43 day old male baby Incessant cry for past 5 days Baby given drops para Drops gastica Drops cpm Well for some time and again cries Doesn't crt during urination and ear clear Tenderness and guarding present on palpating abdomen B/L testes present inside scrotum Baby sent for USG abdomen. What can be the diagnosis and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have thorough textbook content. Let me synthesize a comprehensive clinical answer.
Clinical Analysis: 43-Day-Old Male with Incessant Crying + Abdominal Tenderness/Guarding
This is a surgical emergency until proven otherwise. The combination of persistent crying for 5 days, abdominal tenderness, and guarding in a 43-day-old male goes well beyond infantile colic. Here is a structured differential and management approach:
Most Likely Diagnoses
🔴 1. Incarcerated/Strangulated Inguinal Hernia — TOP PRIORITY
This is the most dangerous and most likely surgical cause at this age.
Why it fits:
- 43-day-old male → highest risk age group for incarceration (narrow inguinal ring, patent processus vaginalis)
- Males have 10:1 predominance, right side more common
- Inconsolable crying + abdominal tenderness + guarding = hallmarks of incarceration
- The fact that bilateral testes are present in scrotum helps rule out undescended testis but does not rule out an inguinal hernia — the hernia may not be visibly bulging if edema or the examiner hasn't specifically palpated the inguinal canal
"If the incarceration has been present for several hours, the infant may be inconsolable and have feeding intolerance, pain, abdominal distention, vomiting, and lack of flatus or stool, signaling complete intestinal obstruction." — Mulholland & Greenfield's Surgery, 7e
What to do RIGHT NOW:
- Carefully palpate both inguinal canals for a firm, non-reducible mass
- USG abdomen/groin (already sent) — will show the bowel loop/omentum in the canal
- If confirmed → urgent surgical referral for manual reduction under sedation or emergency herniorrhaphy
🟠 2. Intussusception — Urgent Consideration
Why it fits:
- Peak age 6 weeks–3 years, but can occur in neonates
- Classic triad: colicky abdominal pain + vomiting + bloody stool (currant-jelly stool)
- Crying with legs drawn to abdomen, episodic nature ("well for some time and again cries")
- Abdominal mass may be palpable in right abdomen (80–90% of cases)
- Guarding develops as obstruction and ischemia progress
"The typical infant develops acute onset of severe, colicky abdominal pain. Intermittent episodes of irritability and crying may be associated with drawing the legs up to the abdomen. Between bouts of colic, the infant is often lethargic or sleepy." — Mulholland & Greenfield's Surgery, 7e
What USG will show: Target sign / bull's-eye sign (intussusceptum within intussuscipiens)
Treatment:
- Hemodynamically stable + no peritonitis → pneumatic or hydrostatic enema reduction (60–90% success)
- Peritonitis present → immediate surgical exploration
- Failed enema → operative manual reduction or resection
- Recurrence: ~5%, usually managed with repeat enema
🟡 3. Infantile Colic — Diagnosis of Exclusion ONLY
Infantile colic:
- Peaks at 5–6 weeks, typically resolves by 3–4 months
- Characterized by inconsolable crying, legs drawn up, abdominal distension, excessive gas
- Diagnosis requires ruling out ALL organic causes first
"Although we tend to think of colic as an abdominal process, a complete evaluation of all organ systems must be performed. Other causes of inconsolable crying [must be excluded]." — Swanson's Family Medicine Review
Critical point: Infantile colic does NOT cause abdominal tenderness or guarding. The presence of these signs makes a surgical cause mandatory to exclude before diagnosing colic. The drops given (paracetamol, simethicone/gripe water, CPM) providing only partial/temporary relief is another red flag.
