Chronic obstructive pulmonary disease and restrictive disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"COPD" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed response.
COPD and Restrictive Lung Disease
The Fundamental Difference: Obstructive vs. Restrictive
The two broad categories of chronic lung disease are separated by a single key spirometric principle:
| Parameter | COPD (Obstructive) | Restrictive |
|---|---|---|
| FEV1 | Reduced | Reduced |
| FVC | Normal or reduced | Reduced |
| FEV1/FVC ratio | < 0.70 (reduced) | Normal or increased (>80%) |
| TLC | Normal or increased | Reduced |
| RV | Increased (air trapping) | Reduced or normal |
| DLCO | Reduced (esp. emphysema) | Reduced |
The classic spirometry curves illustrate this clearly:
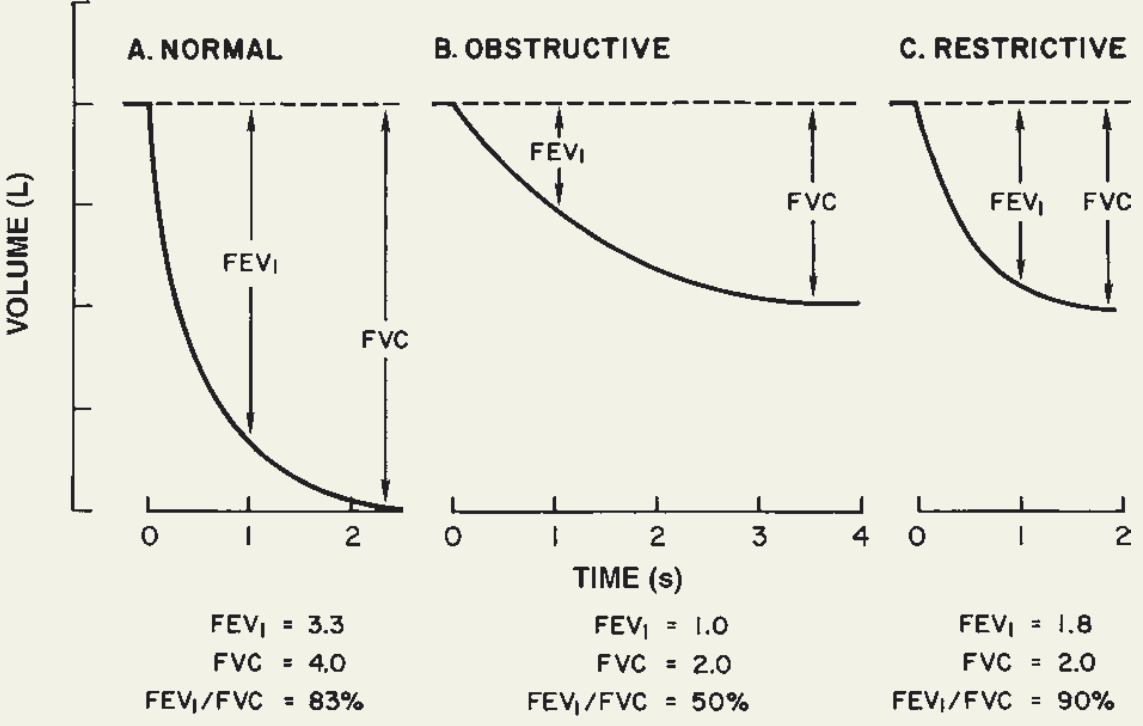
- Normal: FEV1 = 3.3 L, FVC = 4.0 L, FEV1/FVC = 83%
- Obstructive: FEV1 = 1.0 L, FVC = 2.0 L, FEV1/FVC = 50% - slow steady slope, air trapping
- Restrictive: FEV1 = 1.8 L, FVC = 2.0 L, FEV1/FVC = 90% - fast initial flow, quickly plateaus
(Ganong's Review of Medical Physiology, 26th ed.)
