Cataract surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cataract surgery" AND outcomes
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of cataract surgery based on Kanski's Clinical Ophthalmology (10th ed.) and Miller's Anesthesia (10th ed.).
Cataract Surgery
Overview
Cataract surgery involves removal of the opacified crystalline lens and replacement with an artificial intraocular lens (IOL). It is the most commonly performed elective surgical procedure worldwide, with excellent visual outcomes in the vast majority of patients.
Surgical Techniques
1. Intracapsular Cataract Extraction (ICCE) - Historical
A cryoprobe removes the entire lens together with its capsule. Now largely abandoned in favour of ECCE and phacoemulsification.
2. Extracapsular Cataract Extraction (ECCE)
A large anterior capsulotomy is made, a limbal incision (8-10 mm) is completed, and the nucleus is expressed after hydrodissection. Cortical matter is aspirated, leaving the capsular bag intact for IOL support. Suturing is required, which can induce corneal astigmatism.
3. Manual Small-Incision Cataract Surgery (MSICS)
A variant of ECCE designed for high-volume treatment of dense cataracts in resource-limited settings. A self-sealing sclero-corneal tunnel is created, the capsule is stained for capsulorhexis, the nucleus is manually expressed, cortex is aspirated, and an IOL is implanted. Visual rehabilitation is comparable to phacoemulsification but is faster and avoids expensive technology.
- Kanski's Clinical Ophthalmology, p. 308
4. Phacoemulsification (Standard Modern Technique)
Phaco is the standard method in high-income countries and regional centres in most lower-income countries.
Phacodynamics
- Bottle height: Controls infusion flow and intraocular pressure (IOP) stability; flow is proportional to bottle height
- Aspiration flow rate (AFR): Volume of fluid removed (ml/min); high AFR attracts lens material to the phaco tip faster but reduces effective power - trainee surgeons should use lower AFR
- Vacuum (mmHg): Generated when the pump attempts to aspirate during occlusion; determines how tightly material is held by the tip; lower vacuum slows events, reduces surge risk
- Post-occlusion surge: When tip occlusion breaks, pent-up energy causes a sudden outflow increase - can cause capsular rupture; suppressed by modern phaco machines
Pump Types
- Peristaltic (flow) pump: Pulls fluid by compressing tubing; vacuum builds only after tip occlusion, then stops at preset level
- Venturi (vacuum) pump: Driven by compressed gas, generating vacuum directly and immediately; faster vacuum response
Surgical Steps
- Preparation: Topical anaesthetic, 5% povidone-iodine instilled into conjunctival sac (left for minimum 3 minutes), eyelid cleaning, draping to exclude lashes
- Incisions: Side port ~60° from main incision (right-handed surgeon); viscoelastic injected into AC; main corneal incision sited on steepest corneal axis
- Capsulorhexis: Continuous curvilinear capsulorhexis with cystotome or capsule forceps
- Hydrodissection: Blunt cannula inserted under capsulorhexis edge; fluid injected to separate nucleus/cortex from capsule; a hydrodissection wave confirms success
- Nucleus removal - three main techniques:
- Divide and conquer: Two perpendicular grooves sculpted, nucleus cracked into quadrants, each emulsified and aspirated - safe, widely used
- Phaco chop (horizontal): Blunt-tipped chopper passed under capsule to equator, nucleus split into pieces - faster, lower total phaco energy, longer learning curve
- Phaco chop (vertical): Pointed-tip chopper, does not pass beyond capsulorhexis
- Stop and chop: Combination technique
- Cortex removal: Cortical segments aspirated using vacuum; automated coaxial, bimanual automated, or manual (Simcoe cannula) methods
- IOL insertion: Capsular bag filled with cohesive viscoelastic; loaded injector cartridge introduced through main wound; IOL deployed into capsular bag
5. Femtosecond Laser-Assisted Cataract Surgery (FLACS)
A laser platform performs some steps (capsulorhexis, nuclear fragmentation, corneal incisions) with precision. Useful especially for toric IOL alignment and in complex cases.
Preoperative Evaluation
Patients are often elderly with multiple comorbidities, but cataract surgery is short and low-risk - very little precludes it if the patient can lie flat for the duration.
