Cavernous sinus anatomy and cavernous sinus thrombosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cavernous sinus thrombosis" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Make 20 marks university answer for this
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive 20-mark university answer. Here it is:
Cavernous Sinus: Anatomy and Cavernous Sinus Thrombosis
PART A: ANATOMY OF THE CAVERNOUS SINUS (10 marks)
1. Location and Structure
The cavernous sinus is a paired dural venous sinus situated at the base of the skull, on either side of the body of the sphenoid bone and the sella turcica. It extends from the apex of the orbit anteriorly to the apex of the petrous temporal bone posteriorly. Its walls are formed by a fold of the inner layer of dura mater - the medial and upper walls are continuous with the diaphragma sellae, while the posterolateral wall is medial to the trigeminal (Meckel's) cave, which itself contains the trigeminal ganglion. - Scott-Brown's Otorhinolaryngology, Vol. 2
The sinus is not a simple channel; it is a plexus of interconnecting venous channels ("cavernous" refers to its cave-like trabeculated structure).
2. Contents
The cavernous sinus contains several critically important structures arranged in two groups:
Within the lateral dural wall (from superior to inferior):
| Cranial Nerve | Function |
|---|---|
| CN III (Oculomotor) | Levator palpebrae, superior/medial/inferior rectus, inferior oblique, pupil constriction |
| CN IV (Trochlear) | Superior oblique muscle |
| CN V1 (Ophthalmic division of Trigeminal) | Sensation - forehead, eye, nose |
| CN V2 (Maxillary division of Trigeminal) | Sensation - cheek, upper lip, upper teeth |
Running medially/inferiorly within the sinus itself:
- CN VI (Abducens) - runs inferolaterally within the sinus (most vulnerable to raised ICP)
- Internal Carotid Artery (ICA) - the main content; enters through the foramen lacerum at the petrous apex, courses upward, forward, and medially, then perforates the dura just posterior to the optic canals to enter the middle cranial fossa
- Sympathetic plexus - travels along the ICA wall (carries Horner's pathway fibers)
