teach me diabetes mellitus briefly with types and with complications specially focu on diabetic foot thier examination investigation and management with classfifcation get materal from harrison and more other books if relevant make it precise detailed and relavant
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-structured answer. Here it is:
Diabetes Mellitus - A Comprehensive Overview
Sources: Harrison's Principles of Internal Medicine 22E (2025), Bailey & Love's Short Practice of Surgery 28E, Current Surgical Therapy 14E
1. DEFINITION
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Chronic hyperglycemia damages multiple organ systems, particularly eyes, kidneys, nerves, heart, and blood vessels.
2. CLASSIFICATION OF DIABETES MELLITUS
Type 1 DM (T1DM)
- Pathogenesis: Autoimmune destruction of pancreatic beta cells leading to absolute insulin deficiency
- Autoantibodies: Islet cell antibodies (ICA), anti-GAD65, anti-insulin, anti-IA-2, anti-ZnT8
- Onset: Usually childhood/adolescence but can occur at any age
- Risk of DKA: High - the hallmark acute complication
- Treatment: Insulin is mandatory; no alternative
- Subtypes: Immune-mediated (1A) and idiopathic (1B)
Type 2 DM (T2DM)
- Pathogenesis: Insulin resistance + progressive beta-cell dysfunction (relative insulin deficiency)
- Risk factors: Obesity (especially central), physical inactivity, family history, older age, ethnicity
- Onset: Usually after age 40, but rising in youth due to obesity epidemic
- Long asymptomatic period - many have complications at diagnosis
- Treatment: Lifestyle modification, oral agents, eventually insulin in many
Gestational DM (GDM)
- Any degree of glucose intolerance with onset or first recognition during pregnancy
- Risk of developing T2DM later (~50% within 10 years)
Other Specific Types
| Type | Cause/Example |
|---|---|
| Pancreatic DM (Type 3c) | Pancreatitis, pancreatic cancer, cystic fibrosis, hemochromatosis |
| MODY (Maturity Onset DM of the Young) | Single gene mutations (GCK, HNF-1α, HNF-4α, etc.) |
| Drug-induced | Glucocorticoids, antipsychotics, tacrolimus, thiazides |
| Immune checkpoint-related DM | Anti-PD-1/PD-L1 therapy - rapid onset with DKA |
| Endocrine DM | Cushing's, acromegaly, pheochromocytoma, glucagonoma |
| Genetic insulin resistance syndromes | Lipodystrophy, leprechaunism |
(Harrison's 22E, Chapter 415)
3. DIAGNOSTIC CRITERIA
(ADA 2024 criteria)
| Test | Diagnostic Value |
|---|---|
| Fasting plasma glucose (FPG) | ≥ 126 mg/dL (7.0 mmol/L) |
| 2-h plasma glucose (75g OGTT) | ≥ 200 mg/dL (11.1 mmol/L) |
| HbA1c | ≥ 6.5% (48 mmol/mol) |
| Random glucose + symptoms | ≥ 200 mg/dL (11.1 mmol/L) |
Pre-diabetes: FPG 100-125 mg/dL, 2h OGTT 140-199 mg/dL, HbA1c 5.7-6.4%
4. PATHOPHYSIOLOGY IN BRIEF
- T1DM: Autoimmune T-cell mediated destruction of beta cells → zero insulin → unopposed glucagon → hyperglycemia + ketosis
- T2DM: Insulin resistance in muscle/liver/fat → compensatory hyperinsulinemia → eventual beta-cell exhaustion → progressive hyperglycemia
- Chronic hyperglycemia activates four damaging pathways:
- Polyol pathway (sorbitol accumulation)
- Advanced glycation end-products (AGEs)
- Protein kinase C activation
- Hexosamine pathway
- These pathways damage the microvasculature (basement membrane thickening, pericyte loss) and accelerate atherosclerosis
5. COMPLICATIONS OF DIABETES MELLITUS
(Harrison's 22E, Chapter 417)
A. ACUTE COMPLICATIONS
Diabetic Ketoacidosis (DKA)
- Primarily T1DM; absolute insulin deficiency
- Triad: hyperglycemia + ketonemia + metabolic acidosis
- Glucose typically >250 mg/dL, pH <7.3, bicarbonate <15 mEq/L, ketones elevated
- Precipitants: infection, missed insulin, new onset T1DM
- Management: IV fluids, insulin infusion (0.1 units/kg/hr), potassium replacement, treat precipitant
Hyperosmolar Hyperglycemic State (HHS)
- Primarily T2DM; enough residual insulin to prevent ketosis
- Glucose >600 mg/dL, plasma osmolality >320 mOsm/kg, profound dehydration, altered sensorium
- Management: Aggressive fluid replacement (main priority), insulin, electrolyte correction
Hypoglycemia
- Most common acute complication of insulin/sulfonylurea therapy
- Glucose <70 mg/dL; symptoms: sweating, tremor, tachycardia, confusion
- Treatment: 15-20g fast-acting carbs (conscious); IM glucagon or IV dextrose (unconscious)