Conditions requiring optimization before proceeding (SAMBA guidelines):
- Myocardial infarction within 30 days (uncomplicated) or 60 days (complicated)
- PCI within 14 days (no stent) or 30 days (with stent)
- Significant arrhythmias with haemodynamic compromise (VT, AF with rapid rates)
- Decompensated heart failure
- Active pneumonia, PE in past 3 months
- Stroke/TIA within 3 months, uncontrolled epilepsy, raised ICP
- Malignant hypertension
- DKA or HHS
Key perioperative points:
- Elevated BP or hyperglycaemia on the day of surgery does NOT generally warrant delay
- Antiplatelet and anticoagulant medications should NOT be stopped - bleeding risk is very low (<0.4%)
- Routine preoperative medical testing (including cardiac risk assessment) is NOT recommended
- New-onset asymptomatic AF on day of surgery - surgery can proceed; refer for early outpatient management
- Miller's Anesthesia, p. 9724-9725
Biometry and IOL Power Calculation
Biometry calculates the IOL power needed for the desired refractive outcome.
- Keratometry: Measures anterior corneal curvature (steepest and flattest meridians, in dioptres or mm)
- Optical coherence biometry (preferred): Non-contact axial length measurement using partial coherence interferometry (e.g. IOLMaster); also measures keratometry, anterior chamber depth, lens thickness, white-to-white diameter
- Ultrasound biometry (A-scan): Used when OCB is not possible (e.g. dense cataract blocking the signal)
- IOL formulas: Haigis, SRK/T, Barrett Universal II, Kane formula - selection depends on axial length
IOL Types
| Type | Feature |
|---|---|
| Monofocal | Corrects for one distance (usually distance); requires reading glasses |
| Toric | Corrects pre-existing corneal astigmatism |
| Multifocal (bifocal/trifocal) | Two or three focal points; reduces spectacle dependence; may cause halos/glare |
| Extended Depth of Focus (EDOF) | Single elongated focal zone; fewer dysphotopsias than trifocal; less near vision |
| Accommodating | Attempt to mimic natural accommodation (variable results) |
