Organize well answer for university exam high yeild 10 marks long answer As m pharm student write Easy language ma hooi but also maintain formal language.. easy to understand and write in exam Classify immunosuppressant drugs and explain their mechanism of action, therapeutic uses, and adverse effects. Discuss pharmacology of immunosuppressants used in organ transplantation and autoimmune diseases.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed. Let me write the complete, high-yield exam answer.
IMMUNOSUPPRESSANT DRUGS
Classification, Mechanism of Action, Therapeutic Uses, and Adverse Effects
(M.Pharm / University Exam - 10 Marks Long Answer)
INTRODUCTION
Immunosuppressant drugs are agents that suppress or reduce the activity of the immune system. They are used primarily in two situations:
- Organ transplantation - to prevent graft rejection
- Autoimmune diseases - to control abnormal immune responses
The immune response depends on T-cell activation, which occurs in three sequential signals - and most immunosuppressants target one of these signals.
CLASSIFICATION OF IMMUNOSUPPRESSANT DRUGS
Immunosuppressants are classified based on their role in therapy (for transplantation) and their mechanism of action.
Classification by Role in Transplant Therapy:
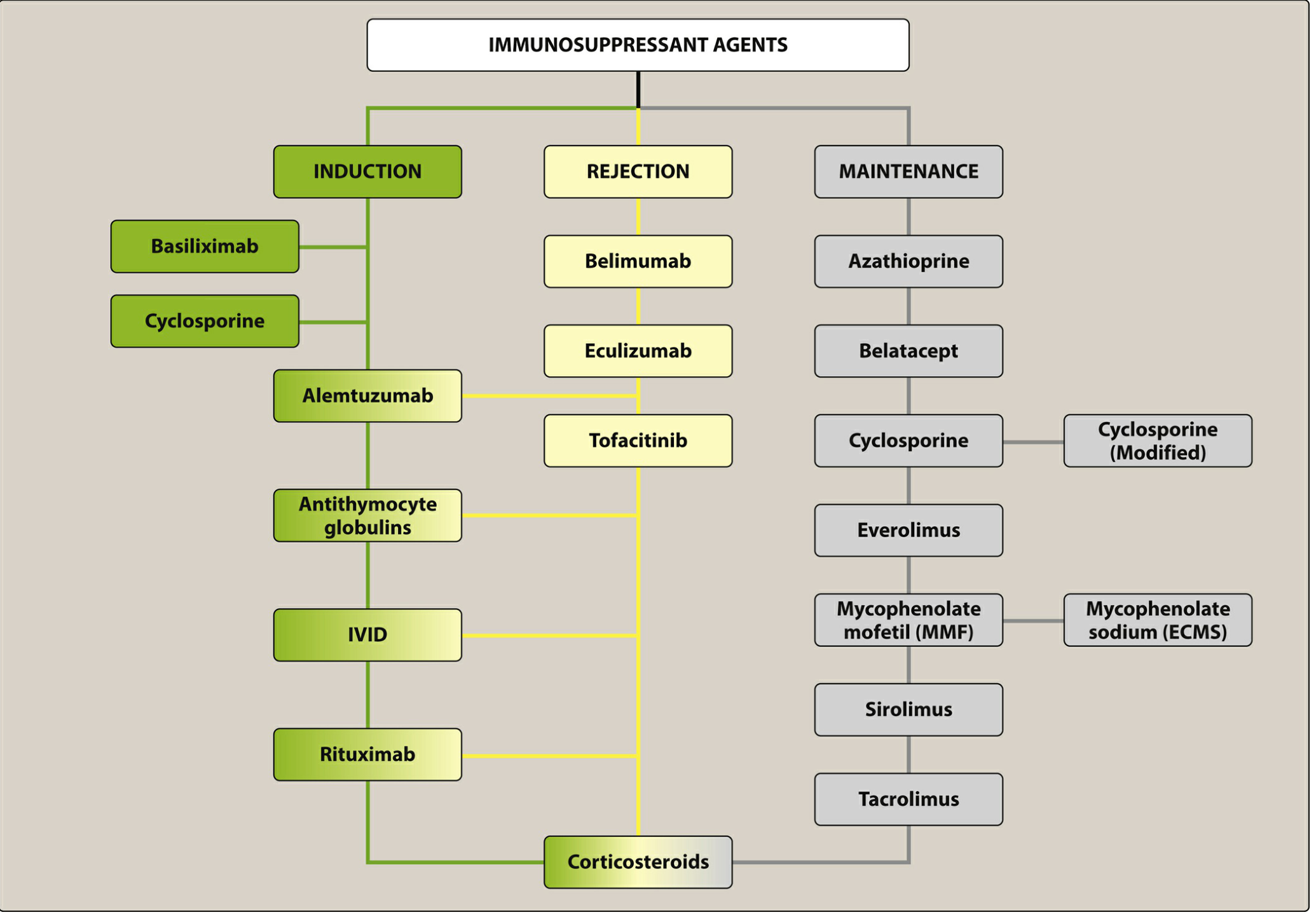
| Role | Drugs |
|---|---|
| Induction | Basiliximab, Cyclosporine, Alemtuzumab, Antithymocyte globulins, IVIG, Rituximab, Corticosteroids |