PART 1: COPD
Definition
COPD is characterized by persistent, progressive airflow limitation that is not fully reversible, driven by an abnormal inflammatory response of the lungs to noxious particles or gases - primarily cigarette smoke. It most commonly manifests as emphysema and/or chronic bronchitis, which frequently coexist. - Robbins & Kumar Basic Pathology
COPD is the third most common cause of death in the United States, accounting for more than $40 billion/year in direct and indirect health care costs. - Katzung's Basic and Clinical Pharmacology, 16th ed.
Risk Factors
- Cigarette smoking - the dominant risk factor (present in ~85% of cases)
- Occupational dusts and chemicals
- Alpha-1 antitrypsin (AAT) deficiency - a genetic risk factor
- Air pollution, childhood respiratory infections
- Note: COPD develops in only 15-30% of habitual smokers by traditional measures, though radiographic evidence shows important progressive changes in bronchial wall thickness and lung tissue even in smokers with normal spirometry
Pathogenesis
Emphysema
Destruction of alveolar walls distal to the terminal bronchioles through the protease-antiprotease imbalance:
- Cigarette smoke activates macrophages and recruits neutrophils
- Inflammatory cells release proteases (elastase, MMP)
- These destroy elastin in alveolar walls
- Normally, alpha-1 antitrypsin (AAT) inhibits this - but smoking also inactivates AAT
- Result: permanent enlargement of air spaces, loss of elastic recoil, air trapping
Emphysema subtypes:
- Centriacinar (centrilobular) - most common; involves the central/proximal acinus; strongly smoking-related; worse in upper lobes
- Panacinar (panlobular) - involves the entire acinus uniformly; seen in AAT deficiency; worse in lower lobes
Chronic Bronchitis
Defined clinically: persistent productive cough for at least 3 consecutive months in at least 2 consecutive years.
Pathology:
- Hyperplasia of tracheal/large airway mucous glands (Reid index >0.5)
- Goblet cell metaplasia in small airways
- Small airway inflammation (chronic bronchiolitis) - the main driver of obstruction
- Bronchiolar wall fibrosis
Bronchitic patients tend to develop hypoxemia and hypercapnia ("Blue bloaters"), in contrast to emphysematous patients who maintain near-normal oxygenation until late ("Pink puffers"). - Robbins & Kumar Basic Pathology
V/Q Mismatch in COPD
In COPD, some alveoli are perfused but poorly ventilated (low V/Q units). This mismatch dilutes oxygenated blood returning from well-ventilated areas, dropping arterial PaO2. The physiologic response is hyperventilation (driven by hypoxemia stimulating peripheral chemoreceptors), which lowers PaCO2 early in disease. - Costanzo Physiology, 7th ed.
COPD vs. Asthma Comparison
| Feature | COPD | Asthma |
|---|---|---|
| Age at onset | Older (>40 yrs, usually smokers) | Any age |
| Airflow obstruction | Fixed/irreversible | Reversible |
| Inflammation type | Neutrophilic (CD8+ T cells) | Eosinophilic (Th2, IgE-mediated) |
| ICS response | Poor (unless eosinophils high) | Excellent |
| Progression | Inexorable with smoking | Episodic, non-progressive |
GOLD Classification (Severity by Spirometry)
All require post-bronchodilator FEV1/FVC < 0.70, then graded by FEV1:
| GOLD Grade | Severity | FEV1 (% predicted) |
|---|---|---|
| I | Mild | ≥ 80% |
| II | Moderate | 50-79% |
| III | Severe | 30-49% |
| IV | Very severe | < 30%, or < 50% + PaO2 < 60 mmHg |
(GOLD 2021 Guidelines via Fishman's Pulmonary Diseases and Disorders)
The full GOLD ABCD assessment also incorporates symptom burden (CAT score or mMRC dyspnea scale) and exacerbation history, because spirometry alone does not capture functional impairment.
