Hi
Hi! How can I help you today?
Heart failure
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"heart failure preserved ejection fraction" AND treatment
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, medical-student-oriented overview of HFpEF management, synthesized from Braunwald's, Harrison's, Goldman-Cecil, and Goodman & Gilman's.
Management of Heart Failure with Preserved Ejection Fraction (HFpEF)
What is HFpEF?
HFpEF is defined as typical heart failure symptoms with a left ventricular ejection fraction (LVEF) >50%. It accounts for roughly half of all HF cases, is more common in women, and its prevalence rises sharply with age. The typical patient is an older woman with hypertension, obesity, diabetes, and atrial fibrillation. The key pathophysiology is impaired diastolic relaxation and increased ventricular stiffness (from hypertrophy and fibrosis) - not a pump problem, but a filling problem.
Unlike HFrEF (where ACEi/ARB, beta-blockers, MRAs, and ARNIs have all shown clear mortality benefits), no single drug has conclusively reduced mortality in HFpEF. Management is therefore organized around three pillars: symptom relief, risk factor control, and emerging disease-modifying therapy.
Pillar 1 - Symptom Relief (Decongestion)
Diuretics (loop diuretics, e.g., furosemide) are the cornerstone of symptom management.
- Reduce pulmonary congestion and edema
- Must be used carefully - the non-compliant ventricle operates in a narrow filling window. Overdiuresis drops cardiac output and can cause prerenal azotemia
Pillar 2 - Risk Factor Control (the most important interventions)
| Target | Why it matters | Intervention |
|---|---|---|
| Hypertension | Leading cause; LVH and fibrosis drive stiffness | Treat to guideline targets |
| Coronary artery disease | Ischemia worsens diastolic relaxation | Revascularization if indicated |
| Atrial fibrillation | Loss of atrial kick - major cause of acute decompensation | Rhythm control preferred; rate control if needed |
| Obesity | Chronic inflammation, volume expansion | Caloric restriction + aerobic exercise |
| Diabetes / insulin resistance | Metabolic cardiomyopathy | Tight glycaemic control, especially SGLT2i |
| Sleep apnea | Pulmonary HTN, systemic HTN, right heart dysfunction | Screening + CPAP/BiPAP |
| Tachycardia | Limits filling time; patients tolerate it poorly | Heart rate control (beta-blocker or rate-limiting CCB in AF) |
Pillar 3 - Pharmacologic Therapy (what works and what doesn't)
What NOW works - SGLT2 inhibitors (first-line)
Dapagliflozin and empagliflozin (10 mg once daily) are the most important pharmacologic advances in HFpEF:
- Reduce HF hospitalization and cardiovascular mortality
- Improve symptoms and health-related quality of life
- Katzung calls them "first-line therapy for HFpEF"; Goldman-Cecil endorses them for LVEF ≥50%
- Key trials: EMPEROR-Preserved (empagliflozin) and DELIVER (dapagliflozin)