A recent Cochrane meta-analysis (Tavassoli et al., 2024, PMID 38984608) compared trifocal vs EDOF IOLs, finding trifocals generally provide better uncorrected near vision, while EDOF lenses may have fewer dysphotopsias.
Anesthesia
- Topical anaesthesia: Most common; drops only; no block; suitable for cooperative patients
- Peribulbar block: Local anaesthetic injected outside the muscle cone; good akinesia and analgesia
- Retrobulbar block: Injected inside the muscle cone; more complete akinesia but higher risk (globe perforation, retrobulbar haemorrhage, brainstem anaesthesia)
- Sub-Tenon block: Low-pressure cannula technique; relatively safe
- MAC (Monitored Anaesthesia Care): Sedation with local/topical; avoids GA risks
- General anaesthesia: Reserved for uncooperative or paediatric patients; avoid succinylcholine (raises IOP transiently)
Informed Consent: Risk Discussion
- ~1 in 1,000 operations: eye left with little or no sight
- ~1 in 10,000: loss of the eye
Common (mild, usually treatable):
- Periocular ecchymosis
- Allergy to eye drops
- IOP spike
- Iridocyclitis
- Posterior capsular opacification (PCO)
Less common (moderate-severe):
- Posterior capsular rupture with vitreous loss: <1% experienced surgeons, higher for trainees
- Zonular dehiscence
- Dropped nucleus (~0.2%)
- Cystoid macular oedema (CMO/Irvine-Gass syndrome)
- Corneal decompensation
- Unexpected refractive outcome
- Retinal detachment (<1%)
- IOL dislocation
- Persistent ptosis or diplopia
Rare but serious:
- Endophthalmitis (0.1%)
- Suprachoroidal haemorrhage (0.04%)
Kanski's Clinical Ophthalmology, p. 315
Complications in Detail
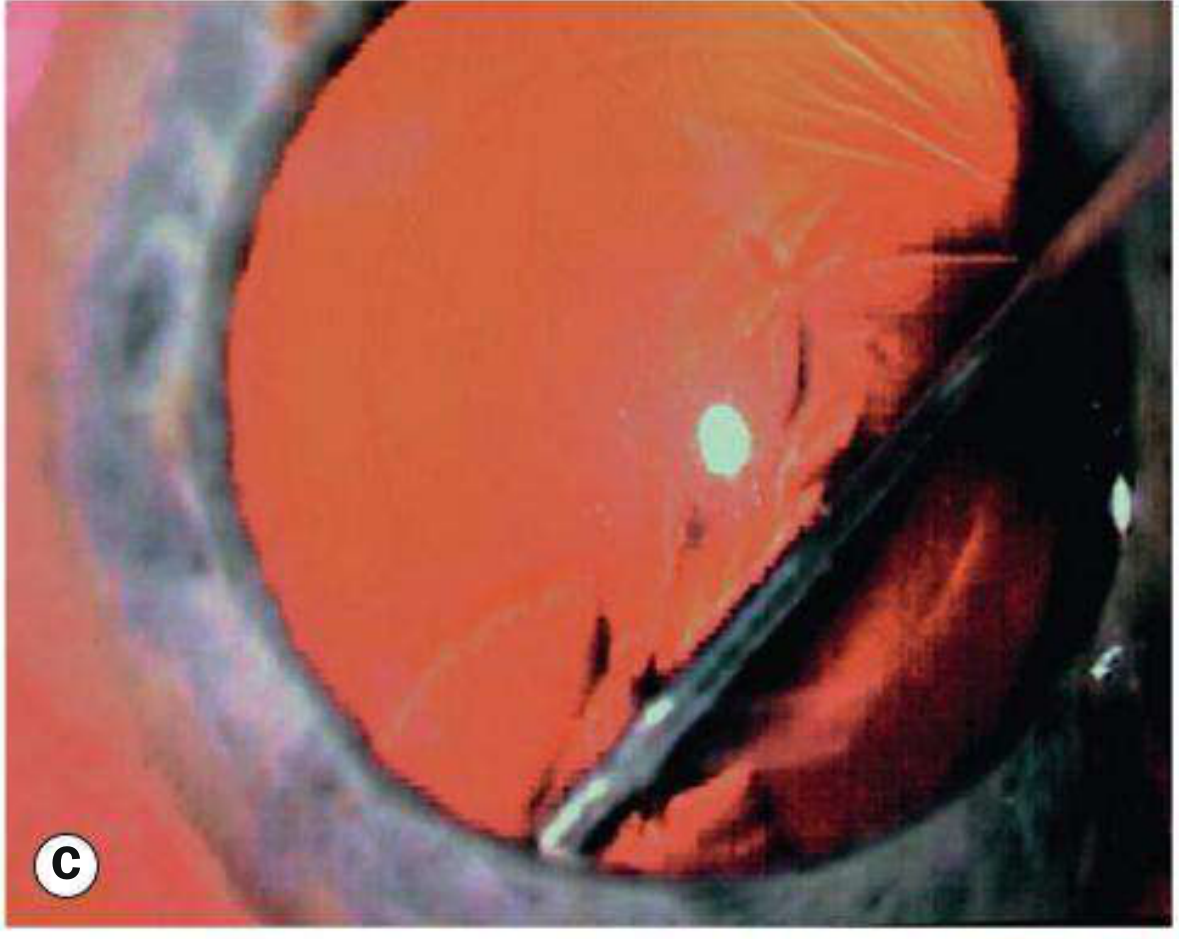
Posterior Capsular Rupture (Intraoperative)
If a small posterior capsular tear occurs, dispersive viscoelastic is used to push vitreous back and plug the defect. Residual nuclear fragments can be removed by phaco at low bottle height and low AFR, or by visco-expression after wound extension. Re-plugging the tear with dispersive OVD and using manual aspiration with irrigation off helps safely remove residual cortex.
