Bk amputation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"transtibial amputation" OR "below-knee amputation"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full structured answer:
Below-Knee (Transtibial) Amputation
Definition & Overview
A below-knee amputation (BKA), formally termed transtibial amputation, is surgical removal of the lower limb at a level between the knee joint and the ankle. It preserves the knee joint, which is the single most important factor in functional rehabilitation - patients with an intact knee consume far less energy ambulating with a prosthesis than those with above-knee (transfemoral) amputation.
Indications
The leading causes are complications of diabetes mellitus and peripheral arterial disease (together accounting for the majority of cases). Other indications include:
- Severe trauma or crush injury
- Malignancy (soft tissue or bone sarcoma)
- Severe infection / necrotizing fasciitis / gas gangrene
- Congenital limb deficiency
- Chronic non-healing wounds unresponsive to revascularization
Guillotine (open) amputation is reserved for emergency situations - rapidly spreading infection, gas gangrene - where the goal is rapid life-saving debridement; formal closure follows days later once infection is controlled.
Choosing BKA vs. AKA
| Factor | Favors BKA | Favors AKA |
|---|---|---|
| Circulation | Adequate perfusion at BKA level | Ischemia extends too proximally |
| Knee function | Intact, functional knee | Fixed flexion contracture |
| Infection / gangrene | Confined below knee | Spreads above proposed BKA level |
| Stump length | At least 8.8 cm of tibia preservable | Inadequate residual tibia |
| Functional goals | Patient ambulatory candidate | Non-ambulatory, high comorbidities |
A short BKA (even to the level of the tibial tuberosity) is functionally superior to an AKA. Minimum usable tibial length is approximately 8.8 cm; below this the fibula should be entirely removed to allow the short stump to fit a prosthetic socket.
Level of Amputation
- Ideal tibial length: 12.5 to 17.5 cm from the medial knee joint line (rule of thumb: 2.5 cm per 30 cm of body height)
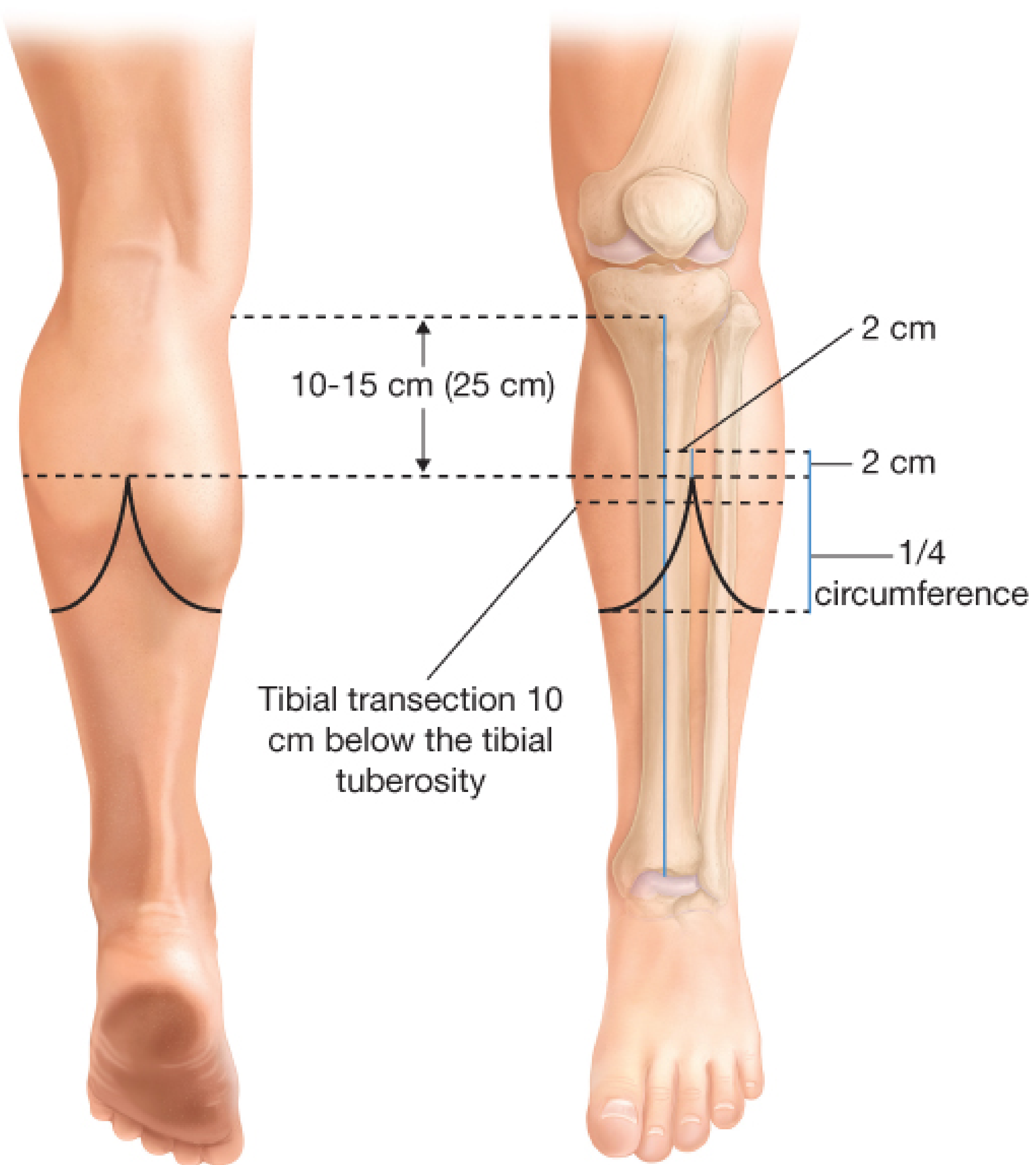
- Standard level: tibia transected ~10 cm below the tibial tuberosity
- Fibula: cut 1-2 cm shorter than the tibia