🟡 4. Other differentials to consider
| Condition | Feature pointing to it | Feature against it |
|---|---|---|
| Hirschsprung's enterocolitis | Age, abdominal distension | No mention of failure to pass meconium, no explosive diarrhea |
| Mesenteric adenitis / viral peritonitis | Abdominal tenderness | Less common at this age |
| FPIES (Food protein-induced enterocolitis) | Age, irritability | Usually vomiting/diarrhea prominent |
| Urinary tract infection | Common cause of crying in infants | No dysuria (no crying on urination), no fever mentioned |
| Hair tourniquet syndrome | Easy to miss | Ears checked; genitals and digits should also be checked |
Immediate Action Plan
- Do not send home — this baby needs urgent evaluation
- Examine inguinal canals carefully — any firm bulge = surgical emergency
- Check digits, toes, penis for hair tourniquet (quick, easy to miss)
- USG abdomen + groin (already ordered) — look for:
- Bowel in inguinal canal (hernia)
- Target/bull's-eye sign (intussusception)
- Free fluid, dilated bowel loops
- Bloods: CBC, CRP, electrolytes, blood gas if unwell
- Surgical referral immediately if USG confirms hernia or intussusception
- If incarcerated hernia found on USG/exam:
- IV access + IV fluids
- Attempt gentle manual reduction with sedation
- If irreducible → emergency surgery
Key Teaching Point
Abdominal tenderness + guarding in an infant = surgical abdomen until proven otherwise. The partial response to paracetamol/simethicone/antihistamine (CPM) and return of symptoms suggests an underlying structural/surgical pathology, not simple colic. The USG is the right next step, but clinical re-examination of the inguinal canals is critical and should precede waiting for the USG report.
Sources: Mulholland & Greenfield's Surgery, 7e; Schwartz's Principles of Surgery, 11e; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Swanson's Family Medicine Review
Create a diagnostic flowchart for persistent infant crying with physical findings
Generating Image
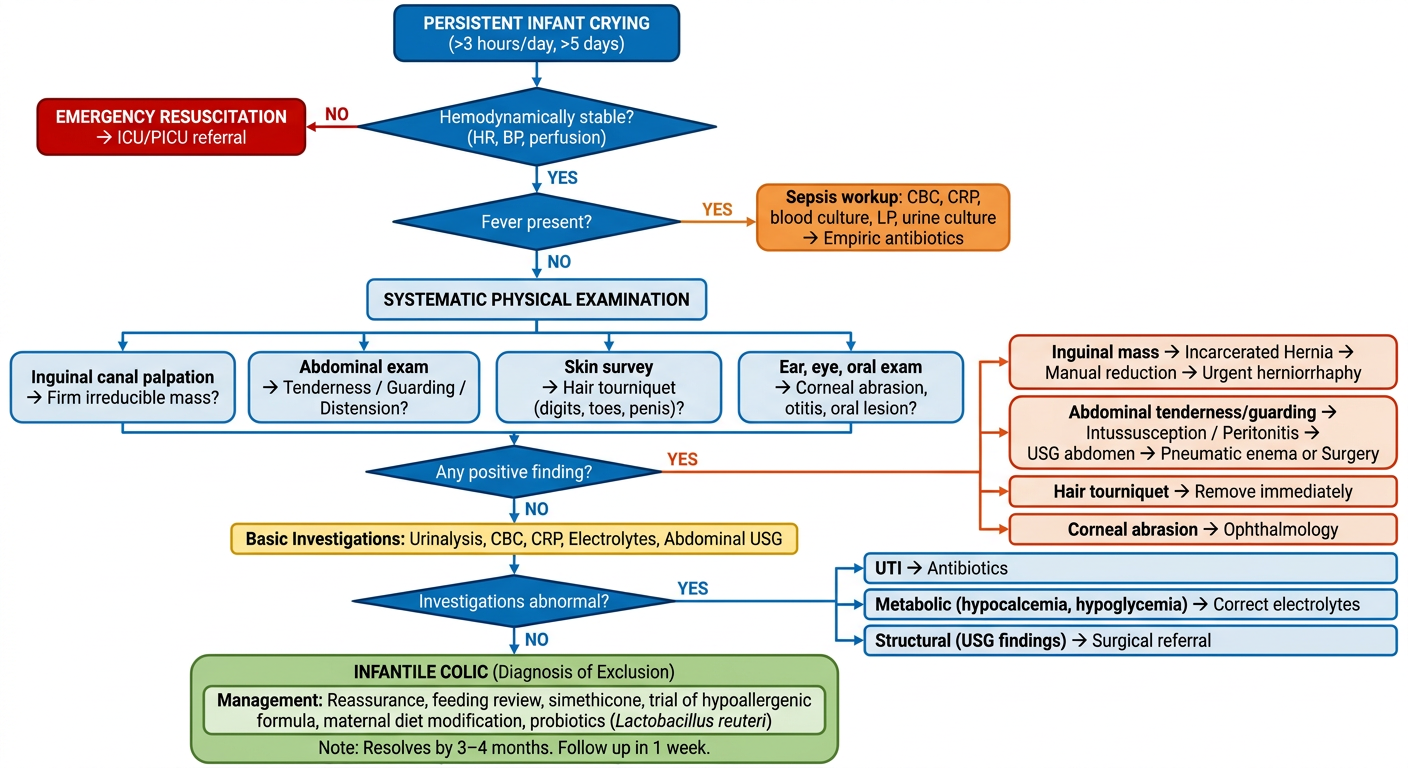
Here is the diagnostic flowchart. It follows a stepwise clinical approach:
Flow summary:
