Thiopentone sodium
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to write a thorough answer. Let me compile everything.
Thiopentone Sodium (Sodium Thiopental)
Classification & Chemistry
Thiopentone sodium is an ultra-short-acting thiobarbiturate — a derivative of barbituric acid in which the oxygen at C2 is replaced by a sulfur atom (making it a thiobarbiturate). This substitution markedly increases lipid solubility, accounting for its rapid onset and short clinical duration after a single dose.
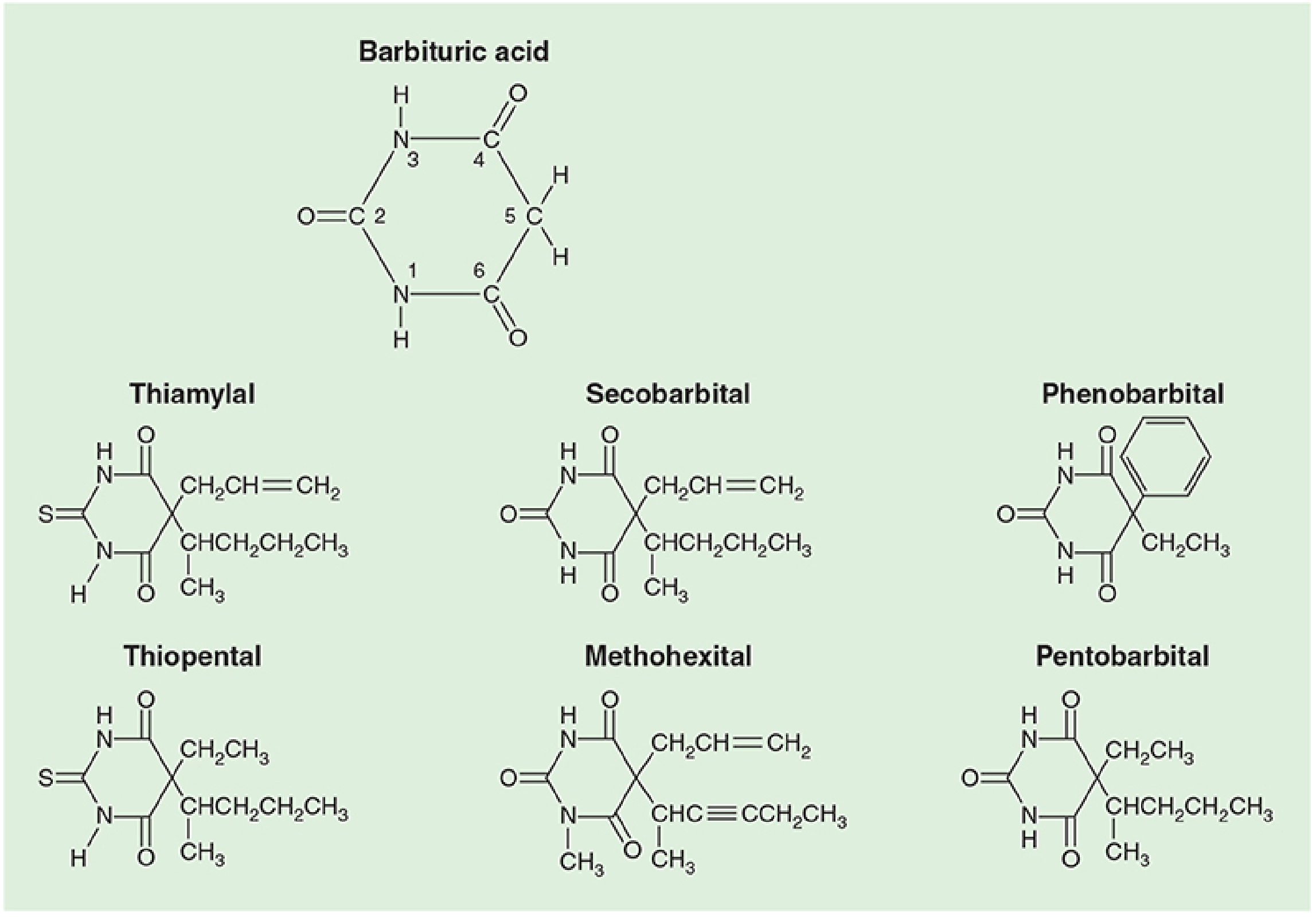
Barbituric acid derivatives. Note the sulfur at C2 in thiopental, compared to oxygen in oxybarbiturates like pentobarbital. — Morgan & Mikhail's Clinical Anesthesiology, 7e
- Supplied as the sodium salt with 6% sodium carbonate
- Reconstituted in water or saline → highly alkaline solution (pH ≥ 10)
- 2.5% solution has a shelf-life of ~2 weeks
- Racemic mixture (despite enantioselective anesthetic potency)
Mechanism of Action
Thiopentone acts primarily on the GABA-A receptor — at a site distinct from the benzodiazepine binding site. It prolongs the duration of chloride channel opening, enhancing inhibitory neurotransmission. It also:
- Inhibits kainate and AMPA receptors (excitatory)
- Depresses the reticular activating system in the brainstem, which controls consciousness
— Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 320
Pharmacokinetics
Absorption & Distribution
Administered intravenously (rarely rectally). High lipid solubility and a 60% non-ionized fraction at physiological pH → rapid brain uptake within 30 seconds.