Clinical Features
- Progressive exertional dyspnea
- Chronic cough ± sputum production
- Barrel chest (increased AP diameter from air trapping)
- Hyperresonance on percussion
- Decreased breath sounds, prolonged expiration, wheeze
- In advanced disease: cyanosis, use of accessory muscles
- Cor pulmonale (right heart failure from chronic hypoxic pulmonary vasoconstriction) in severe/late COPD
Treatment
Bronchodilators (mainstay)
- Short-acting β2 agonists (SABA) - e.g., albuterol (salbutamol): for acute symptom relief
- Short-acting anticholinergics - e.g., ipratropium: for acute relief; can combine with SABA
- Long-acting β2 agonists (LABA) - e.g., salmeterol, formoterol: for persistent symptoms
- Long-acting muscarinic antagonists (LAMA) - e.g., tiotropium: often first choice in stable COPD
- Dual LABA + LAMA: superior to monotherapy for most patients
Inhaled Corticosteroids (ICS)
Less central than in asthma. Reserved for:
- Severe airflow obstruction (FEV1 < 50%)
- Frequent exacerbations
- High blood eosinophil count (suggests steroid responsiveness)
- Clear concurrent asthma
- Risk: increased bacterial pneumonia
Anti-inflammatory / Other
- Roflumilast (PDE4 inhibitor): reduces exacerbations in severe COPD with chronic bronchitis phenotype
- Theophylline: older agent; recent placebo-controlled trials failed to show exacerbation benefit
- Azithromycin (long-term): reduces exacerbation frequency in select patients
COPD Exacerbations
Triggered predominantly by viral and bacterial respiratory infections. Management:
- Short-acting bronchodilators (increased dose/frequency)
- Systemic corticosteroids (e.g., prednisolone 40 mg x 5 days)
- Antibiotics - routinely used (unlike asthma), as bacterial infection is frequently involved; common agents: beta-lactams, macrolides, fluoroquinolones
- Controlled oxygen (target SpO2 88-92% in hypercapnic patients)
- Non-invasive ventilation (NIV/BiPAP) for hypercapnic respiratory failure
Non-pharmacological
- Smoking cessation - the single most important intervention to slow disease progression
- Pulmonary rehabilitation
- Long-term oxygen therapy (LTOT): if PaO2 ≤ 55 mmHg (or ≤ 60 mmHg with cor pulmonale/polycythemia) - proven mortality benefit
- Lung volume reduction surgery (LVRS): for upper-lobe predominant emphysema with poor exercise tolerance
- Lung transplantation: for very severe end-stage disease
AAT Deficiency
Inherited deficiency of alpha-1 antitrypsin promotes emphysema in adulthood; smoking dramatically accelerates it. Since 1987, AAT replacement therapy (augmentation therapy) is available. - Fishman's Pulmonary Diseases and Disorders
Prognosis
Poor survival predictors include: low FEV1, hypoxemia, cor pulmonale, low BMI, resting tachycardia, poor exercise capacity, frequent exacerbations, anemia. The BODE index (BMI, Obstruction, Dyspnea, Exercise capacity) is a validated multidimensional prognostic tool. Patients unable to walk 100 m without stopping have only a 30% 5-year survival. - Fishman's Pulmonary Diseases and Disorders
PART 2: Restrictive Lung Disease
Definition
Restrictive lung disease is characterized by reduced lung volumes - specifically a reduced TLC - with a preserved or elevated FEV1/FVC ratio. The lung cannot fully inflate, either because the lung parenchyma itself is stiff/fibrotic, or because of external mechanical constraints.
Harrison's Principles of Internal Medicine (22e, 2025): "A restrictive deficit is typified by a reduced total lung capacity (TLC) and symmetrically reduced measures of FEV1 and FVC. A reduction in DLCO is also common and may precede a reduction in lung volumes."