- Hemodynamic stability — first and immediate check; unstable infants go directly to resuscitation
- Fever screen — triggers sepsis workup and empiric antibiotics if present
- Systematic physical exam — four parallel tracks covering the most common and most dangerous causes:
- Inguinal canals (incarcerated hernia)
- Abdomen (intussusception, peritonitis)
- Skin/digits/genitalia (hair tourniquet)
- Eyes/ears/mouth (corneal abrasion, otitis, oral lesions)
- Positive finding → color-coded urgent/surgical pathways with specific management
- Investigations (USG, urinalysis, CBC, CRP, electrolytes) if exam is normal
- Infantile colic — only after all organic causes are excluded (green, bottom)
Key principle embedded in the chart: Abdominal tenderness and guarding are red flags that bypass the colic pathway entirely — directly into surgical evaluation. This directly reflects the clinical scenario of your 43-day-old patient.
What are the Meternal diet modification
Finding Sources
Searching PubMed
maternal diet modification breastfeeding infantile colic
Finding Sources
Searching PubMed
maternal diet infantile colic breastfed
Finding Sources
Finding Sources
Finding Sources
Searching the Web
maternal diet modification infantile colic breastfeeding evidence 2023 2024
Reading File
Here is a comprehensive, evidence-based guide to maternal diet modifications for infantile colic in breastfeeding mothers:
Maternal Diet Modification for Infantile Colic
Applies to: Breastfeeding mothers only. Formula-fed infants require formula changes (hypoallergenic/hydrolyzed), not maternal diet changes.
Why Maternal Diet Matters
Food proteins from the mother's diet are secreted into breast milk and can sensitize or irritate the infant's immature gut. IgE-mediated and non-IgE-mediated hypersensitivity reactions account for colic in 10–15% of cases. Food allergen proteins — especially cow's milk protein — are the most well-studied trigger.
A Cochrane review found that 74% of colicky infants responded to a low-allergen maternal diet vs. only 37% on a standard diet (p<0.001).
Step-by-Step Approach
Step 1 — Cow's Milk Protein Elimination (First Line)
Most evidence-based and most impactful step.