After a single bolus, the duration of action is determined by redistribution, not metabolism:
- Drug moves rapidly from plasma → vessel-rich group (VRG: brain, heart, liver, kidney) → muscle group (MG) → fat group (FG)
- Plasma and brain concentrations fall to ~10% of peak within 20–30 minutes
- Patient loses consciousness in ~30 s; awakens within ~20 min
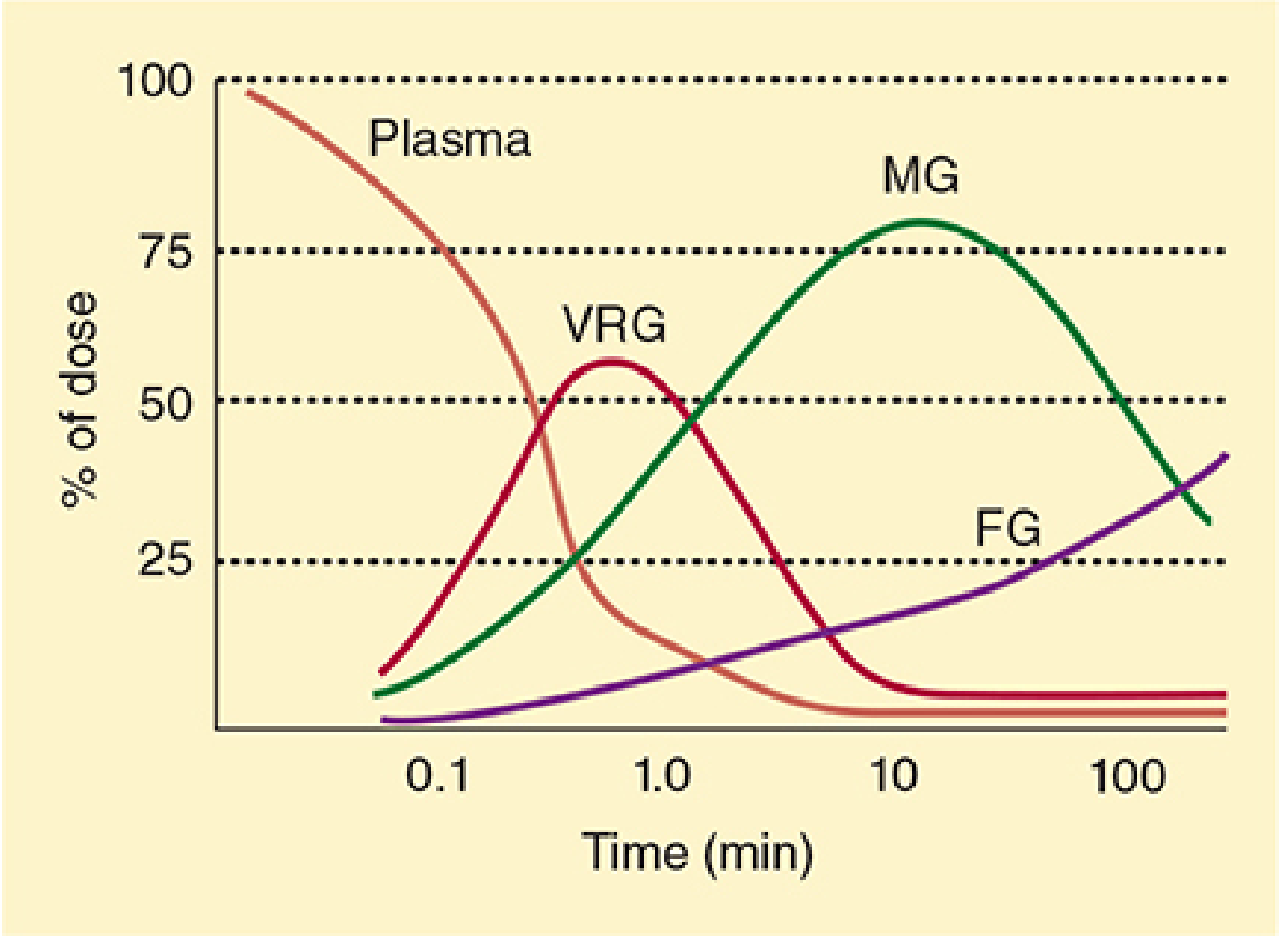
Redistribution of thiopental from plasma to the vessel-rich group (VRG), muscle group (MG), and fat group (FG). — Morgan & Mikhail's Clinical Anesthesiology, 7e
Key clinical point: With repeated dosing or infusions, peripheral compartments saturate → duration becomes dependent on elimination rather than redistribution (context-sensitive accumulation → "barbiturate coma" can last days).