What may help in selected patients
| Drug class | Evidence | Best candidates |
|---|---|---|
| MRA (spironolactone) | TOPCAT trial - reduced HF hospitalizations by 17%, but missed the primary composite endpoint; post-hoc benefit in Americas cohort | Consider in patients without significant renal impairment or hyperkalemia |
| ARNI (sacubitril-valsartan) | PARAGON-HF - borderline significance (p=0.06); benefit mostly in women and those with EF <57% (i.e., mildly reduced end of the spectrum); now FDA-approved across the full EF spectrum | Consider especially in HFmEF (EF 41-49%) |
| ARBs (candesartan) | CHARM-Preserved - reduced HF hospitalizations, no mortality benefit | Second-line if ARNI not tolerated |
| GLP-1 agonists (semaglutide, liraglutide) | Improve QOL and exercise capacity in obese HFpEF regardless of diabetic status | Obese patients (BMI >35) |
What does NOT work in HFpEF
| Drug | Evidence |
|---|---|
| ACE inhibitors | PEP-CHF - early apparent benefit attenuated at longer follow-up |
| Beta-blockers | No dedicated HFpEF trial; nebivolol subgroup analysis negative. Still useful for rate control in AF |
| Digoxin | DIG Ancillary Trial - no mortality or hospitalization benefit |
| Sildenafil (PDE5 inhibitor) | Failed to improve outcomes despite promising mechanistic rationale (titin phosphorylation via cGMP) |
| Isosorbide mononitrate | Actually worsens activity levels in HFpEF |
| Ivabradine | No benefit on exercise capacity |
Treatment Algorithm (Goldman-Cecil / ACC-AHA 2022)
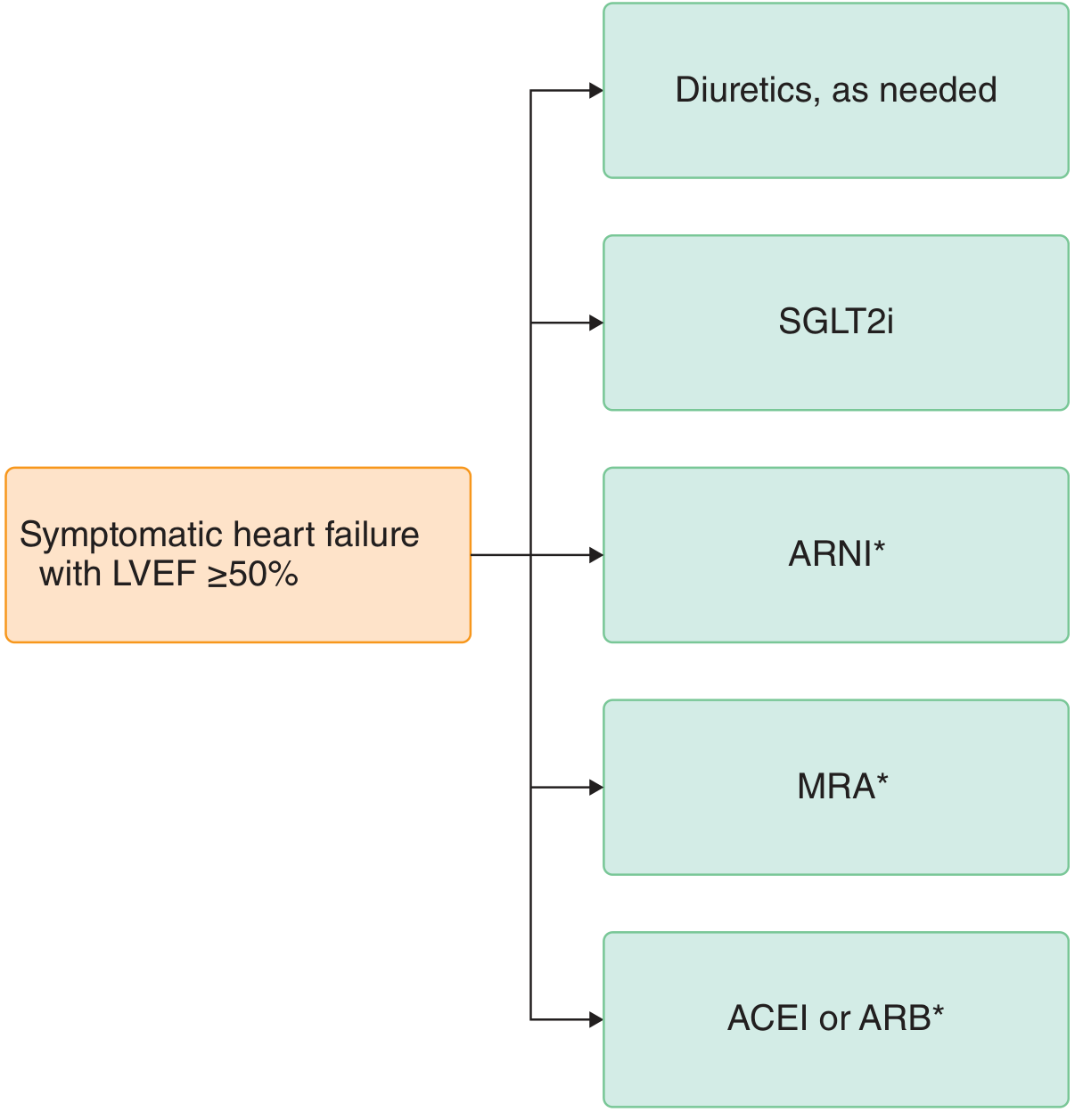
* = greater benefit when LVEF is closer to 50% (i.e., toward the HFmEF range)
Non-Pharmacologic Interventions
- Aerobic exercise - the only intervention consistently shown to increase peak VO2 and improve exercise capacity in HFpEF
- Weight loss (caloric restriction + exercise) - provides additional benefit in obese patients on top of exercise alone
- Dietary sodium restriction - avoid excess salt and fluid
Key Exam Points to Remember
- SGLT2 inhibitors are now first-line pharmacologic therapy for HFpEF - this is a major paradigm shift from older editions of textbooks.
- No drug has proven mortality benefit in pure HFpEF; the wins so far are reduced hospitalization and better QOL.
- The closer the EF is to 50% (HFmEF range), the more the HFrEF drugs carry over (ARNIs, MRAs, ARBs).
- Atrial fibrillation is both common and dangerous in HFpEF - the stiff ventricle depends heavily on atrial kick; losing it can precipitate acute decompensation.
- Overdiuresis is a real risk - the narrow filling window of the non-compliant ventricle means too little volume is just as bad as too much.
Sources:
- Braunwald's Heart Disease (10e), p. 1035
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 265
- Goldman-Cecil Medicine, p. 492 (Fig. 46-6)
- Katzung's Basic and Clinical Pharmacology (16e), p. 347
- Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.