Classification by Etiology
Intrinsic (Parenchymal / Intrapulmonary)
These are Interstitial Lung Diseases (ILD) - diffuse interstitial fibrosis from chronic alveolar injury and excessive TGF-β driven fibrogenesis.
A. Idiopathic Interstitial Pneumonias
- Idiopathic Pulmonary Fibrosis (IPF) = Usual Interstitial Pneumonia (UIP) pattern
- Most common and most severe IIP
- Patchy interstitial fibrosis, fibroblastic foci, honeycomb cysts on HRCT
- Associated with germline mutations in telomerase; genetic variants in mucin (MUC5B) and surfactant genes
- Affects adults >50 years; ~132,000 Americans currently affected
- Median survival ~3-5 years without treatment
- Mechanism: repeated alveolar epithelial injury → ER stress, apoptosis, epithelial-mesenchymal transition → fibroblast activation → irreversible fibrosis
- Robbins & Kumar Basic Pathology; Ganong's Review
B. Pneumoconioses (occupation-related)
- Pathogenesis: inhaled particles phagocytosed by alveolar macrophages → inflammasome activation → fibrogenic cytokine release
- Coal workers' pneumoconiosis: ranges from simple (anthracosis) to Progressive Massive Fibrosis (PMF)
- Silicosis: most common pneumoconiosis worldwide; crystalline silica (quartz); risk of TB and lung cancer
- Asbestosis: interstitial fibrosis; also linked to pleural plaques, pleural effusions, lung cancer (synergistic with smoking), and malignant mesothelioma
C. Granulomatous ILD
- Sarcoidosis: multisystem disease of unknown etiology; non-necrotizing (non-caseating) granulomas; CD4+ Th1 driven
- Lung involvement in ~90% of cases
- Other features: bilateral hilar lymphadenopathy, erythema nodosum, uveitis, hypercalcemia
- Can progress from granulomatous to diffuse interstitial fibrosis
- Hypersensitivity Pneumonitis (HP): immune-mediated response to organic antigens (farmer's lung, bird fancier's lung)
D. ILD associated with systemic disease
- Connective tissue diseases: RA, SLE, systemic sclerosis (most common CTD-ILD), Sjogren's, polymyositis/dermatomyositis
- Drug-induced: amiodarone, bleomycin, methotrexate, nitrofurantoin
Extrinsic (Extra-pulmonary)
The lung itself may be normal, but restricted from the outside:
| Cause | Mechanism |
|---|---|
| Obesity | Diaphragm elevation, chest wall loading |
| Kyphoscoliosis | Deformed chest wall, mechanical disadvantage |
| Neuromuscular disease | Respiratory muscle weakness (ALS, muscular dystrophy, phrenic nerve palsy, myasthenia gravis) |
| Pleural disease | Massive pleural effusion, fibrothorax |
| Ankylosing spondylitis | Rigid chest wall |
| Post-surgical | Pneumonectomy, resection |
Pathophysiology
- Decreased lung compliance - stiff lungs resist inflation; more work to breathe
- All lung volumes reduced: TLC ↓, FRC ↓, RV ↓
- FEV1 and FVC both fall proportionally, preserving the ratio
- Diffusion impairment (reduced DLCO) develops as alveolar surface area is destroyed
- Hypoxemia via V/Q mismatch and diffusion limitation
- In advanced disease: pulmonary hypertension and cor pulmonale (as in COPD)
- Decreased compliance vs. increased resistance: restrictive = stiff lungs (compliance problem); obstructive = airway narrowing (resistance problem)
Clinical Features
- Progressive exertional dyspnea (hallmark)
- Dry, non-productive cough (in ILD)
- Fine, "velcro" (bibasilar) crackles on auscultation (IPF)
- Clubbing of fingers (especially IPF)
- Cyanosis and right heart failure in advanced stages