| Rejection Treatment | Methylprednisolone, Bortezomib, Rituximab, Belimumab, Eculizumab, Tofacitinib |
| Maintenance | Azathioprine, Mycophenolate mofetil (MMF), Cyclosporine, Tacrolimus, Sirolimus, Everolimus, Belatacept, Corticosteroids |
Classification by Mechanism of Action:
| Class | Examples |
|---|---|
| 1. Calcineurin Inhibitors (CNIs) | Cyclosporine, Tacrolimus, Voclosporin |
| 2. mTOR Inhibitors | Sirolimus (Rapamycin), Everolimus |
| 3. Antiproliferatives (Antimetabolites) | Azathioprine, Mycophenolate mofetil |
| 4. Corticosteroids | Prednisolone, Methylprednisolone |
| 5. Biological Agents - Monoclonal Antibodies | Basiliximab, Alemtuzumab, Rituximab, Belatacept, Belimumab |
| 6. Polyclonal Antibodies | Antithymocyte globulin (ATG) |
| 7. Proteasome Inhibitors | Bortezomib |
| 8. JAK Inhibitors | Tofacitinib |
MECHANISM OF ACTION (Detailed)
The overall mechanism of all major immunosuppressants is shown in this diagram:
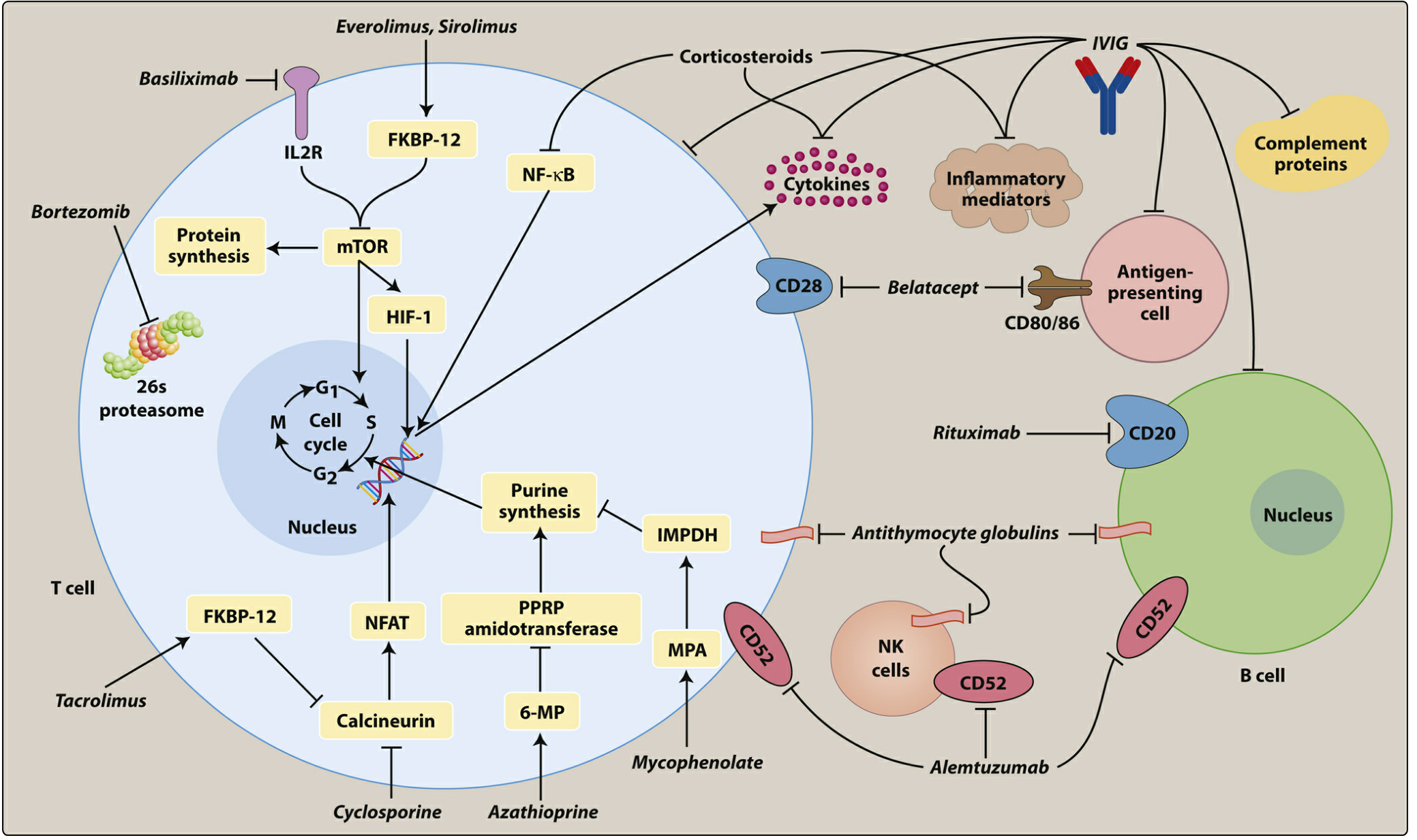
1. CALCINEURIN INHIBITORS (CNIs)
Drugs: Cyclosporine, Tacrolimus, Voclosporin
Mechanism:
- T-cell activation requires calcineurin (a phosphatase enzyme) to activate NFAT (Nuclear Factor of Activated T-cells), which promotes IL-2 gene transcription.
- Cyclosporine binds to Cyclophilin-1 (an intracellular receptor).
- Tacrolimus binds to FKBP-12 (FK-binding protein).