- Distal third of the leg is suboptimal - poor vascularity, slower healing, limited soft tissue
- In ischemic limbs, amputation is customarily at a higher level (10-12.5 cm distal to the joint line)
Surgical Techniques
1. Long Posterior Flap (Burgess Technique) - Most Common
This is the preferred technique, especially in vascular disease, because the gastrocnemius and soleus are supplied by sural arteries arising proximal to the knee - making the posterior flap reliable even with distal arterial occlusion.
Skin marking:
- Anterior incision: 1 cm distal to the proposed tibial transection level, with a length equal to two-thirds of the leg circumference at that level
- Medial and lateral longitudinal limbs: each one-third of the circumference (~9-12 cm)
- The posterior flap must be generous - excess is trimmed at closure
Key steps:
- Anterior compartment muscles divided at skin incision level
- Anterior tibial neurovascular bundle - identified and suture-ligated
- Tibia cleared of periosteum; transected with oscillating/Gigli saw; anterior cortex beveled at 45° to prevent pressure necrosis
- Fibula cleared and transected 2 cm proximal to tibial cut
- Posterior tibial and peroneal neurovascular bundles - suture-ligated
- Nerves (posterior tibial, common peroneal, deep peroneal, sural) - gently retracted distally, sharply divided, allowed to retract proximally to prevent neuroma formation
- Posterior flap rotated anteriorly; muscle debulked as needed
- Deep posterior musculature secured over tibial end (myodesis to periosteum)
- Gastrocnemius fascia approximated to anterior fascia - absorbable suture
- Skin closed with interrupted nylon or staples
2. Skew Flap (Robinson/Jain Technique)
Used when posterior flap viability is questionable:
- A fishmouth incision is made at 10-25 cm below the joint line (2-2.5 cm lateral to tibial crest as the flap junction point)
- Creates anterolateral and posteromedial flaps of equal quarter-circumference length
- The posterior gastrocnemius-soleus complex is brought anteriorly and secured to anterior periosteum
- The suture line lies off the tibial crest - reducing pressure from prosthetic socket
3. Equal Anterior and Posterior Flaps (Classic)
Used when gangrene or wounds preclude posterior flap; each flap length = one-half the anteroposterior diameter of the leg.