- Symptoms/signs of underlying cause (e.g., skin rash in dermatomyositis, arthritis in RA)
Investigations
Pulmonary Function Tests
- FVC ↓, FEV1 ↓, FEV1/FVC normal or ↑, TLC ↓ (confirmatory of restriction), DLCO ↓
- A low FVC with a normal FEV1/FVC should prompt TLC measurement to confirm restriction vs. a non-specific pattern
Imaging
- CXR: basilar reticular pattern (IPF), bilateral hilar lymphadenopathy (sarcoidosis), upper lobe opacities (silicosis)
- HRCT (standard of care for ILD evaluation):
- IPF: basal, peripheral honeycombing ± traction bronchiectasis (UIP pattern)
- HRCT can be diagnostic for IPF in the right clinical context, avoiding the need for lung biopsy
Bronchoscopy (BAL + biopsy)
- BAL: eosinophilia >25% suggests chronic eosinophilic pneumonia; lymphocytosis suggests HP or sarcoidosis
- Transbronchial biopsy: good for sarcoidosis (granulomas); limited for most IIPs
- Cryobiopsy: emerging technique with larger yield
Surgical Lung Biopsy (VATS)
- Gold standard for IIP diagnosis when HRCT is non-diagnostic
- Short-term mortality risk ~5%; higher in IPF patients
- Should ideally be obtained before starting treatment
Treatment
IPF (Intrinsic/Fibrotic ILD)
- Antifibrotic agents (slow progression, do not reverse fibrosis):
- Pirfenidone: anti-fibrotic, anti-inflammatory, antioxidant
- Nintedanib: tyrosine kinase inhibitor; targets PDGFR, VEGFR, FGFR pathways
- Lung transplantation: definitive for eligible patients; 5-year survival ~50%
- Supplemental oxygen, pulmonary rehabilitation, smoking cessation
Sarcoidosis
- Many cases spontaneously remit; treatment for symptomatic/progressive disease
- Oral corticosteroids remain the mainstay
- Steroid-sparing agents: methotrexate, azathioprine
Pneumoconioses
- No curative treatment; remove from exposure
- Supportive management; treat complications (TB in silicosis)
Extrinsic Restriction
- Treat the underlying cause (weight loss, orthotic devices, respiratory support in NMD)
Summary Comparison Table
| Feature | COPD | Restrictive |
|---|---|---|
| Core defect | Airflow obstruction (airways) | Reduced lung volumes (parenchyma/chest wall) |
| FEV1/FVC | < 0.70 (reduced) | Normal or elevated (>80%) |
| TLC | Normal or elevated | Reduced (diagnostic) |
| Residual volume | Elevated (air trapping) | Reduced or normal |
| DLCO | Reduced (emphysema) | Reduced (ILD) |
| Main causes | Smoking, AAT deficiency | IPF, sarcoidosis, pneumoconioses, CTD, obesity, NMD |
| Reversibility | Partial at best | Usually irreversible (fibrotic) |
| Airway resistance | Increased | Normal (unless mixed pattern) |
| Compliance | Increased (emphysema) | Decreased |
| Cor pulmonale | In severe/late disease | In severe/late disease |
| Treatment | Bronchodilators, ICS, smoking cessation, O2 | Antifibrotics (IPF), steroids (sarcoidosis), lung Tx |
Sources:
- Robbins & Kumar Basic Pathology - COPD and ILD pathology, emphysema subtypes, sarcoidosis, pneumoconioses
- Ganong's Review of Medical Physiology, 26th ed. - PFT spirometry diagram, airflow mechanics, IPF
- Katzung's Basic and Clinical Pharmacology, 16th ed. - COPD pharmacotherapy, exacerbation management
- Fishman's Pulmonary Diseases and Disorders - GOLD classification, BODE index, AAT deficiency
- Harrison's Principles of Internal Medicine, 22e (2025) - Restrictive PFT interpretation, HRCT, biopsy
- Costanzo Physiology, 7th ed. - COPD physiology case, V/Q mismatch, A-a gradient
This is a shared conversation. Sign in to Orris to start your own chat.