Clinical mnemonic for lateral wall contents (superior to inferior): O T Om Ma - Oculomotor, Trochlear, Ophthalmic, Maxillary (CN III, IV, V1, V2)
The arrangement means that any lesion of the cavernous sinus may produce any combination of III, IV, V1, V2, and VI nerve palsies along with a Horner syndrome. - Wills Eye Manual; Harrison's Principles of Internal Medicine, 22e
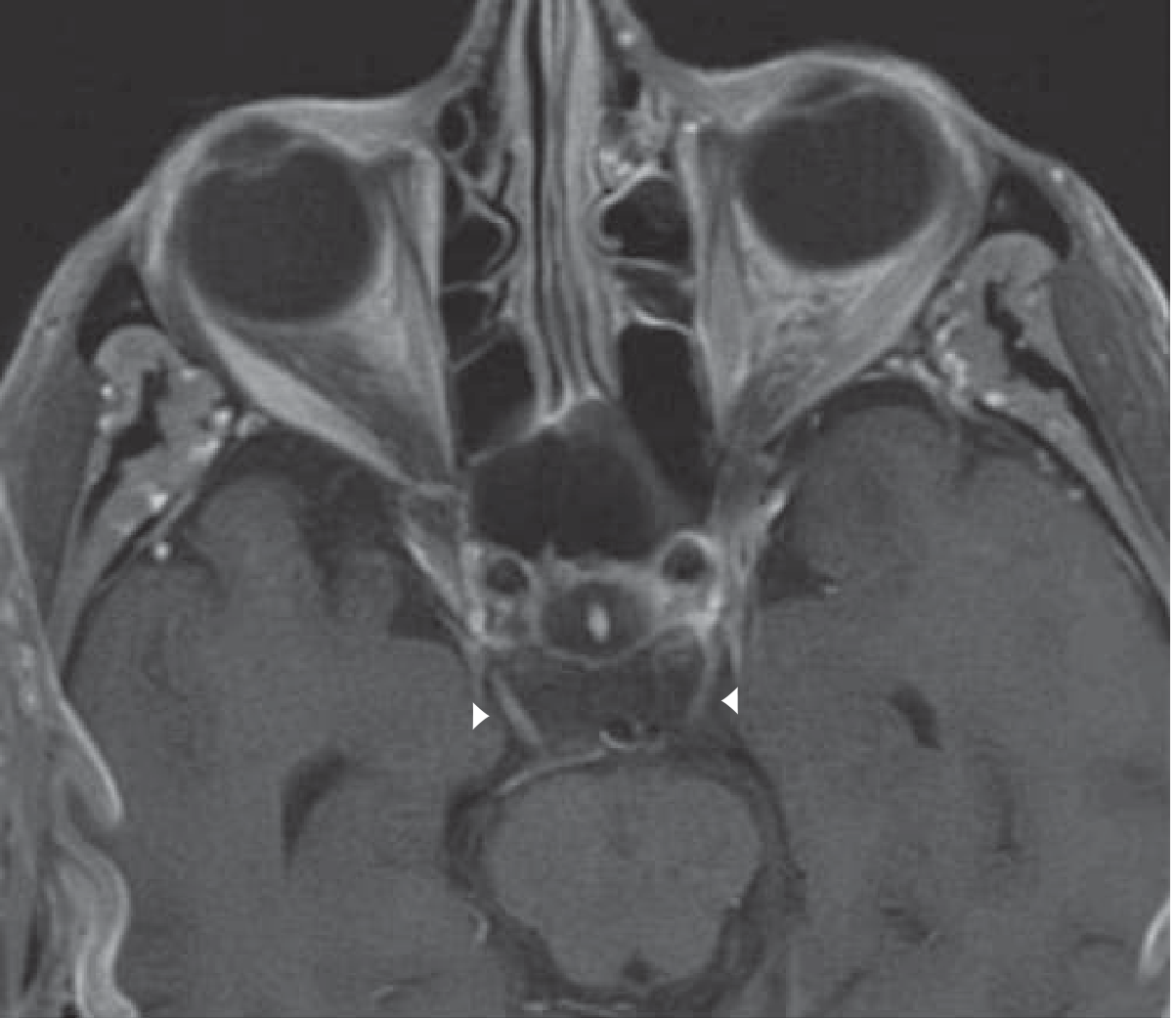
Axial MRI showing bilateral cavernous sinus region - note the oculomotor nerve enhancement (arrowheads). Bradley and Daroff's Neurology in Clinical Practice
3. Venous Drainage and Communications
The cavernous sinus receives blood from:
- Superior and inferior ophthalmic veins (draining the orbit and face)
- Superficial middle cerebral veins (draining the cerebral hemispheres)
- Sphenoparietal sinus
It drains via:
- Superior petrosal sinus → transverse/sigmoid sinus → internal jugular vein
- Inferior petrosal sinus → directly into the internal jugular vein
- Pterygoid venous plexus via emissary veins through the foramen ovale (or foramen of Vesalius)
The two cavernous sinuses communicate with each other via:
- The intercavernous (circular) sinus - which runs anterior and posterior to the pituitary stalk
- This connection is clinically important: unilateral infection can spread to become bilateral CST
The pterygoid plexus communicates with the cavernous sinus via a connecting vein through the foramen ovale, and with the facial vein via the inferior ophthalmic vein. These connections explain the pathway by which dental, facial, or orbital infections spread to the cavernous sinus. - Scott-Brown's Otorhinolaryngology, Vol. 2
4. Relations
- Medial: Pituitary gland (in the sella turcica) and sphenoid sinus
- Superior: Optic chiasm and optic tract
- Lateral: Temporal lobe
- Inferior: Foramen lacerum and petrous apex
- Anterior: Superior orbital fissure (continuation into the orbit)
PART B: CAVERNOUS SINUS THROMBOSIS (CST) (10 marks)
1. Definition and Pathophysiology
Cavernous sinus thrombosis (CST) is clotting within the cavernous sinus, most commonly resulting from septic thrombophlebitis - a potentially devastating condition with significant mortality if not recognized and treated urgently.