B. CHRONIC COMPLICATIONS
Microvascular Complications
1. Diabetic Retinopathy
- Leading cause of new blindness in adults
- Progression: Non-proliferative (NPDR) → Proliferative (PDR) → macular edema
- NPDR features: microaneurysms, dot-blot hemorrhages, hard exudates, soft exudates (cotton-wool spots)
- PDR features: neovascularization (NVD/NVE), vitreous hemorrhage, traction retinal detachment
- Treatment: Glycemic + BP control; laser photocoagulation; anti-VEGF injections for macular edema; vitrectomy
2. Diabetic Nephropathy
- Most common cause of end-stage renal disease (ESRD)
- Progression: hyperfiltration → microalbuminuria (30-300 mg/day) → macroalbuminuria → declining GFR → ESRD
- Treatment:
- Glycemic control (HbA1c <7%)
- BP target <130/80 mmHg
- ACE inhibitor or ARB (first-line, renoprotective)
- SGLT-2 inhibitors (reduce CKD progression - e.g., empagliflozin, dapagliflozin)
- Finerenone (mineralocorticoid receptor antagonist)
3. Diabetic Neuropathy
- Most common complication overall; affects >50% of long-standing diabetics
- Types:
- Distal symmetric polyneuropathy (DSPN): "stocking-glove" distribution; loss of sensation, pain, numbness; most common type
- Autonomic neuropathy: Gastroparesis, orthostatic hypotension, resting tachycardia, neurogenic bladder, erectile dysfunction, Charcot foot
- Painful neuropathy: Burning, electric-shock like pain, worse at night
- Mononeuropathy: CN III, VI palsy; carpal tunnel
- Amyotrophy (Bruns-Garland): Proximal asymmetric lower limb weakness and pain
- Treatment: Glycemic control; pregabalin/gabapentin; duloxetine/amitriptyline; topical capsaicin; SNRIs
Macrovascular Complications
Atherosclerotic Cardiovascular Disease (ASCVD)
- 2-4x increased risk of MI, stroke, and cardiovascular death
- DM accelerates atherosclerosis via dyslipidemia, hypertension, endothelial dysfunction
- Management: Statins (all T2DM patients with ASCVD), aspirin, GLP-1 RA or SGLT-2 inhibitors with proven CV benefit
Peripheral Arterial Disease (PAD)
- Accelerated atherosclerosis of lower limb arteries; DM is a major risk factor
- Often presents as claudication or critical limb-threatening ischemia (CLTI)
- Contributes critically to diabetic foot
Cerebrovascular Disease
- Increased risk of ischemic stroke
Heart Failure
- Diabetic cardiomyopathy independent of CAD
- SGLT-2 inhibitors reduce hospitalizations for heart failure
Other Complications
- Gastrointestinal: gastroparesis (delayed emptying), diarrhea
- Genitourinary: neurogenic bladder, erectile dysfunction
- Infections: increased susceptibility (impaired neutrophil function)
- Dermatologic: necrobiosis lipoidica, acanthosis nigricans, diabetic dermopathy
- Cheiroarthropathy (limited joint mobility), periodontal disease, hearing loss
6. THE DIABETIC FOOT
Epidemiology & Pathophysiology
- ~1 in 4 diabetic patients will develop a foot complication during their lifetime
- 15-20% of diabetic foot ulcers (DFUs) result in lower extremity amputation (LEA)
- 85% of all amputations are preceded by DFU
- Annual incidence of foot complications: 1-2% per year
The diabetic foot results from a triad:
- Peripheral neuropathy (sensorimotor + autonomic) - loss of protective sensation, altered gait, dry/cracked skin
- Peripheral arterial disease (ischemia) - impaired wound healing and tissue survival
- Infection - immune defects, hyperglycemia impair bacterial killing; infection spreads rapidly to deep structures
(Current Surgical Therapy 14E)
CLASSIFICATION OF DIABETIC FOOT ULCERS
Wagner Classification (Simple, widely used)
| Grade | Description |
|---|---|
| 0 | Intact skin; pre-ulcerative lesion (callus, deformity) |
| 1 | Superficial ulcer (skin only) |
| 2 | Deep ulcer to tendon/capsule/bone without abscess |
| 3 | Deep ulcer with abscess, osteomyelitis, or joint sepsis |
| 4 | Localized gangrene (toe or forefoot) |
| 5 | Gangrene of entire foot requiring amputation |
University of Texas Classification (UT)
- Two axes: Depth (0-3) and Stage (A=clean, B=infected, C=ischemic, D=infected+ischemic)
SINBAD Classification
- Six variables: Site, Ischemia, Neuropathy, Bacterial infection, Area, Depth
- Each scores 0-1, total 0-6; simple for audit/communication
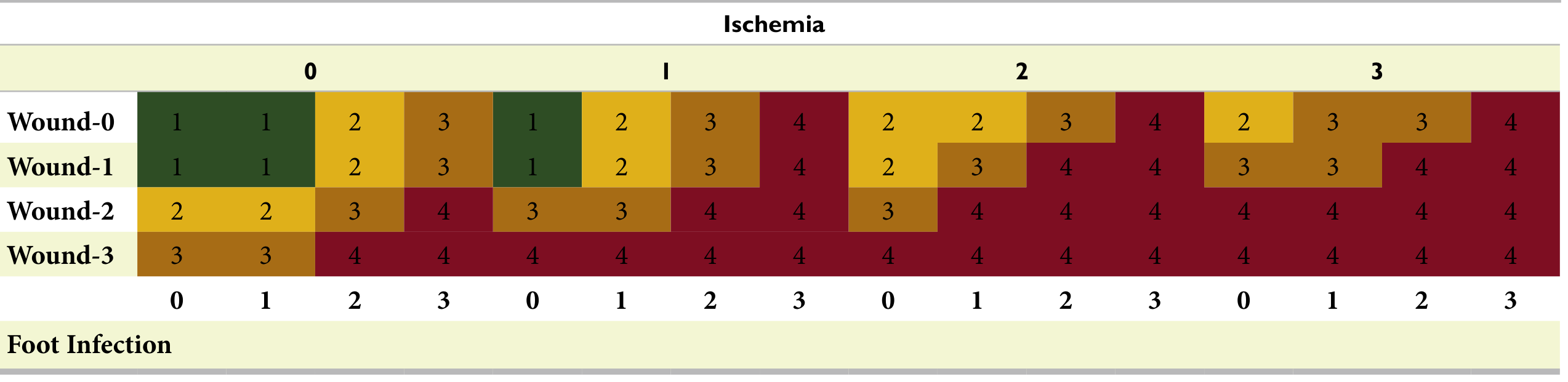