- Both drug-receptor complexes inhibit calcineurin.
- Result: Inhibition of IL-2, IL-3, IL-4, TNF-α, and IFN-γ transcription → T-cell activation is blocked.
- Tacrolimus is 10-100x more potent than cyclosporine.
Therapeutic Uses:
- Prevention of solid organ rejection (kidney, liver, heart, lung transplants)
- Treatment of rheumatoid arthritis, psoriasis, SLE
- Voclosporin: specifically approved for SLE nephritis
Adverse Effects:
- Nephrotoxicity (major, dose-limiting) - most important!
- Hypertension, headache, tremor
- Cyclosporine specific: Hirsutism (excessive hair growth), gingival hyperplasia, hyperlipidemia
- Tacrolimus specific: Diabetes mellitus (new-onset), alopecia, neurotoxicity
- Both: Infections, CYP3A4 drug interactions, narrow therapeutic index (requires TDM)
Note for exams: Both CNIs are metabolized by CYP3A4 - so numerous drug interactions occur. Grapefruit juice increases cyclosporine bioavailability by 62%.
2. mTOR INHIBITORS
Drugs: Sirolimus (Rapamycin), Everolimus
Mechanism:
- After IL-2 binds to its receptor (Signal 3), it activates the mTOR pathway.
- Sirolimus and everolimus bind to FKBP-12 → the complex then inhibits mTOR (mammalian target of rapamycin).
- mTOR inhibition blocks the cell cycle (G1 → S transition), preventing T-cell proliferation.
- Note: Unlike CNIs, they do NOT inhibit calcineurin or IL-2 production - they block the cell's response to IL-2.