Acute Postoperative Endophthalmitis
- Incidence: ~0.1%
- Pathogens: ~90% Gram-positive (most commonly S. epidermidis), ~10% Gram-negative
- Risk factors: posterior capsule rupture, prolonged surgery, clear corneal sutureless incision, temporal incision, wound leak, delayed postoperative antibiotics, diabetes, adnexal disease
- Prophylaxis: Intracameral cefuroxime 1 mg in 0.1 ml at end of surgery (or moxifloxacin 0.5 mg/0.1 ml if unavailable); avoid intracameral vancomycin (risk of haemorrhagic occlusive retinal vasculitis)
- Treatment: Intravitreal ceftazidime 2 mg/0.1 ml + vancomycin 2 mg/0.1 ml immediately after obtaining culture specimens; oral moxifloxacin 400 mg/day x10 days; oral prednisolone 1 mg/kg/day (after 12-24 hours, once fungal infection excluded)
Posterior Capsular Opacification (PCO)
- Most common late complication
- Caused by migration and proliferation of residual lens epithelial cells
- Presents as gradual visual decline weeks to months postoperatively
- Types: vacuolated/pearl type (Elschnig pearls), fibrotic
- Treatment: Nd:YAG laser posterior capsulotomy - creates a clear central opening in the opacified capsule; outpatient, quick, effective
Cystoid Macular Oedema (Irvine-Gass Syndrome)
- Peak incidence 6-10 weeks post-surgery
- Incidence increases with surgical complications
- Treated with topical NSAIDs ± steroids
Immediate Sequential vs. Delayed Sequential Bilateral Cataract Surgery (ISBCS vs. DSBCS)
Large trials show no difference in visual acuity or complications at 1 month and 1 year. ISBCS remains debated due to the theoretical risk of bilateral endophthalmitis; meticulous patient selection is essential.
Postoperative Care
- Pain is usually short-lived; persistent pain may indicate choroidal effusion, suprachoroidal haemorrhage, or aqueous misdirection syndrome