WiFi Classification (Society for Vascular Surgery - most comprehensive)
Three independent domains, each graded 0-3:
- W = Wound (depth/extent: 0=no wound, 1=superficial, 2=deep into tendon/joint, 3=to bone/full thickness)
- I = Ischemia (ankle-brachial index/toe pressures: 0=no ischemia, 1-2=moderate, 3=severe)
- f = foot Infection (0=none, 1=local <2 cm, 2=local >2 cm/abscess/osteomyelitis, 3=SIRS)
This creates 64 permutations predicting:
- Risk of major LEA at 1 year (Clinical Stage 1-4)
- Likelihood of benefit from revascularization
EXAMINATION OF THE DIABETIC FOOT
A structured examination covers three areas:
1. General and Vascular Assessment
- Pulses: Femoral, popliteal, posterior tibial, dorsalis pedis - absent/diminished suggests PAD
- Capillary refill time (normal <2 seconds)
- Ankle-Brachial Index (ABI): <0.9 = PAD; <0.4 = critical ischemia; >1.3 = calcified vessels (unreliable)
- Buerger's test: Pallor on elevation, dependent rubor on lowering = significant ischemia
- Toe pressures / TBI (toe-brachial index): more reliable in calcified vessels; <0.7 abnormal
- Skin temperature: Cool/cold = ischemia; warm = infection or Charcot
- Hair loss, skin atrophy, dystrophic nails = chronic ischemia signs
2. Neurological Assessment
- 10-g Semmes-Weinstein monofilament (key test): apply to 10 sites on plantar surface; inability to feel = loss of protective sensation (LOPS)
- Vibration: 128 Hz tuning fork at hallux; loss = early large-fiber neuropathy
- Temperature discrimination: warm/cool rods
- Pinprick sensation
- Proprioception (joint position sense)
- Ankle reflexes: absent in advanced neuropathy
- Motor exam: Intrinsic muscle wasting, toe deformities (claw toe, hammer toe), Charcot deformity
3. Wound Assessment
- Location: Neuropathic ulcers = plantar surface/pressure points; ischemic ulcers = toe tips/margins
- Callus debridement first - overriding callus hides wound extent
- Probe-to-bone test: Insert sterile probe into wound; if bone is felt = osteomyelitis until proven otherwise (PPV ~89%)
- Wound depth and undermining
- Signs of infection: Odor, purulent drainage, erythema >2 cm, warmth, swelling, fluctuance
- Maceration: Suggests infection or fluid overload
- Necrosis/gangrene: Dry (black, demarcated) vs. wet (spreading infection, odor, systemic upset)
- Sinus tracts - probe gently to determine depth
INVESTIGATIONS
Laboratory
| Test | Purpose |
|---|---|
| HbA1c | Glycemic control (target <7-7.5%) |
| FBC / WBC | Infection (WBC may be normal even with severe infection!) |
| CRP / ESR | Inflammatory markers (may be only mildly raised) |
| Blood cultures | Systemic sepsis / bacteremia |
| Wound swab / deep tissue culture | Microbiology (deep tissue > surface swab for reliability) |
| Renal function, electrolytes | Pre-op assessment, antibiotic dosing |
| Coagulation | Pre-op |
Important: Inflammatory markers are frequently unhelpful in diabetic foot infection as they may be normal or only mildly raised. (Bailey & Love)
Imaging
| Investigation | Indication / Finding |
|---|---|
| Plain X-ray (3 views) | First-line: cortical destruction/periosteal reaction = osteomyelitis (late sign); gas in soft tissues = gas-forming organisms; Charcot changes; structural deformities |
| MRI foot | Gold standard for osteomyelitis detection (most sensitive and specific); used when X-ray equivocal or non-healing wound at 4-6 weeks |
| 3-phase bone scan | If MRI contraindicated (metal hardware, cardiac devices) |
| Duplex Doppler USS | PAD assessment, pre-revascularization mapping |
| CT angiography | Vascular anatomy; plan revascularization |
| Conventional angiography | Gold standard for PAD; therapeutic intervention |
| TCPO2 (transcutaneous oxygen pressure) | Wound oxygenation; <30 mmHg = poor healing potential |
Microbiology
- Superficial swabs are unreliable for determining deep infection organisms
- Deep tissue biopsy or bone biopsy is the gold standard for osteomyelitis culture
- Common organisms: S. aureus, beta-haemolytic streptococci, aerobic Gram-negative bacilli
- Pseudomonas is over-represented; anaerobes present in necrotic/abscess tissue
MANAGEMENT OF THE DIABETIC FOOT
A multidisciplinary team approach (vascular surgery, endocrinology, orthopedics, infectious disease, podiatry, wound care nurses) has been shown to reduce amputation rates.