4. Ertl (Osteomyoplastic) Amputation
- A bone bridge is created between tibia and fibula using a fibular autograft strut
- Notches cut in both bones; strut secured with heavy sutures
- Advantages: more stable end-bearing construct, decreased tibiofibular joint instability, better load transfer
Ischemic limb modifications:
- Tourniquet traditionally avoided (though recent RCTs show it may be safe)
- Tension myodesis and osteomyoplasty contraindicated in ischemic limbs - compresses remaining blood supply
- Skew or posterior flaps favored over anterior flaps
Neurovascular Management
| Structure | Action |
|---|---|
| Anterior tibial vessels | Suture-ligate proximal to bone cut |
| Posterior tibial vessels | Suture-ligate |
| Peroneal vessels | Suture-ligate |
| Posterior tibial nerve | Retract distally under tension → divide sharply → allow to retract proximally |
| Common peroneal nerve | Identified deep to peroneus longus; divided proximal to where superficial peroneal branches |
| Deep peroneal nerve | Divided with anterior compartment muscles |
| Sural nerve | Divided in posterior subcutaneous plane |
| Great/lesser saphenous veins | Ligated during skin incision |
Nerves are handled with gentle traction + sharp division + proximal retraction - this minimizes painful neuroma formation.
Postoperative Management
- Rigid dressing or posterior splint - prevents knee flexion contracture (major complication)
- Closed-suction drain - optional, at surgeon's discretion to prevent hematoma
- Skin closure kept for at least 3 weeks until healed
- Stump shrinker applied after wound healing to shape residual limb for prosthetic fitting
- Early prosthetic fitting: 5 to 21 days postoperatively if residual limb can transfer load and patient has adequate physiologic reserve
- Formal inpatient rehabilitation is brief; most prosthetic training is outpatient
Rehabilitation
- Requires functional quadriceps - stumps lacking quadriceps function are not useful for prosthetic ambulation
- Physiatrist + physical therapist guide progression: rigid dressing → temporary prosthesis → permanent prosthesis (process takes several months)
- Endoskeletal (pylon) prosthetic designs preferred - easier to modify
- Goals: return to prior occupation, hobbies, education (with social work + vocational counseling support)
- Rehabilitation in nonischemic limbs is far more aggressive and successful due to younger, healthier population
Complications
| Complication | Details |
|---|---|
| Wound breakdown / infection | Most common local complications; can lead to conversion to AKA |
| Knee flexion contracture | Prevented by posterior splint; if established, makes prosthetic use impossible |
| Neuroma | Painful; prevented by proper nerve handling |
| Phantom limb pain | Requires multimodal pain management |
| Residual limb edema | Managed with stump shrinker, compressive wrapping |
| Hematoma | Consider closed drain; risk of infection and wound dehiscence |
| Tibiofibular joint instability | Addressed by Ertl procedure or retention of fibular head |
| Prosthetic socket skin breakdown | Higher risk in elderly with newer longer-stump prosthetic components |
Key Points Summary
- BKA preserves the knee joint and dramatically reduces the energy cost of ambulation compared to AKA
- The long posterior flap (Burgess) is the standard technique for vascular patients
- Ideal tibial length: 12.5-17.5 cm; minimum functional length ~8.8 cm
- Fibula cut 2 cm proximal to tibia; anterior tibial cortex beveled at 45°
- All nerves divided under traction and allowed to retract - prevents neuroma
- Tension myodesis is contraindicated in ischemic limbs
- Knee flexion contracture and wound breakdown are the two major preventable complications
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, p. 879-881; Fischer's Mastery of Surgery 8th Ed, p. 6635-6660; Mulholland and Greenfield's Surgery 7th Ed, p. 5001-5003; Miller's Review of Orthopaedics 9th Ed; Current Surgical Therapy 14th Ed
This is a shared conversation. Sign in to Orris to start your own chat.