- Topical antibiotics and steroids in the first weeks
- IOP monitored on day 1 (risk of acute IOP spike from retained viscoelastic)
- Watch for signs of endophthalmitis: pain, redness, reduced vision, hypopyon within 2-7 days postoperatively
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach (10th ed.) | Miller's Anesthesia (10th ed.) | Tavassoli et al. Cochrane 2024 - Trifocal vs EDOF IOLs
How toTest near and far vision
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-based guide on how to test near and far (distance) vision.
Testing Near and Far Vision
Part 1: Distance (Far) Visual Acuity
What it measures
Distance visual acuity (VA) is the minimum angle of separation between two objects (subtended at the eye's nodal point) that allows them to be perceived as distinct. It reflects the resolving power of the central fovea.
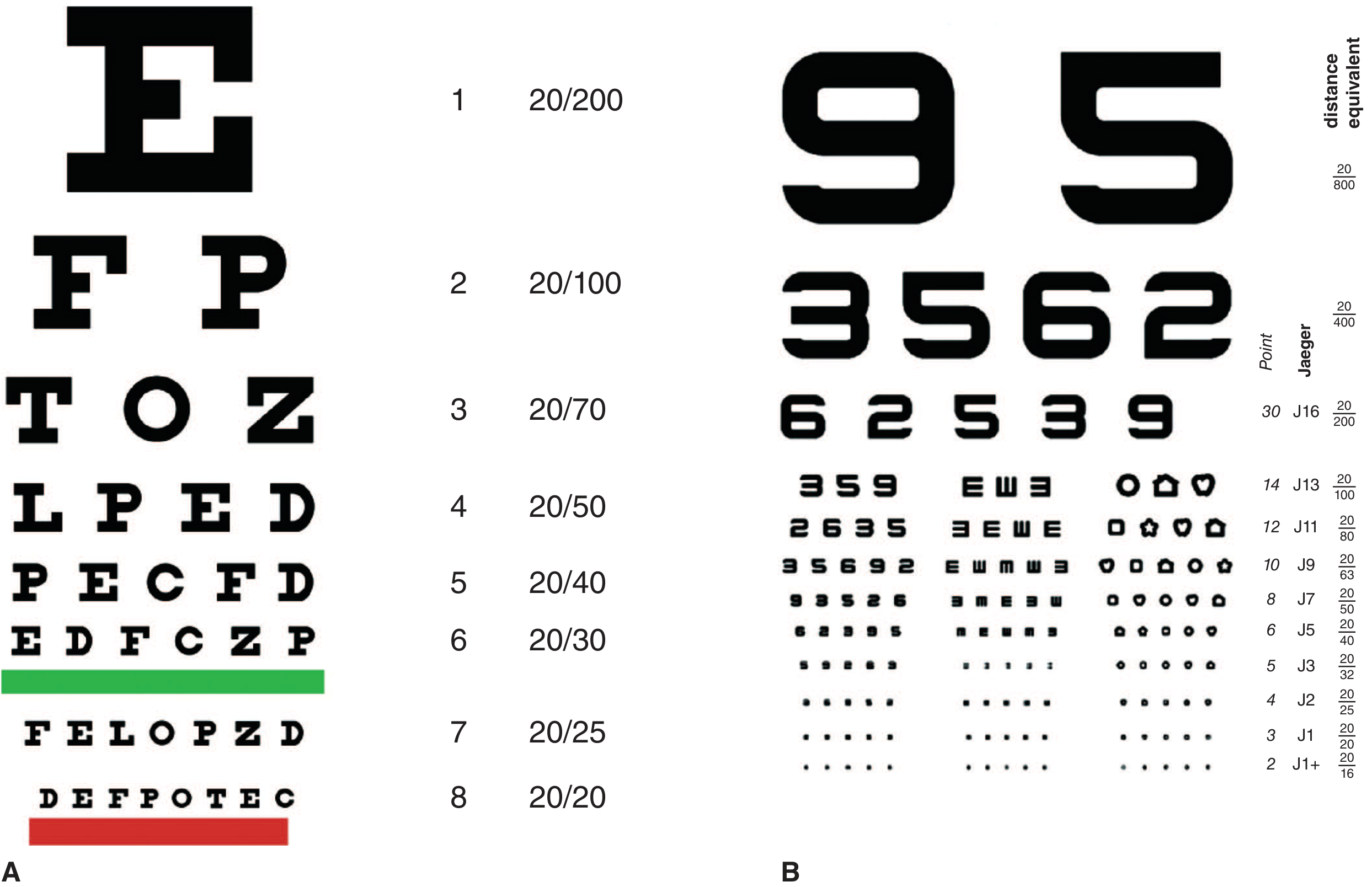
The Snellen Chart
The Snellen chart is the most widely used tool for distance VA testing.
How to perform:
- Place the patient 6 metres (20 feet) from the chart (or use a mirror system to simulate this in a smaller room)
- The room should be well lit
- Test the worse eye first, with the other eye firmly occluded
- The patient should wear their usual distance glasses or contact lenses if they have them
- Push the patient to read every letter possible, even if uncertain
- Record the smallest line the patient can read correctly
Recording:
- Written as a fraction: distance tested / distance at which a person with normal vision reads that line
- Example: 6/6 (20/20) = normal. Patient reads at 6 m what a normal person reads at 6 m
- 6/12 (20/40) = patient reads at 6 m what a normal person reads at 12 m (reduced vision)