1. Glycemic Control
- Poor glycemic control impairs wound healing and immune function
- HbA1c every 3 months; target <7-7.5%; insulin often required during admission
- Involve endocrinology team proactively
2. Wound Care
- Debridement: Sharp debridement of devitalized tissue (clinic or operative)
- Dressing selection (by wound type):
- Healthy wound = collagen dressing
- Fibrinous tissue = enzymatic (e.g., collagenase/Santyl, MediHoney)
- Deep healthy wound = VAC (negative pressure wound therapy / NPWT)
- Locally infected = iodine-based (Iodosorb) or topical mupirocin
- Macerated wound = silver alginate or absorptive foam
- Edema management: Multilayer compression; address systemic cause
3. Offloading
- Neuropathic ulcers are caused/perpetuated by pressure
- Total contact cast (TCC): Gold standard for offloading; redistributes plantar pressure; requires weekly change and clean wound
- DH walking boot, wedge shoes, heel-off shoes = alternatives
- Patients with PAD: caution with compression
4. Infection Management
(Bailey & Love 28E)
- Mild/local infection: Oral antibiotics (e.g., co-amoxiclav, flucloxacillin) + wound care
- Moderate/severe infection: IV antibiotics; empirical cover for S. aureus, streptococci, Gram-negatives, Pseudomonas (e.g., piperacillin-tazobactam) and anaerobes (metronidazole)
- Surgical debridement: Mandatory for collections, necrosis, abscess, or extensive osteomyelitis
- Osteomyelitis treatment:
- Conservative: 6-12 weeks antibiotics if no extensive bone involvement
- Surgical: excision of infected bone (ray amputation / sequestrectomy) + antibiotics
- Refer urgently if: spreading cellulitis, systemic SIRS, critical ischemia, wet gangrene
5. Revascularization for Ischemia
- If ABI <0.6 or non-healing wound + confirmed PAD → revascularization assessment
- Options:
- Endovascular (angioplasty ± stenting): Preferred for limited disease, elderly, comorbid patients
- Open bypass surgery (femoro-popliteal/distal bypass): For extensive occlusive disease
- Hybrid procedures: Combination
- Target: restore inline pulsatile flow to the foot
- Revascularization significantly improves amputation-free survival
6. Amputation
- Performed when limb not salvageable, non-revascularizable ischemia, life-threatening infection
- Levels (distal to proximal):
- Toe amputation
- Ray amputation (toe + metatarsal)
- Transmetatarsal amputation (TMA)
- Syme's (ankle disarticulation)
- Below-knee amputation (BKA)
- Above-knee amputation (AKA)
- Goal: most distal level with adequate tissue perfusion for healing
7. Prevention
- Annual foot examination for all diabetic patients
- Education on daily foot inspection, foot hygiene, appropriate footwear
- Custom therapeutic footwear (redistributes pressure)
- Regular podiatry review
- Aggressive glycemic, BP, and lipid control
- Smoking cessation

7. QUICK SUMMARY TABLE: NEUROPATHIC vs. ISCHEMIC FOOT
| Feature | Neuropathic | Ischemic |
|---|---|---|
| Pulses | Present | Absent/reduced |
| Sensation | Reduced/absent | Relatively preserved |
| Skin | Warm, dry, cracked | Cool, hairless, shiny |
| Ulcer site | Plantar (pressure points) | Toe tips, margins |
| Ulcer appearance | Painless, punched-out, callus rim | Painful, sloughy, pale base |
| ABI | Normal (>0.9) | Low (<0.9) |
| Bone changes | Charcot arthropathy | Distal/digital gangrene |
| Reflexes | Absent | Normal |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapters 415, 416, 417
- Bailey and Love's Short Practice of Surgery 28E, Chapter 43
- Current Surgical Therapy 14E (Kavousi, Hicks, Abularrage - Diabetic Foot chapter)
treatment guidelines of dm and diabetic foot
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the material needed. Let me compile the full treatment guidelines answer.
Treatment Guidelines for Diabetes Mellitus & Diabetic Foot
Sources: Harrison's Principles of Internal Medicine 22E (2025), Katzung's Basic & Clinical Pharmacology 16E, Current Surgical Therapy 14E, Fuster & Hurst's The Heart 15E
PART 1: TREATMENT GUIDELINES FOR DIABETES MELLITUS
GLYCEMIC TARGETS (ADA 2024)
| Parameter | Target |
|---|---|
| HbA1c (general) | < 7.0% |
| HbA1c (young, motivated, no hypoglycemia) | < 6.5% |
| HbA1c (elderly, comorbidities, hypoglycemia risk) | < 8.0% |
| Fasting/pre-meal glucose | 4.4 - 7.2 mmol/L (80 - 130 mg/dL) |
| Post-meal (1-2 h) glucose | < 10.0 mmol/L (< 180 mg/dL) |
| Time in Range (CGM, TIR) | > 70% of time in 3.9 - 10.0 mmol/L |
| Blood pressure | < 130/80 mmHg |
| LDL-cholesterol (with ASCVD) | < 70 mg/dL (< 50 mg/dL in very high risk) |
A. LIFESTYLE + NON-PHARMACOLOGIC TREATMENT
Medical Nutrition Therapy (MNT)
- High-quality, nutrient-dense foods; limit processed carbohydrates
- Mediterranean-style diet (rich in monounsaturated/polyunsaturated fats) preferred
- Carbohydrate monitoring for postprandial control; use glycemic index
- Avoid fructose/sucrose beverages
- Sodium < 2300 mg/day
- No routine vitamin/antioxidant supplements (except Vit D/calcium for bone health)
- Weight loss target: 5-10% of body weight in T2DM significantly improves glycemic control
Physical Activity
- ≥ 150 minutes/week of moderate-intensity aerobic exercise (or 75 min vigorous)
- Resistance training 2-3 times/week
- Reduce prolonged sitting; break sedentary time every 30 minutes
Psychosocial Care
- Screen for depression, anxiety, "diabetes distress" at every visit
- Involve diabetes educator, dietitian, psychologist as needed
Monitoring
- CGM (Continuous Glucose Monitoring): Preferred; provides glucose trend, TIR, time below range, hypoglycemia alerts
- HbA1c: Every 3 months (unstable) or every 6 months (stable, at target)
- Self-monitoring blood glucose (SMBG): Fingerstick, if CGM not available
B. PHARMACOLOGIC TREATMENT - TYPE 1 DM
Insulin is mandatory in all T1DM patients.
