Acute and chronic smoker
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Difference between a and c smoker in terms of duration packet etc
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough answer. Here is the complete comparison:
Acute vs. Chronic Smoker - Key Differences
Definition by Duration & Pack History
| Feature | Acute Smoker | Chronic Smoker |
|---|---|---|
| Duration of smoking | Recent/new onset (days to weeks to a few months) | Long-term, years to decades |
| Pack-year history | Low (< a few pack-years) | Heavy - typically ≥ 20 pack-years (often 40+ pack-years for COPD/bronchitis) |
| Pack-year formula | Packs per day × years smoked | Same formula, but accumulated over long periods |
A "pack-year" = smoking 1 pack (20 cigarettes) per day for 1 year. So 2 packs/day × 20 years = 40 pack-years.
Pathological Changes: Progression from Acute to Chronic
This is the core concept in pathology - smoking causes a stepwise progression of epithelial injury:
Acute Smoker - Early/Mild Changes
These are the earliest changes seen in smoking-damaged respiratory epithelium:
- Goblet cell hyperplasia - increase in mucus-secreting cells
- Basal (reserve) cell hyperplasia - proliferation of the regenerative layer
- Squamous metaplasia - normal ciliated pseudostratified epithelium replaced by squamous epithelium
These changes are potentially reversible if the person stops smoking early.
Chronic Smoker - Progressive/Severe Changes
With continued, long-term exposure:
4. Squamous dysplasia - disordered squamous epithelium, loss of nuclear polarity, nuclear hyperchromasia, pleomorphism, mitotic figures
5. Carcinoma in situ (CIS) - full thickness atypia, basement membrane still intact
6. Invasive squamous cell carcinoma - basement membrane disrupted, stromal invasion
These are illustrated in the Robbins histology image below:
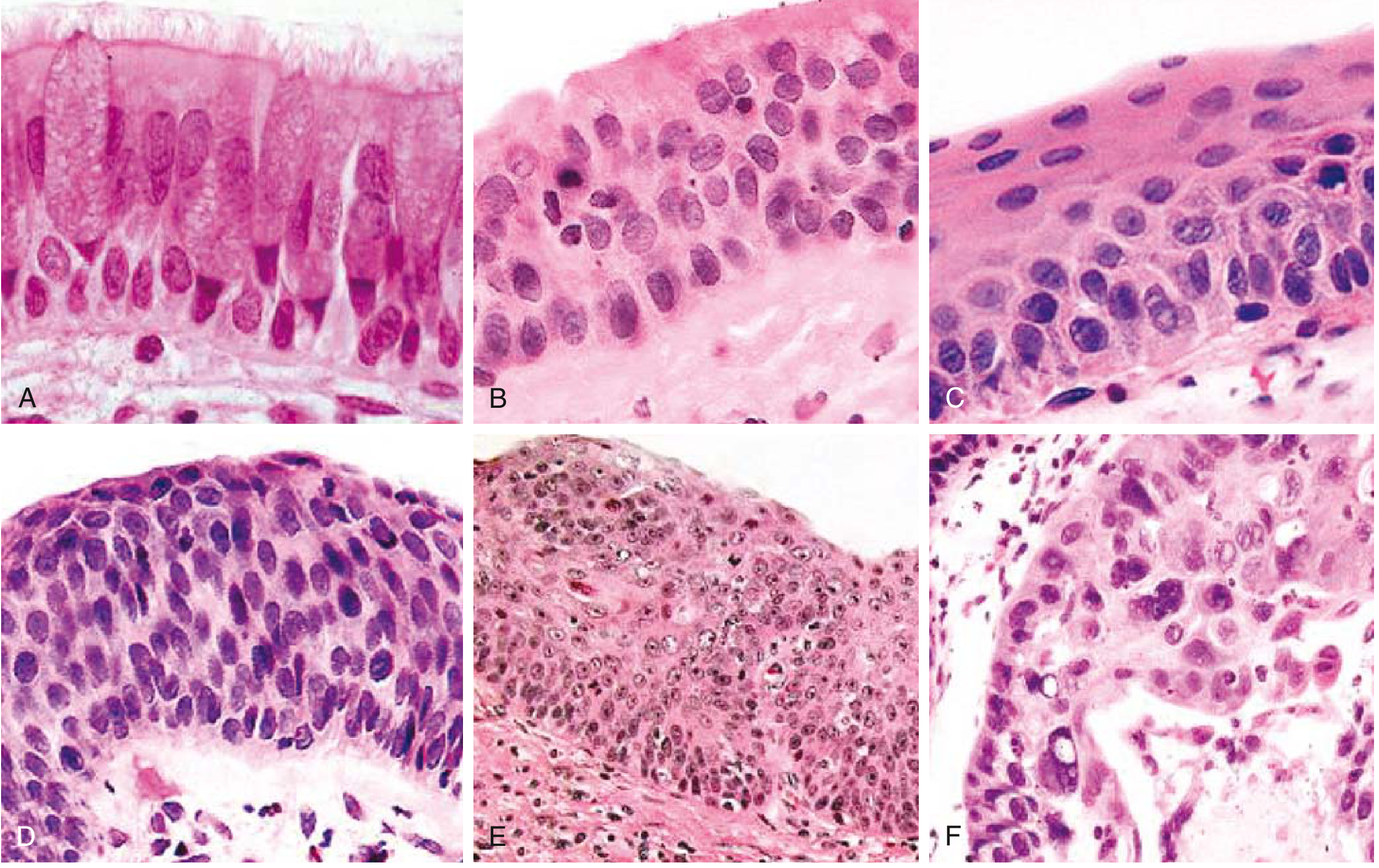
A-C = acute/early smoker changes; D-F = chronic/late smoker changes - Robbins & Kumar Basic Pathology