- 6/60 (20/200) = only the top letter visible - significantly reduced
Also record:
- Unaided (uncorrected) VA - without glasses
- Best-corrected VA (BCVA) - with optimal spectacle correction
Pinhole Test
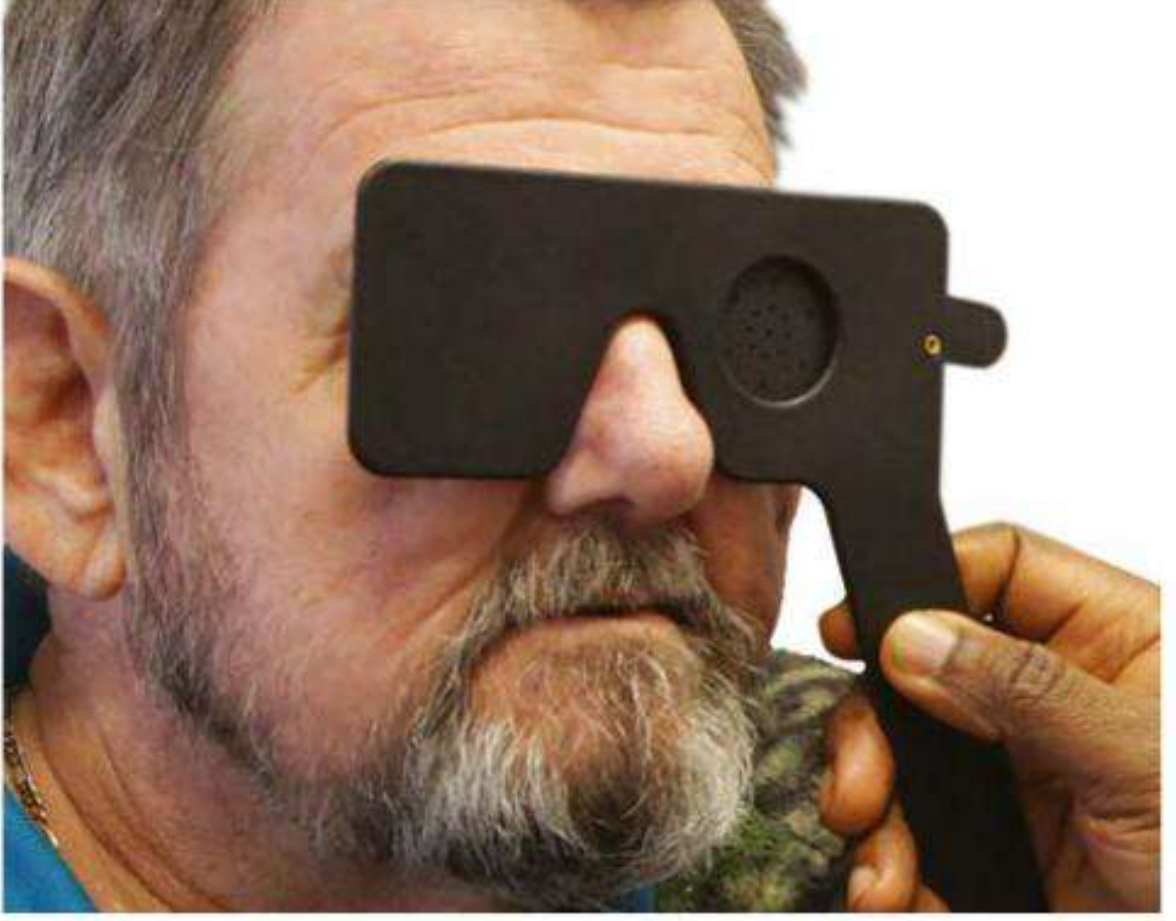
Purpose: The pinhole (a 1 mm aperture in an opaque disc) eliminates the effect of refractive error by allowing only a narrow shaft of light to reach the fovea. This bypasses the need for correct optical focusing.
When to use: If VA is less than 6/6, repeat the test with the pinhole in place.
Interpretation:
- VA improves with pinhole → vision loss is due to uncorrected refractive error (myopia, hyperopia, astigmatism) or media opacity (e.g. cataract)
- VA does not improve (or worsens) with pinhole → vision loss is likely due to a retinal, macular, or neurological cause
- Note: In macular disease and posterior lens opacities, pinhole VA may actually be worse than with spectacle correction
- Kanski's Clinical Ophthalmology, p. 16
When vision is too poor for the Snellen chart
Record progressively:
| Level | Definition |
|---|---|
| Counting Fingers (CF) | Patient correctly counts fingers held up by examiner, usually at 1 metre. Record as "CF at 1 m" |
| Hand Movements (HM) | Patient can detect that the examiner's hand is moving, held close in front |
| Perception of Light (PL) | Patient can only detect the presence of light (e.g. a pen torch) - no shape or movement |
| No Perception of Light (NPL) | No light detected at all |
For PL, also test projection of light - can the patient identify the direction from which light comes (superior, inferior, nasal, temporal)? If yes, the photoreceptors are intact in that quadrant. A dense cataract with an intact retina should give accurate projection in all four quadrants.