Insulin Preparations (Harrison's 22E)
| Type | Drug | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting | Aspart, Lispro, Glulisine | < 15 min | 0.5-1.5 h | 3-5 h |
| Rapid-acting inhaled | Inhaled human insulin | < 15 min | 1-2 h | 3 h |
| Short-acting | Regular (soluble) | 30-60 min | 2-3 h | 4-8 h |
| Intermediate | NPH | 2-4 h | 4-10 h | 10-16 h |
| Long-acting | Glargine (U100/U300) | 2-4 h | Peakless | 20-24 h |
| Ultralong-acting | Degludec | 1-9 h | Peakless | >42 h |
Insulin Regimen Strategies for T1DM
1. Basal-Bolus (MDI - Multiple Daily Injections):
- Basal insulin (glargine or degludec) once daily = suppresses fasting hepatic glucose
- Bolus insulin (rapid-acting) with each meal = carbohydrate coverage + correction
- Insulin-to-carbohydrate ratio + correction factor individualised
2. Continuous Subcutaneous Insulin Infusion (CSII / Insulin Pump):
- Delivers variable basal rate + manual bolus at meals
- More physiologic than MDI
3. Sensor-Augmented Pump:
- CSII + CGM; algorithm suspends insulin when glucose falls or predicted to fall
4. Automated Insulin Delivery (AID / Closed Loop / Artificial Pancreas):
- CGM + pump + algorithm adjusts basal rate in real time
- Closest to physiologic insulin replacement currently available
C. PHARMACOLOGIC TREATMENT - TYPE 2 DM
The current approach is individualized, comorbidity-driven, and cardiorenal outcome-focused rather than purely glucose-centric.
Step-by-Step Algorithm (ADA/EASD 2024)
Step 1: Assess for cardiovascular/renal comorbidities first
Does the patient have:
- Established ASCVD or high CV risk? → Prioritize GLP-1 RA or SGLT-2 inhibitor
- Heart failure? → Prioritize SGLT-2 inhibitor
- CKD (eGFR ≥20)? → Prioritize SGLT-2 inhibitor
- Obesity / weight loss needed? → Prioritize GLP-1 RA or GLP-1/GIP dual agonist
- Hypoglycemia risk? → Avoid sulfonylureas/insulin if possible
Step 2: Start Metformin (if no contraindications)
- First-line in all T2DM without contraindications
- Contraindicated: eGFR < 30 mL/min, active liver disease, significant alcohol use, risk of lactic acidosis, IV contrast procedures
Step 3: Add agents based on cardiorenal needs (see below)
Drug Classes for T2DM - Detailed
(Katzung's Basic & Clinical Pharmacology 16E, Harrison's 22E)
1. BIGUANIDES - Metformin
- Mechanism: Activates AMP kinase → reduces hepatic gluconeogenesis, improves insulin sensitivity in muscle/liver
- HbA1c reduction: 1.0 - 2.0%
- Benefits: Weight neutral/modest loss, no hypoglycemia, CV-neutral, inexpensive
- Side effects: GI (nausea, diarrhea, metallic taste - take with food); B12 deficiency with long-term use; lactic acidosis (rare)
- Dose: Start 500 mg daily with food; titrate to 1000 mg BD (max 2550 mg/day)
2. SGLT-2 INHIBITORS (Gliflozins)
- Mechanism: Block SGLT-2 in proximal renal tubule → block glucose reabsorption → glucosuria → glucose lowering (insulin-independent)
- Drugs: Empagliflozin, Dapagliflozin, Canagliflozin
- HbA1c reduction: 0.5 - 1.0%
- Additional benefits:
- Weight loss (3-5 kg)
- BP reduction (3-6 mmHg systolic)
- Reduces ASCVD events and CV mortality (empagliflozin, canagliflozin)
- Reduces heart failure hospitalizations
- Slows CKD progression (empagliflozin, canagliflozin, dapagliflozin)
- Side effects: Genital mycotic infections (both sexes), UTIs, polyuria, DKA risk (euglycemic DKA - especially if insulin omitted during illness), increased fracture risk (canagliflozin), lower limb amputation risk (canagliflozin)
- Contraindication: eGFR < 20 mL/min (not effective); T1DM
- Do not initiate if: eGFR < 30 (CKD Stage 3b), but can continue if eGFR falls during treatment
3. GLP-1 RECEPTOR AGONISTS (GLP-1 RAs)
- Mechanism: Mimic GLP-1 incretin hormone → glucose-dependent insulin secretion, suppress glucagon, slow gastric emptying, central appetite suppression
- Drugs:
- Injectable: Semaglutide (weekly, Ozempic), Liraglutide (daily, Victoza), Dulaglutide (weekly), Exenatide
- Oral: Semaglutide (Rybelsus, daily)
- HbA1c reduction: 1.0 - 1.8%
- Additional benefits:
- Significant weight loss (5-15 kg)
- Reduces ASCVD events (liraglutide, semaglutide) - mortality benefit in T2DM with CVD
- Reduces CKD progression (semaglutide - FLOW trial 2024)
- Reduces BP
- Side effects: Nausea, vomiting, diarrhea (dose-dependent, transient); pancreatitis risk; Black box warning: thyroid C-cell tumors (contraindicated in personal/family history of medullary thyroid cancer or MEN2); slows gastric emptying (affects oral drug absorption)