Therapeutic Uses:
- Rejection prophylaxis for organ transplantation (kidney, heart)
- Prevention and treatment of graft-versus-host disease (GVHD) - Sirolimus
- Sirolimus-coated coronary stents - prevent restenosis
- Everolimus: also used in oncology (renal cell carcinoma, breast cancer, neuroendocrine tumors)
- Commonly used to reduce CNI dose and minimize nephrotoxicity
Adverse Effects:
- Metabolic: Hypercholesterolemia, hypertriglyceridemia
- Hematologic: Leukopenia, thrombocytopenia, anemia
- GI: Nausea, vomiting, diarrhea
- New-onset diabetes mellitus (long-term use)
- Poor wound healing (avoid in perioperative period)
- Mouth ulcers (aphthous stomatitis)
- Substrate of CYP3A4 - multiple drug interactions; TDM required
3. ANTIPROLIFERATIVES (ANTIMETABOLITES)
Drugs: Azathioprine, Mycophenolate mofetil (MMF)
A. Azathioprine
- A prodrug converted to 6-mercaptopurine (6-MP), then to thioinosinic acid (nucleotide analogue).
- This analogue is incorporated into DNA chains and blocks DNA elongation - preventing lymphocyte proliferation.
- Important interaction: Xanthine oxidase inhibitors (allopurinol, febuxostat) inhibit azathioprine metabolism → increased toxicity. Concomitant use with febuxostat is contraindicated.
- Adverse effects: Bone marrow suppression (dose-limiting), hepatotoxicity, GI disturbances, increased risk of infections and malignancy.
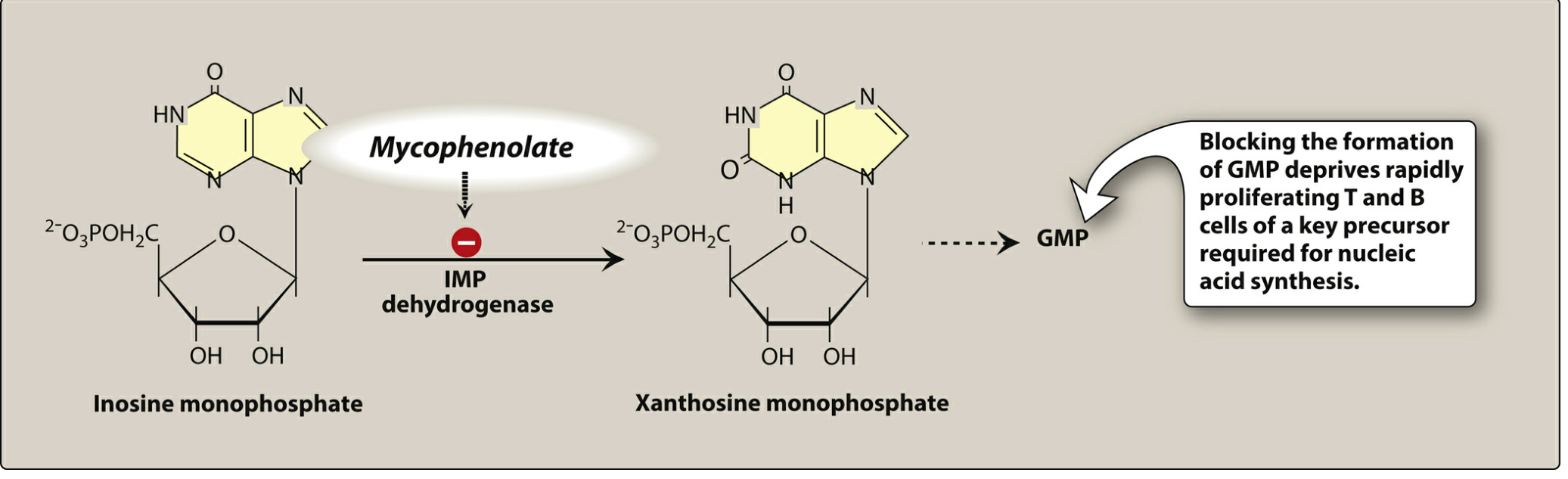
B. Mycophenolate Mofetil (MMF)
- MMF is a prodrug converted to Mycophenolic acid (MPA) in the liver.
- MPA is a potent, reversible, noncompetitive inhibitor of inosine monophosphate dehydrogenase (IMPDH).
- This blocks the de novo synthesis of guanosine monophosphate (GMP).
