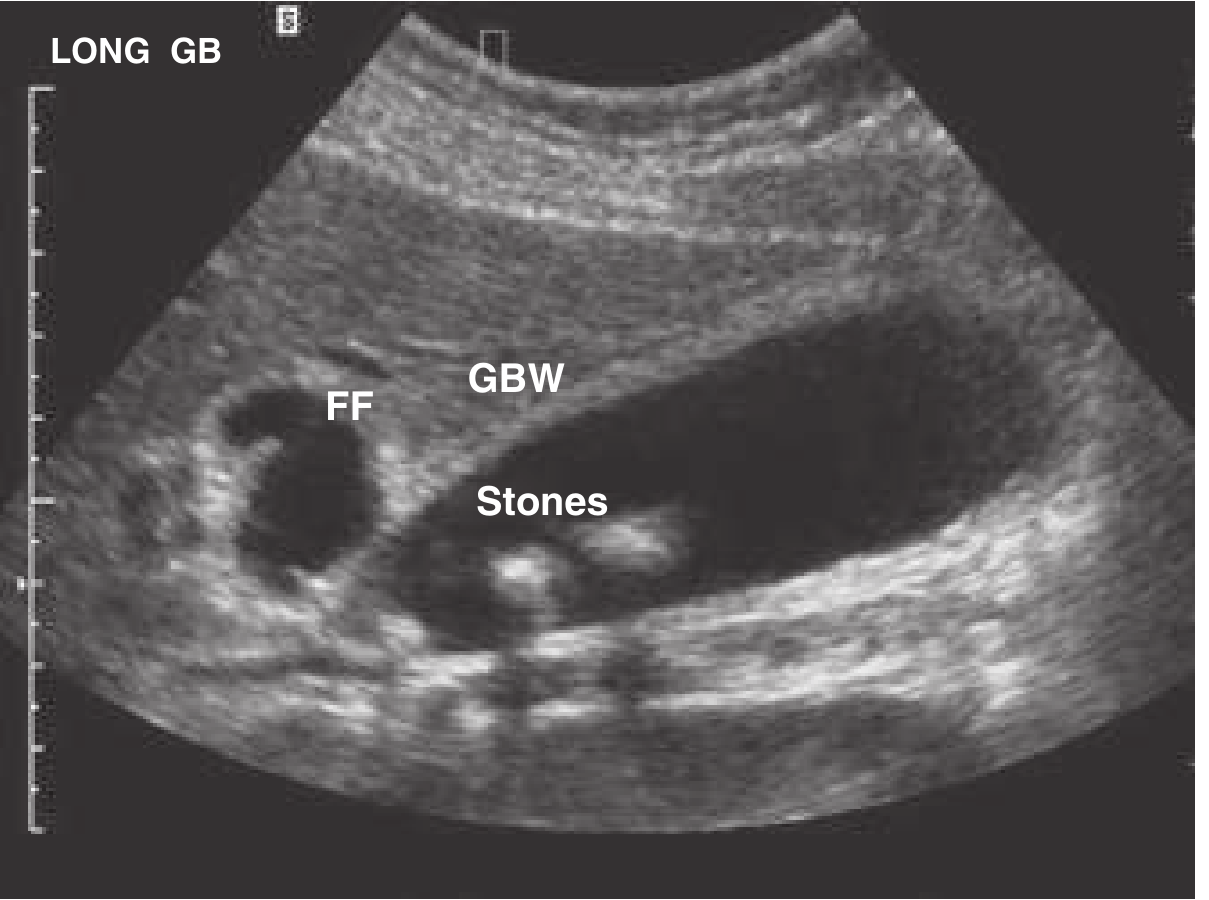
Fig. 76.22 - Gallbladder with gallstones (Stones), thickened gallbladder wall (GBW), and pericholecystic fluid (FF). Together with a sonographic Murphy sign, these findings constitute the diagnosis of cholecystitis.
When all four signs are present (stones + thickened wall + pericholecystic fluid + sonographic Murphy sign), the positive predictive value for cholecystitis exceeds 90%.
Complications Worth Knowing
- Choledocholithiasis - stone migrates to common bile duct → obstructive jaundice, cholangitis (Charcot's triad), pancreatitis
- Empyema - pus fills the gallbladder
- Gangrenous cholecystitis - ischemic necrosis of the wall
- Perforation - can lead to peritonitis or cholecystoenteric fistula
- Gallstone ileus - large stone erodes into bowel, causes small bowel obstruction
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Rosen's Emergency Medicine; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.