- No hypoglycemia when used as monotherapy
4. GLP-1/GIP DUAL AGONIST (Twincretin)
- Drug: Tirzepatide (Mounjaro) - weekly SC injection
- Mechanism: Dual agonism at GIP + GLP-1 receptors → greater weight loss than GLP-1 RA alone
- HbA1c reduction: 1.9 - 2.6% (dose-dependent)
- Weight loss: 6 - 13 kg on average (superior to all other agents)
- Doses: 2.5 mg/week → titrate every 4 weeks to max 15 mg/week
- Beneficial effects on lipids, BP, fatty liver
- Side effects same as GLP-1 RAs; slightly higher pancreatitis rate
5. DPP-4 INHIBITORS (Gliptins)
- Mechanism: Inhibit DPP-4 enzyme → prolong action of native GLP-1 and GIP → enhanced glucose-dependent insulin secretion
- Drugs: Sitagliptin (100 mg OD), Vildagliptin, Saxagliptin, Linagliptin, Alogliptin
- HbA1c reduction: 0.5 - 1.0%
- Benefits: Weight neutral; no hypoglycemia; oral dosing; generally well tolerated
- Side effects: Nasopharyngitis; rare - pancreatitis, severe joint pain, angioedema; Saxagliptin increases heart failure risk (avoid in HF patients)
- Renal dose adjustment: Sitagliptin (50 mg if eGFR 30-50; 25 mg if < 30); Linagliptin - no adjustment needed (biliary excretion)
6. SULFONYLUREAS
- Mechanism: Bind sulfonylurea receptor → close ATP-K+ channel → depolarize beta cell → calcium influx → insulin release (glucose-independent)
- Drugs: Glipizide, Glibenclamide (glyburide), Gliclazide, Glimepiride
- HbA1c reduction: 1.0 - 2.0%
- Side effects: Hypoglycemia (most significant - especially glyburide); weight gain (2-4 kg)
- Avoid in: Elderly (hypoglycemia risk), renal failure, irregular meals
- Note: Older agents but inexpensive; avoid if hypoglycemia is a concern
7. THIAZOLIDINEDIONES (TZDs)
- Mechanism: PPARγ agonists → improve insulin sensitivity in adipose/muscle/liver
- Drug: Pioglitazone (Actos)
- HbA1c reduction: 0.5 - 1.4%
- Benefits: No hypoglycemia; reduces TG, raises HDL; may reduce NASH
- Side effects: Fluid retention / edema; weight gain (2-4 kg); heart failure exacerbation (contraindicated in NYHA class III/IV HF); bone fractures; possible bladder cancer (controversial for pioglitazone)
8. MEGLITINIDES / GLINIDES
- Mechanism: Rapid-acting insulin secretagogues (same receptor as SU but shorter acting)
- Drugs: Repaglinide, Nateglinide
- Use: Post-meal glucose spikes; useful in irregular meal patterns; dose with each meal
- Side effects: Hypoglycemia (less than SUs); weight gain
9. ALPHA-GLUCOSIDASE INHIBITORS
- Mechanism: Inhibit brush border enzymes → delay intestinal carbohydrate absorption → reduce post-meal glucose
- Drug: Acarbose, Miglitol
- HbA1c reduction: 0.5 - 0.8%
- Side effects: Flatulence, diarrhea, abdominal pain (limits use)
10. INSULIN IN T2DM
- Added when oral agents + injectables fail to maintain target HbA1c
- Starting regimen: Basal insulin at night (glargine or degludec, 10 units or 0.1-0.2 units/kg) + continue oral agents (except sulfonylureas may need dose reduction)
- Escalation: Add prandial insulin for persistent post-meal hyperglycemia
- Combination: Basal insulin + GLP-1 RA (very effective; reduces insulin dose required and weight gain)
Summary: Drug Choice by Comorbidity (ADA 2024 / ESC/EASD Guidelines)
| Clinical Scenario | Preferred Agent(s) |
|---|---|
| Established ASCVD or high CV risk | GLP-1 RA (liraglutide, semaglutide) or SGLT-2 inhibitor |
| Heart failure (HFrEF or HFpEF) | SGLT-2 inhibitor (empagliflozin, dapagliflozin) |
| CKD (eGFR ≥ 20) | SGLT-2 inhibitor first; add finerenone; semaglutide |
| Obesity / weight management | GLP-1 RA or tirzepatide |
| Hypoglycemia risk | Avoid SUs; prefer DPP-4i, SGLT-2i, GLP-1 RA |
| Cost constraints | Metformin + sulfonylurea + NPH insulin |
| Elderly / frail | DPP-4i (sitagliptin); avoid SUs and TZDs |
D. TREATMENT OF ACUTE COMPLICATIONS
DKA Treatment Protocol (Harrison's 22E)
1. Fluids (most urgent)
- 1-2 L 0.9% NaCl over first hour
- Then 250-500 mL/hr 0.9% NaCl (or 0.45% if Na > 135 meq/L)
- Switch to D5 0.45% saline when glucose drops to 11.1-13.9 mmol/L (200-250 mg/dL)
2. Insulin
- IV regular insulin bolus 0.1 units/kg IV, then 0.1 units/kg/hr infusion
- If glucose not falling by 10% in first hour: double infusion rate
- Reduce insulin to 0.02-0.1 units/kg/hr when glucose reaches 200-250 mg/dL
- Do NOT stop insulin until anion gap closes and patient eating
3. Potassium Replacement
- If K+ < 3.5 mEq/L: hold insulin, give 20-40 mEq/hr KCl first
- If K+ 3.5-5.0 mEq/L: add 20-30 mEq K+ to each liter of IV fluid
- If K+ > 5.0 mEq/L: hold K+, monitor hourly