- Lymphocytes (T and B cells) rely entirely on de novo synthesis and cannot use the salvage pathway - making them selectively sensitive.
- Result: Selective T and B cell proliferation is blocked.
- MMF has largely replaced azathioprine due to better efficacy and safety profile.
- EC-MPA (enteric-coated, mycophenolate sodium) reduces GI side effects.
- Adverse effects: Leukopenia, thrombocytopenia, GI distress (nausea, vomiting, diarrhea), opportunistic infections.
4. CORTICOSTEROIDS
Drugs: Prednisone, Prednisolone, Methylprednisolone
Mechanism:
- First pharmacologic agents used as immunosuppressives.
- Enter cells and bind to the glucocorticoid receptor → complex enters nucleus → regulates DNA transcription.
- Result: Nonspecific inhibition of interleukins and TNF-α. Rapidly reduce lymphocyte populations by lysis or redistribution.
- T-lymphocytes are most affected.
- Methylprednisolone is used for transplant induction and rejection episodes; Prednisone/prednisolone for autoimmune conditions.
Therapeutic Uses:
- Solid organ transplant (induction, maintenance, acute rejection)
- Chronic GVHD
- Autoimmune diseases: Rheumatoid arthritis, SLE, temporal arteritis, asthma, inflammatory bowel disease, multiple sclerosis
Adverse Effects (Dose-Dependent):
- Short-term: Hyperglycemia, hypertension, edema, mood swings/insomnia, increased infections
- Long-term: Osteoporosis, myopathy, cataracts, impaired wound healing, Cushingoid appearance, adrenal suppression, peptic ulcer
5. BIOLOGICAL AGENTS - MONOCLONAL ANTIBODIES
A. Basiliximab (IL-2 Receptor Antagonist)
- Chimeric monoclonal antibody targeting CD25 (IL-2 receptor α chain) on activated T-cells.
- Blocks IL-2 from binding → prevents T-cell activation and proliferation (non-depleting).
- Used for induction in kidney transplantation.
- Well tolerated; minimal adverse effects compared to other biologics.
B. Alemtuzumab
- Humanized monoclonal antibody targeting CD52 on T and B lymphocytes.
- Causes profound and prolonged T and B cell depletion.
- Used for induction and rejection therapy.
- Adverse effects: Infusion reactions, severe leukopenia, neutropenia, thrombocytopenia, CMV and viral infections.
C. Rituximab
- Chimeric monoclonal antibody targeting CD20 on B lymphocytes.
- Mediates B cell lysis and depletion via CDC (complement-dependent cytotoxicity) and ADCC.
- Used for induction, antibody-mediated rejection (AMR), and autoimmune conditions (RA, lupus).
- Adverse effects: Infusion reactions, leukopenia, risk of PML (progressive multifocal leukoencephalopathy).
D. Belatacept (Costimulation Blocker)
- Recombinant fusion protein of CTLA-4.
- Binds to CD80/CD86 on antigen-presenting cells → blocks CD28 from binding → inhibits Signal 2 of T-cell activation.
- Approved for kidney transplant as CNI substitute to avoid nephrotoxicity.
- Risk of PTLD (post-transplant lymphoproliferative disorder), especially CNS. Contraindicated in EBV-seronegative patients.
E. Belimumab
- Fully human monoclonal antibody against BLyS (B lymphocyte stimulator protein).
- Blocks B-cell survival and differentiation into immunoglobulin-secreting plasma cells.
- Approved for systemic lupus erythematosus (SLE).
- Available as SC or IV formulation.
- Warnings: serious infections, PML, depression/suicidality.
6. POLYCLONAL ANTIBODIES - ANTITHYMOCYTE GLOBULIN (ATG)
- Prepared by immunizing horses or rabbits with human thymocytes.
- Contains multiple antibodies → causes T-cell depletion by complement-mediated lysis.
- Used for transplant induction and treatment of acute rejection.
- Adverse effects: Infusion reactions (fever, chills), leukopenia, thrombocytopenia, pulmonary edema, CMV infections.
7. BORTEZOMIB (Proteasome Inhibitor)
- Inhibits the 26S proteasome → leads to plasma cell depletion.
- Used in the treatment of antibody-mediated rejection (AMR).