Specific Conditions Associated with Each
Acute Smoker
- Acute eosinophilic pneumonia - a subset is directly linked to recent onset of smoking (within weeks of starting)
- Ciliary dysfunction and impaired mucus clearance begin almost immediately
Chronic Smoker (≥ 20-40 pack-years)
- Chronic bronchitis - defined clinically as productive cough for ≥ 3 months in ≥ 2 consecutive years; histologically: enlarged mucous glands, Reid index > 0.4, goblet cell metaplasia, mucus plugging
- Emphysema - destruction of alveolar walls (centriacinar type, upper lobe dominant)
- COPD - FEV1/FVC < 0.7; most affected patients have ≥ 40 pack-year history
- Smoking-related ILDs - Respiratory bronchiolitis-ILD (RB-ILD), Desquamative Interstitial Pneumonia (DIP), Pulmonary Langerhans Cell Histiocytosis (PLCH)
- Lung cancer - squamous cell carcinoma and small cell carcinoma most tightly linked; screening recommended at ≥ 50 years old with ≥ 20 pack-year history
- Acquired CFTR dysfunction - leads to abnormal dehydrated mucus, worsening chronic bronchitis
Summary Table
| Parameter | Acute Smoker | Chronic Smoker |
|---|---|---|
| Duration | Days - months | Years - decades |
| Pack-years | < 5 | ≥ 20 (COPD/cancer risk threshold) |
| Epithelial change | Goblet hyperplasia, basal cell hyperplasia, squamous metaplasia | Dysplasia → CIS → carcinoma |
| Reversibility | Yes (if cessation is early) | Partially reversible at best; cancer risk remains |
| Associated disease | Acute eosinophilic pneumonia | COPD, chronic bronchitis, emphysema, lung cancer, RB-ILD, DIP |
| Reid index | Normal (≈ 0.4) | Elevated (> 0.4), proportional to severity |
| Cilia function | Early impairment | Severe, chronic impairment with recurrent infections |
- Robbins & Kumar Basic Pathology (eFig. 11.6; p. 487)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 637)
- Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.