- Eliminate all dairy products: milk, cheese, yoghurt, butter, ghee, cream, ice cream, whey protein
- Cow's milk protein is the #1 dietary trigger in breastfed colicky infants
- Duration: Trial for 2 weeks minimum — symptoms usually improve within 3–7 days if cow's milk is the trigger
- Rechallenge: Reintroduce after 3–4 weeks to confirm causality
- Ensure the mother gets calcium from alternate sources: fortified plant milk, sesame seeds, broccoli, ragi (finger millet), almonds
Step 2 — Broader Low-Allergen Diet (If Step 1 Fails)
Eliminate the "Big 7" allergens simultaneously:
| Food to Avoid | Reason | Hidden Sources to Watch |
|---|---|---|
| Cow's milk / dairy | Most common trigger | Butter, ghee, casein in processed foods |
| Eggs | Common allergen | Baked goods, mayonnaise, pasta |
| Peanuts | Strong allergen | Peanut butter, mixed oils |
| Tree nuts | Allergen | Cashew, almond, walnut-based snacks |
| Wheat / gluten | Sensitizer | Bread, chapati, biscuits, pasta |
| Soy | Cross-reacts with cow's milk protein | Soy milk, tofu, soy sauce |
| Fish / shellfish | Allergen | Tuna, prawns, crabs |
"Significant reductions in colic symptoms have been observed in mothers who eliminated cow's milk, eggs, peanuts, tree nuts, wheat, soy, and fish from their diet." — Nutrition Guide for Clinicians (PCRM)
Step 3 — Gas-Producing Foods (Moderate Evidence)
These foods produce oligosaccharides and fermentable sugars that may pass into breast milk or increase maternal intestinal gas, potentially affecting the infant:
| Food Category | Examples |
|---|---|
| Cruciferous vegetables | Cabbage, broccoli, cauliflower, Brussels sprouts |
| Legumes | Rajma, chana, moong, lentils (especially if not well-cooked/soaked) |
| Onion and garlic | In large quantities |
| Carbonated drinks | Aerated drinks, soda |
| Spicy foods | Chilli, pepper in excess |
⚠️ Note: Evidence for this category is weaker than for allergen elimination. These foods are culturally important and need not all be avoided simultaneously — trial-and-error is appropriate.
Step 4 — Caffeine Reduction
- Limit to ≤200 mg/day (approximately 1–2 cups of tea or coffee)
- Excess caffeine in breast milk can cause infant irritability and sleep disturbance, mimicking colic
Step 5 — Fructose / Juice Avoidance (If Malabsorption Suspected)
- Some colicky infants have fructose malabsorption — detected by increased breath hydrogen excretion
- Mother should avoid fruit juices, sweetened drinks, high-fructose fruits in excess
- More relevant in formula-fed infants given fruit juices directly
Duration and Follow-Up Protocol
| Step | Duration | Action if No Response |
|---|---|---|
| Dairy elimination | 2 weeks | Proceed to full low-allergen diet |
| Full low-allergen diet | 2–4 weeks | Consider non-dietary causes |
| Rechallenge each food | Every 3–4 months | Determine if tolerance developed |
Important Practical Points
- Do not stop breastfeeding — breastfeeding itself is protective; only dietary modification is needed
- Nutritional supplementation during elimination diet:
- Calcium: 1000–1200 mg/day from non-dairy sources or supplements
- Vitamin D: Continue supplementation
- Vitamin B12: If vegan diet is being followed
- Maternal smoking cessation — smoking doubles the incidence of infantile colic (independent of diet)
- Dietitian referral is ideal for prolonged elimination diets to prevent maternal nutritional deficiency
- If no improvement after full dietary trial → consider Lactobacillus reuteri probiotic supplementation (for the infant) alongside dietary measures
Summary Table
| Intervention | Evidence Level | Priority |
|---|---|---|
| Cow's milk protein elimination | Strong (RCT, Cochrane) | ⭐⭐⭐ First line |
| Full low-allergen diet (Big 7) | Moderate (RCT) | ⭐⭐ If dairy-free fails |
| Avoid gas-producing foods | Weak/anecdotal | ⭐ Trial basis |
| Caffeine restriction | Moderate | ⭐⭐ Alongside dietary changes |
| Maternal smoking cessation | Strong | ⭐⭐⭐ Non-dietary but critical |
Sources: Swanson's Family Medicine Review; Sleisenger & Fordtran's GI & Liver Disease; Cochrane Review — Diet Changes for Infant Colic; PCRM Nutrition Guide for Clinicians
This is a shared conversation. Sign in to Orris to start your own chat.