- Adverse effects: Leukopenia, anemia, thrombocytopenia, peripheral neuropathy, nausea/vomiting, hepatotoxicity.
PHARMACOLOGY IN ORGAN TRANSPLANTATION - TRIPLE THERAPY
The standard immunosuppression protocol in transplantation is Triple Therapy:
| Phase | Drugs Used |
|---|---|
| Induction (0-2 weeks) | ATG or Basiliximab + high-dose corticosteroids ± CNI |
| Maintenance (long-term) | CNI (cyclosporine or tacrolimus) + MMF + low-dose corticosteroids |
| Acute Rejection Treatment | High-dose methylprednisolone (pulse) ± ATG |
| Antibody-Mediated Rejection | IVIG + Rituximab ± Bortezomib |
Why Triple Therapy?
- Each drug targets a different step in the immune cascade → synergistic immunosuppression.
- Allows dose reduction of each drug → fewer adverse effects.
- Notably, CNI dose is often reduced to spare nephrotoxicity.
PHARMACOLOGY IN AUTOIMMUNE DISEASES
| Disease | First Choice | Alternatives |
|---|---|---|
| Rheumatoid Arthritis | Methotrexate | Cyclosporine, Tacrolimus, Azathioprine |
| SLE | Hydroxychloroquine + Corticosteroids | Azathioprine, MMF (for nephritis), Belimumab, Voclosporin |
| Inflammatory Bowel Disease | Azathioprine | MMF, Cyclosporine (refractory) |
| Psoriasis | Cyclosporine | Methotrexate, Tacrolimus (topical) |
| Multiple Sclerosis | Corticosteroids (acute) | Alemtuzumab |
| Polymyositis/Dermatomyositis | Corticosteroids | Cyclosporine, Tacrolimus |
ADVERSE EFFECTS SUMMARY TABLE
| Drug | Major Adverse Effect | Unique Effect |
|---|---|---|
| Cyclosporine | Nephrotoxicity | Hirsutism, gingival hyperplasia |
| Tacrolimus | Nephrotoxicity | New-onset diabetes, alopecia |
| Sirolimus | Hyperlipidemia | Poor wound healing, mouth ulcers |
| Azathioprine | Bone marrow suppression | Interaction with allopurinol |
| MMF | GI distress | Leukopenia |
| Corticosteroids | Osteoporosis (long-term) | Cushingoid features |
| Basiliximab | Well tolerated | - |
| Alemtuzumab | Severe leukopenia | CMV infections |
| Rituximab | Infusion reaction | PML |
| Belatacept | PTLD | Contraindicated in EBV-negative patients |
THERAPEUTIC DRUG MONITORING (TDM)
The following drugs have a narrow therapeutic index and require TDM:
- Cyclosporine
- Tacrolimus
- Sirolimus
- Everolimus
TDM ensures simultaneous maximization of immunosuppression and minimization of toxicity.
KEY POINTS FOR EXAM (Memory Tips)
| Mnemonic | Meaning |
|---|---|
| CNI = CAN NOT Inhibit (T-cell IL-2 production) | Cyclosporine/Tacrolimus block calcineurin → no IL-2 |
| mTOR = Stops T-cell from Proliferating | Sirolimus blocks G1→S transition |
| MMF = Must Monitor For (GI effects) | MMF blocks IMPDH → no GMP → no lymphocyte DNA |
| ATG = All T-cells Gone | Polyclonal antibody depletes T-cells |
| Triple Therapy = CNI + MMF + Steroid | Standard maintenance regimen |
CONCLUSION
Immunosuppressant drugs are broadly classified into calcineurin inhibitors, mTOR inhibitors, antiproliferatives, corticosteroids, and biological agents. Each class targets a specific step in T-cell or B-cell activation. The cornerstone of transplant immunosuppression is triple therapy (CNI + MMF + steroid), while autoimmune diseases are managed with individualized regimens depending on disease severity. The major clinical concerns are nephrotoxicity (CNIs), bone marrow suppression (azathioprine), metabolic effects (steroids/mTOR inhibitors), and increased susceptibility to infections and malignancies in all patients receiving long-term immunosuppression.
Sources: Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th ed.; Goodman & Gilman's The Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.