4. Bicarbonate: Only if pH < 6.9 (controversial; avoid routinely)
5. Phosphate: Replace if < 1.0 mg/dL or symptomatic
6. Identify and treat precipitant (infection, MI, missed insulin)
HHS Treatment
- Fluid deficit often 9-10 L (more profound than DKA); replace over 1-2 days
- 1-3 L 0.9% NaCl first 2-3 hours, then 0.45% saline
- Insulin: 0.1 units/kg IV bolus → 0.1 units/kg/hr infusion
- Potassium replacement as in DKA
- Mortality up to 15% - aggressive monitoring required
E. CARDIOVASCULAR RISK REDUCTION IN DM
| Target | Goal / Agent |
|---|---|
| BP | < 130/80 mmHg; ACEI or ARB first-line (especially with proteinuria) |
| LDL | < 70 mg/dL all T2DM > 40 years; statin mandatory |
| Antiplatelet | Aspirin for secondary prevention; consider in primary prevention if high CV risk |
| Smoking | Cessation - highest modifiable risk factor |
| SGLT-2i/GLP-1 RA | Add regardless of HbA1c if ASCVD present |
PART 2: TREATMENT GUIDELINES FOR THE DIABETIC FOOT
OVERALL PRINCIPLE: MULTIDISCIPLINARY TEAM
Effective management requires: Vascular Surgery + Endocrinology + Infectious Disease + Orthopaedics/Podiatry + Wound Care Nurses + Dietitian + Physiotherapy
STEP 1 - GLYCEMIC OPTIMIZATION
- HbA1c checked every 3 months; target < 7-7.5%
- Tight inpatient glycemic control (IV insulin infusion if needed) as hyperglycemia impairs:
- Neutrophil chemotaxis and phagocytosis
- Wound healing
- Tissue oxygenation
- Involve endocrinology for all inpatient DFU admissions
STEP 2 - WOUND CARE
A. Sharp Debridement
- Remove all devitalized, necrotic, and callus tissue
- Conservative mindset: preserve viable tissue, excise dead tissue
- Hydroresection / jet lavage for deep spaces
- Aggressive debridement before revascularization should be avoided
B. Dressing Selection (by wound type)
| Wound Character | Dressing |
|---|---|
| Healthy granulating wound | Collagen dressing |
| Fibrinous/sloughy | Enzymatic (Santyl/collagenase, MediHoney) |
| Deep healthy wound | VAC / NPWT (Negative Pressure Wound Therapy) |
| Locally infected | Iodine-based (Iodosorb), topical mupirocin (Bactroban) |
| Macerated wound | Silver alginate, absorptive foam |
| Wound + periwound maceration | Separate base dressing + zinc-oxide barrier to edges |
| Exposed bone/osteomyelitis | Surgical excision indicated |
C. Edema Management
- Multilayer compression bandaging (if no critical ischemia)
- Treat underlying cause (venous HTN, lymphedema, cardiac failure)
STEP 3 - PRESSURE OFFLOADING
Essential for neuropathic ulcers at plantar pressure points:
| Device | Notes |
|---|---|
| Total Contact Cast (TCC) | Gold standard; requires clean wound, reliable patient, weekly changes |
| DH Walker Boot / Walking Boot | More practical alternative; removable (patient compliance issue) |
| Wedge / Heel-Off Shoes | For forefoot / heel ulcers specifically |
| Crutches / Wheelchair | Non-weight-bearing when needed |
| Custom orthotic insoles | Prevention of recurrence after healing |
STEP 4 - INFECTION MANAGEMENT
(Bailey & Love 28E, Current Surgical Therapy 14E)
Antibiotic Selection by Severity
| Severity (IDSA/WIfI Grade) | Organisms to Cover | Antibiotic |
|---|---|---|
| Grade 1 - Mild (local, < 2 cm) | S. aureus, streptococci | Oral co-amoxiclav 625 mg TDS, or flucloxacillin 500 mg QDS |
| Grade 2 - Moderate (> 2 cm, deep) | Gram-positive + Gram-negative | IV co-amoxiclav, or ciprofloxacin + clindamycin; add metronidazole if necrosis/abscess |
| Grade 3 - Severe (SIRS) | Broad-spectrum + Pseudomonas + anaerobes | IV piperacillin-tazobactam (Tazocin), or meropenem ± metronidazole; add vancomycin/teicoplanin if MRSA suspected |
| Osteomyelitis | Prolonged | 6-12 weeks antibiotics; guided by bone biopsy cultures |
Culture Rules:
- Surface swabs are unreliable - do NOT rely on them
- Obtain deep tissue biopsy or bone biopsy for microbiology
- Blood cultures for systemic sepsis
Surgical Debridement Indications
- Collections / abscess
- Wet gangrene / necrotizing fasciitis (surgical emergency)
- Necrotic tissue not responding to conservative management
- Extensive osteomyelitis
- Devitalized tissue that prevents wound healing
STEP 5 - MANAGEMENT OF ISCHEMIA (PAD)
(Current Surgical Therapy 14E)
Vascular Assessment Thresholds
- ABI < 0.6 or ankle pressure < 60 mmHg = significant ischemia; consider revascularization
- Toe pressure < 30 mmHg = inadequate for wound healing (< 40 mmHg in diabetics)
- TcPO2 < 20 mmHg = healing failure very likely; > 60 mmHg = adequate healing