Infection spreads to the cavernous sinus by two main routes:
- Via the superior and inferior ophthalmic veins from orbital cellulitis, preseptal cellulitis, or facial infections
- Via emissary veins directly from sphenoid and ethmoid sinusitis
Bacteria are themselves pro-thrombotic; septic emboli and thrombophlebitis propagate centrally from the paranasal sinuses and orbit to the cavernous sinus. As the sinuses communicate, bilateral involvement develops via the intercavernous sinus - a hallmark of CST. - Harrison's Principles of Internal Medicine, 22e; Scott-Brown's Vol. 1
2. Aetiology and Risk Factors
Most common primary sites of infection:
- Sphenoid and ethmoid sinusitis (most frequent)
- Orbital/periorbital cellulitis
- Dental infections (upper teeth/jaw)
- Furunculosis of the mid-face ("danger triangle of the face")
- Otitis media/mastoiditis (less common)
- Intracranial procedures
Common causative organisms:
- Staphylococcus aureus - most common (including MRSA)
- Streptococcus species (including anaerobic streptococci)
- Gram-negative organisms
- Anaerobes (in dental origin)
- Aspergillus and Mucor species in immunocompromised/diabetic patients (angioinvasive fungi) - Harrison's Principles of Internal Medicine, 22e; Kanski's Clinical Ophthalmology, 10e
CST accounts for approximately 9% of intracranial complications of rhinosinusitis. - Scott-Brown's Otorhinolaryngology, Vol. 2
3. Clinical Features
CST presents with a combination of septic features plus localizing signs from the cranial nerve contents of the cavernous sinus:
Systemic features:
- High spiking fever, rigors, malaise
- Severe headache (frontal or retroorbital)
- Nausea, vomiting
- Altered consciousness, confusion
Ocular and orbital features (from venous congestion):
- Proptosis (exophthalmos)
- Chemosis (conjunctival oedema)
- Periorbital oedema
- Congestion of facial, conjunctival, and retinal veins
- Papilloedema
Cranial nerve palsies (due to CN involvement within the sinus):
- CN III: Ptosis, mydriasis, "down and out" eye position
- CN IV: Weakness of superior oblique - vertical diplopia
- CN VI: Lateral gaze palsy (abducens most vulnerable due to intra-sinus position)
- CN V1/V2: Facial numbness/hyperesthesia, decreased corneal reflex, periorbital/cheek paraesthesia
- Sympathetic fibers: Horner syndrome (ptosis + miosis + anhidrosis)
Key distinguishing feature: bilateral signs developing from initially unilateral disease, due to spread via the intercavernous sinus. Unilateral CST can become bilateral within 24-48 hours.
Signs of meningeal irritation: Nuchal rigidity, Kernig's sign, Brudzinski's sign (when meningitis co-exists)
- Harrison's Principles of Internal Medicine, 22e; Kanski's Clinical Ophthalmology, 10e; Scott-Brown's Vol. 1 & 2
4. Investigations
Imaging (most important):
| Investigation | Findings in CST |
|---|---|
| MRI with gadolinium | Absent T2 flow void; sinus expansion; abnormal signal in cavernous sinus; filling defects |
| MR venography (MRV) | Absence of flow in thrombosed sinus - most sensitive modality |
| CT venography (CTV) | Expanded cavernous sinus, filling defects |
| Plain CT | May appear normal in early stages - do NOT exclude CST on normal CT |
Important: In early CST, CT scans may appear normal. CT and MR venography are complementary and both should be used. - Scott-Brown's Vol. 1; Grainger & Allison's Diagnostic Radiology
Laboratory:
- FBC (leukocytosis), CRP, procalcitonin, ESR
- Blood cultures (before antibiotics if possible)
- Coagulation screen (PT, APTT, fibrinogen)
- Lumbar puncture - if no contraindication, to exclude meningitis (CSF may show raised protein, pleocytosis)
- Culture from primary source (sinus aspirate, wound swab)
5. Prognosis
- Mortality: 20% treated; up to 100% untreated (Kanski's Clinical Ophthalmology)
- Adult sinusitis-related CST mortality: approximately 30%
- Morbidity (surviving patients): up to 50% experience residual cranial nerve palsies, blindness, or other neurological deficits
- Relapse and recurrence of meningeal/ocular signs have been reported up to 6 weeks after apparent recovery - Scott-Brown's Vol. 1
6. Treatment
Treatment must be initiated urgently; this is a neurosurgical emergency.