Alternative Distance Charts
- Tumbling E / Illiterate E chart: Patient indicates the direction the letter "E" is pointing (up/down/left/right) - used for illiterate patients or children >3.5 years
- Landolt C chart: Patient identifies the gap position in a broken ring - used internationally
- Numbers chart: For patients who know numbers but not letters
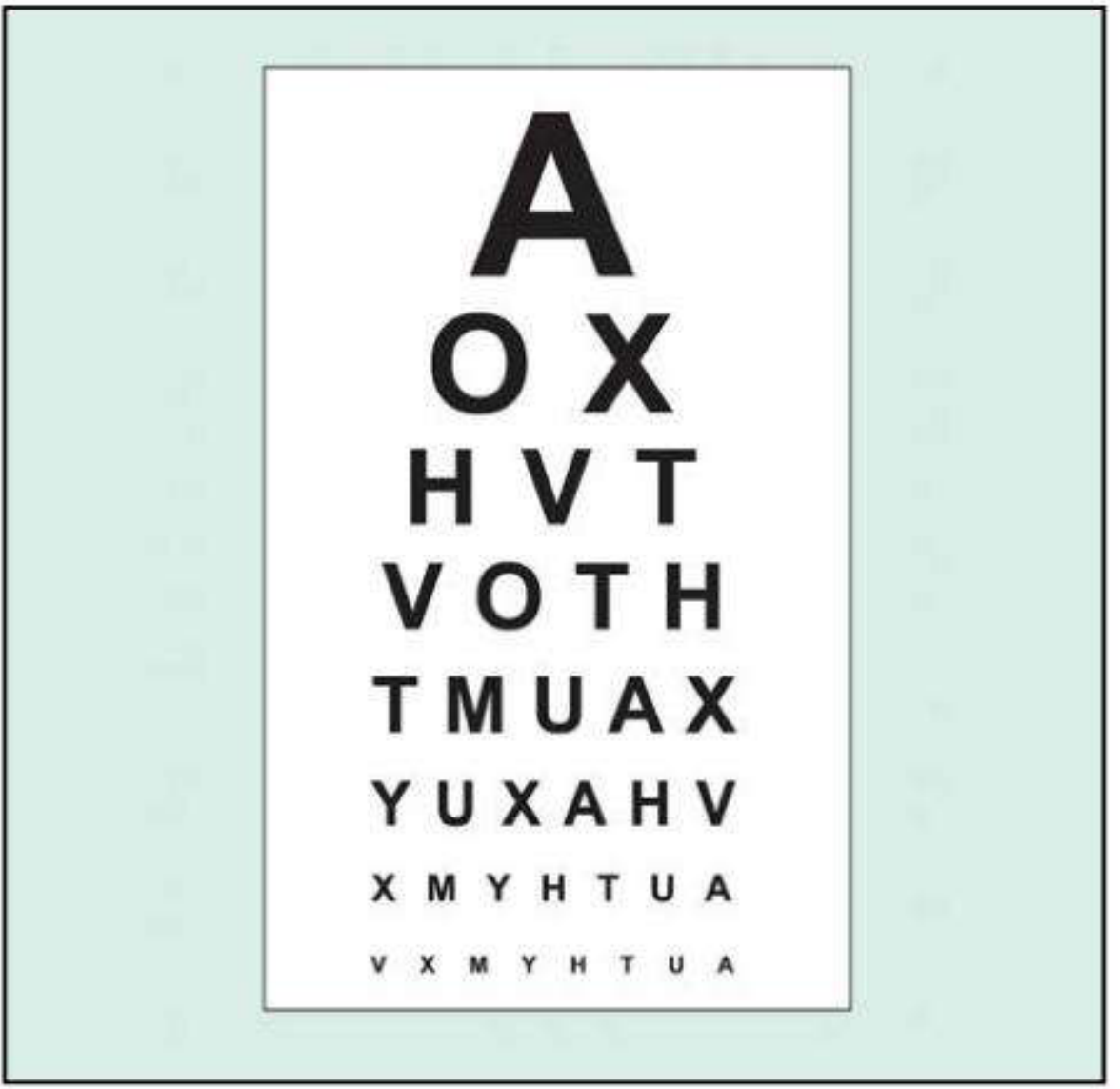
- HOTV chart (children): Wall chart with only H, O, T, V; child matches to a handheld board - suitable for ages 3-5 years
- Allen card test (very young children): Flashcards with 7 simple pictures; tested at varying distances; recorded as e.g. 15/30 (equivalent to 20/40)
- Textbook of Family Medicine, 9th ed.