TASC Classification of Arterial Lesions (for revascularization planning)
| TASC Grade | Description | Preferred Approach |
|---|---|---|
| A | Short focal stenosis | Endovascular (balloon angioplasty) |
| B | Multiple short stenoses, short occlusion | Endovascular preferred |
| C | Long stenosis/occlusion, multiple lesions | Surgical bypass preferred; endovascular in poor candidates |
| D | Long occlusions, extensive disease | Open bypass |
Endovascular Options
- Balloon angioplasty ± stenting: Iliac arteries - durable; femoro-popliteal - less durable
- Drug-eluting stents / drug-coated balloons: Improved 1-year patency for femoropopliteal
- Subintimal dissection + reentry: For long occlusions
- Atherectomy: Plaque excision to restore lumen
Open Bypass Surgery
- Femoro-popliteal bypass (above or below knee)
- Femoro-distal bypass (tibial or pedal vessels) for isolated distal disease
- Conduit: Autologous saphenous vein preferred > synthetic (PTFE/Dacron)
- Assess cardiac risk before open bypass (diabetes + PAD = high CAD prevalence)
ICG Fluorescence Angiography (SPY System)
- Newer technique using indocyanine green + laser camera
- Objectively assesses tissue perfusion to guide amputation level and flap viability
STEP 6 - OSTEOMYELITIS MANAGEMENT
| Approach | Indication |
|---|---|
| Medical (antibiotics alone) | Limited osteomyelitis without extensive cortical destruction; surgery high risk; non-operative candidate |
| Surgical excision (Ray/sequestrectomy) | Probe-to-bone positive, cortical destruction, abscess formation, non-healing after 6 weeks maximal care |
| Duration of antibiotics | 6 weeks if bone excised with clear margins; 12 weeks if residual infected bone |
STEP 7 - AMPUTATION (When Limb Not Salvageable)
Indications:
- Non-revascularizable critical ischemia
- Life-threatening wet gangrene / necrotizing fasciitis
- Extensive osteomyelitis not amenable to conservative surgery
- Intractable pain with no reconstructive option
- Patient preference or unacceptably poor functional prognosis
Levels (distal to proximal - always aim for most distal viable level):
| Level | Description |
|---|---|
| Digital amputation | Single toe |
| Ray amputation | Toe + metatarsal (up to 2 rays can be resected) |
| Transmetatarsal (TMA) | Across all metatarsals; good functional outcome |
| Syme's amputation | Ankle disarticulation; end-bearing stump |
| Below-knee (BKA) | Transtibial; allows prosthetic walking; needs knee |
| Above-knee (AKA) | Transfemoral; for failed BKA or knee joint involvement |
Perioperative care:
- Nutritional optimization before surgery
- Prevent bedsores, UTIs, falls
- Physiotherapy for rehabilitation
- Enhanced recovery protocols
STEP 8 - PREVENTION AND FOOT CARE
| Measure | Frequency |
|---|---|
| Foot inspection by patient | Daily |
| Foot examination by clinician | Every visit (T1DM) / Annually minimum (T2DM) |
| Monofilament + vibration testing | Annually |
| HbA1c | Every 3 months (DFU patient) |
| Podiatry review | 1-3 monthly (high risk) |
| Nail / callus care | By podiatrist; patient must never self-treat |
| Footwear | Custom therapeutic shoes; broad toe box; no barefoot walking |
| Patient education | Inspect feet daily; avoid heat; never walk barefoot; report sores immediately |
| Smoking cessation | Absolute priority |
| Lipid/BP control | Statin + antihypertensive |
DIABETIC FOOT - DECISION ALGORITHM SUMMARY
DFU Identified
│
├─ Assess Wound (Probe, Debride, X-ray)
├─ Assess Ischemia (ABI, toe pressure, duplex)
└─ Assess Infection (cultures, WBC, CRP, MRI if needed)
│
▼
WIfI Classification (Grade Wound / Ischemia / Infection 0-3)
│
┌──────┴──────┐
No ischemia Ischemia present
(ABI ≥ 0.9) (ABI < 0.6 or toe pressure < 30-40 mmHg)
│ │
Offload Vascular referral
Wound care Duplex / CTA / MRA
Antibiotics Revascularisation (endovascular or bypass)
│ │
└─────────┬──────────┘
│
Infection present?
┌────┴────┐
Yes No
│ │
IV antibiotics Local wound care
Surgical debridement Offloading
Bone Bx if osteomyelitis Regular review
│
Not healing / gangrene?
│
Amputation planning
(most distal viable level)
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapters 416, 417
- Katzung's Basic & Clinical Pharmacology 16E, Chapter 41
- Current Surgical Therapy 14E - Diabetic Foot chapter (Kavousi, Hicks, Abularrage)
- Bailey & Love's Short Practice of Surgery 28E, Chapter 43
- Fuster & Hurst's The Heart 15E, Chapter 7 (ESC/EASD/ACC/AHA Guidelines for DM and CVD)
This is a shared conversation. Sign in to Orris to start your own chat.