A. Antibiotics (mainstay of treatment):
- IV broad-spectrum antibiotics covering S. aureus, streptococci, gram-negatives, and anaerobes
- Regimen typically includes: anti-staphylococcal penicillin (or vancomycin if MRSA suspected) + a third-generation cephalosporin + metronidazole
- Duration: at least 2 weeks beyond clinical resolution (bacteria sequestered in thrombus are not killed until dural sinuses begin to recanalize)
- Prolonged follow-up for at least 6 months due to risk of late relapse
B. Anticoagulation (controversial):
- Arguments for: Prevents thrombus propagation; anti-inflammatory properties; may improve outcomes
- Arguments against: Thrombus may wall off infection; risk of intracranial haemorrhage in inflamed environment
- Current practice: Use if no contraindication (no intracerebral haemorrhage on imaging); start with unfractionated heparin infusion (APTT target 1.5-2x normal); switch to low-molecular weight heparin once condition improves
- Anticoagulation is specifically recommended for septic CST complicating bacterial meningitis with progressive neurological deterioration despite antibiotics - Harrison's Principles of Internal Medicine, 22e; Scott-Brown's Vol. 1
C. Surgical:
- Drainage of the primary source (paranasal sinus endoscopic surgery - FESS; drainage of orbital abscess if present)
- Surgery of the sinuses draining poorly: addresses the infective nidus
- No direct surgical drainage of the cavernous sinus itself
- Multidisciplinary approach: ENT + Neurosurgery + Ophthalmology + Infectious Disease
D. Adjunctive measures:
- IV hydration
- Corticosteroids: sometimes added to reduce inflammation (used in Tolosa-Hunt syndrome; adjunctive role in CST remains debated)
- Regular eye monitoring (visual acuity, colour vision, pupillary reflex, range of movements - at minimum twice daily, or 4-6 hourly if deteriorating)
7. Differential Diagnosis of Cavernous Sinus Syndrome
| Condition | Key Features |
|---|---|
| Tolosa-Hunt syndrome | Idiopathic, painful, steroid-responsive; diagnosis of exclusion |
| Pituitary apoplexy | Sudden-onset, visual loss, hormonal disturbance |
| Intracavernous carotid aneurysm | Pulsatile, may cause CN VI palsy |
| Carotid-cavernous fistula | Pulsatile proptosis, bruit, dilated episcleral vessels |
| Orbital apex syndrome | Adds optic nerve dysfunction (proptosis + visual loss) |
| Nasopharyngeal carcinoma | Insidious onset, no fever, weight loss |
| Meningioma/lymphoma | Steroid-responsive, recurs on taper |
| Mucormycosis | Diabetic/immunocompromised; black eschar in nose |
- Localization in Clinical Neurology, 8e; Wills Eye Manual; Adams & Victor's Principles of Neurology, 12e
Summary Table
| Feature | Detail |
|---|---|
| Location | Paired dural sinus, base of skull, bilateral to sella turcica |
| Lateral wall (superior→inferior) | CN III, IV, V1, V2 |
| Intra-sinus contents | CN VI, ICA, sympathetic plexus |
| Venous inflow | Superior/inferior ophthalmic veins, sphenoparietal sinus |
| Venous outflow | Superior/inferior petrosal sinuses |
| Commonest cause of CST | Sphenoid/ethmoid sinusitis; orbital cellulitis |
| Commonest organism | Staphylococcus aureus |
| Classic signs | Fever, proptosis, chemosis, ophthalmoplegia, bilateral signs |
| Imaging of choice | MRI + MR venography |
| Mortality (untreated) | Up to 100%; treated ~20% |
| Treatment | IV antibiotics ≥2 weeks + consider anticoagulation + surgical drainage of primary source |
Sources: Harrison's Principles of Internal Medicine 22e | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 & 2 | Kanski's Clinical Ophthalmology 10e | Bradley and Daroff's Neurology in Clinical Practice | Wills Eye Manual | Localization in Clinical Neurology 8e | Grainger & Allison's Diagnostic Radiology | Adams and Victor's Principles of Neurology 12e
This is a shared conversation. Sign in to Orris to start your own chat.