LogMAR and ETDRS Charts (Research/Clinical Standard)
LogMAR = Logarithm of the Minimum Angle of Resolution. Increasingly the standard in clinical research and ophthalmology clinics.
- ETDRS chart (Early Treatment Diabetic Retinopathy Study): Uses balanced rows of Sloan optotypes, equal numbers of letters per row (controls for "crowding"), more accurate and reproducible than Snellen
- Tested at 4 metres
Snellen vs LogMAR conversion:
| Snellen (metric) | Snellen (imperial) | LogMAR |
|---|---|---|
| 6/6 | 20/20 | 0.00 |
| 6/12 | 20/40 | 0.30 |
| 6/60 | 20/200 | 1.00 |
| Better than 6/6 | Better than 20/20 | Negative value |
LogMAR 0.00 = normal; higher numbers = worse vision
- Kanski's Clinical Ophthalmology, p. 17
Part 2: Near Vision Testing
Purpose
Near vision testing evaluates the ability to read at close range (~33-40 cm). It is essential for detecting presbyopia (age-related loss of accommodation), macular disease, and verifying reading glasses.
Jaeger Near Vision Card
The most common near vision test at the bedside and in clinics.
How to perform:
- Hold the Jaeger card at 14-16 inches (35-40 cm) from the eyes - a comfortable reading distance - or ask the patient to hold it where they normally read
- Measure and record the exact distance used
- Test each eye separately with the other occluded
- Patient wears reading glasses if they have them
- Record the smallest print size the patient can read
Jaeger notation:
| Jaeger | Distance Equivalent | Description |
|---|---|---|
| J1 | 20/20 (6/6) | Normal near vision |
| J2 | 20/25 | |
| J3 | 20/32 | |
| J5 | 20/40 | |
| J7 | 20/50 | |
| J9 | 20/63 | |
| J13 | 20/100 | |
| J16 | 20/200 | Very poor near vision |
J1 = normal; higher numbers = worse near vision
- Adams & Victor's Principles of Neurology, 12th ed., p. 251
Other Near Vision Charts
- LogMAR near charts: More standardised; text size described in M-notation (e.g. 1M = standard newspaper print at 40 cm)
- ETDRS near version: Same optotypes as distance ETDRS chart, used at a fixed distance
- Reading test types (test-type book): Book held at comfortable reading distance; actual distance measured and recorded
- Kanski's Clinical Ophthalmology, p. 17
If no chart is available: ask the patient to read a magazine or newspaper at arm's length; if unable, note the closest distance at which they can read or count fingers.
Summary: Key Differences
| Feature | Distance Vision | Near Vision |
|---|---|---|
| Chart | Snellen / LogMAR / ETDRS | Jaeger / near card / test-type |
| Testing distance | 6 m (20 ft) | 33-40 cm (14-16 in) |
| Notation | 6/6 metric or 20/20 | J1-J16 or M-notation |
| Correction worn | Distance glasses | Reading glasses |
| Pinhole useful? | Yes | Less commonly used |
| Tests for | Myopia, hyperopia, retinal/macular disease | Presbyopia, macular disease, near refractive error |
General Rules for All Visual Acuity Testing
- Always test each eye separately - occlude the other eye completely
- Test worse eye first so the better eye result doesn't bias the patient's confidence
- Wear the appropriate correction (distance glasses for far, reading glasses for near)
- Encourage the patient to read every letter even if uncertain - guessing correctly still counts
- Record precisely: note whether VA is unaided, with correction, or with pinhole
- Binocular VA (both eyes open) is usually slightly better than the better monocular VA and is sometimes recorded separately
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Adams & Victor's Principles of Neurology, 12th ed. | Textbook of Family Medicine, 9th ed. | Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.