Protein Binding & Special Populations
Thiopentone is highly protein-bound (to albumin). In:
- Hypovolemic shock → contracted central compartment → higher brain concentration per dose
- Low albumin (liver disease, malnutrition) → more free drug → enhanced effect
- Acidosis → increased non-ionized fraction → more CNS penetration
Dose requirements are reduced in older adults.
Biotransformation & Elimination
- Hepatic oxidation (primary), plus N-dealkylation, desulfuration, ring destruction
- A small fraction undergoes desulfuration to pentobarbital (a longer-acting hypnotic)
- Elimination half-life: 10–12 hours (prolonged vs. redistribution half-life)
- Metabolites are water-soluble → renally excreted
— Katzung's Basic & Clinical Pharmacology, 16e, p. 2395–2397
Dosage
| Use | Route | Concentration | Dose |
|---|---|---|---|
| Induction of anesthesia | IV | 2.5% | 3–6 mg/kg |
| Seizure control | IV | 2.5% | 50–100 mg (briefly) |
| Neonatal induction | IV | — | 2–4 mg/kg |
— Morgan & Mikhail's Clinical Anesthesiology, 7e, Table 9-1; Katzung, 16e
The standard induction dose is 3–5 mg/kg IV, producing unconsciousness in <30 seconds. Some patients describe a garlic, onion, or pizza taste on injection.
Organ System Effects
CNS
- Dose-dependent depression: sedation → anesthesia → EEG burst suppression → isoelectric EEG
- Potent cerebral vasoconstrictor → ↓ cerebral blood flow (CBF), ↓ cerebral blood volume, ↓ ICP
- ↓ CMRO₂ (cerebral metabolic rate for O₂) in a dose-dependent manner
- Anticonvulsant at sub-anesthetic doses (unlike methohexital)
- No analgesia — in fact, sub-anesthetic doses may lower pain threshold (hyperalgesia)
- No muscle relaxation; does not produce amnesia reliably
Useful for neuroprotection in focal ischemia (e.g., temporary clips during aneurysm surgery, surgical retraction), but likely does not protect from global ischemia (e.g., cardiac arrest).
Cardiovascular
- Bolus induction → ↓ blood pressure (vasodilation, venous pooling) + ↑ heart rate (reflex tachycardia, central vagolytic effect)
- Direct negative inotropic effect (less pronounced than propofol)
- Baroreceptor reflex is blunted but less so than with propofol → compensatory HR increase limits BP fall
- In hypovolemia, tamponade, cardiomyopathy, or β-blockade: compensatory mechanisms fail → dramatic ↓ BP and cardiac output
- Patients with poorly controlled hypertension are prone to wide BP swings
Respiratory
- Respiratory depressant: ↓ tidal volume, ↓ respiratory rate, ↓ minute ventilation
- Blunts ventilatory response to hypercapnia and hypoxia
- Induction dose typically causes transient apnea
- Laryngeal and cough reflex suppression less complete than propofol → inferior for airway instrumentation without neuromuscular blockade
- Risk of laryngospasm or bronchospasm if airway stimulated under inadequate depth
Renal
- ↓ renal blood flow and GFR proportional to ↓ blood pressure
Hepatic
- ↓ hepatic blood flow
- Chronic exposure → hepatic enzyme induction → accelerated metabolism of other drugs
- Inhibits cytochrome P-450 → interferes with biotransformation of other drugs (e.g., tricyclic antidepressants)
Clinical Uses
- Induction of general anesthesia — the principal use; historically the most widely used induction agent before propofol
- Control of grand mal seizures (50–100 mg IV, briefly effective)
- Raised ICP management — reduces CBF and ICP in space-occupying lesions
- Neuroprotection during neurosurgery (focal ischemia)
- "Barbiturate coma" — high-dose infusion for refractory raised ICP (EEG burst suppression endpoint)
- Safe in malignant hyperthermia (MH)-susceptible patients — does not trigger MH
Contraindications
| Contraindication | Reason |
|---|---|
| Acute intermittent porphyria / variegate porphyria | Stimulates aminolevulinic acid synthetase → induces porphyrin synthesis → precipitates crisis |
| Severe hypovolemia / hemorrhagic shock | Catastrophic hypotension |
| Cardiac tamponade, severe cardiomyopathy | Inability to compensate for vasodilation |
| Known barbiturate allergy | Rare anaphylaxis/anaphylactoid reactions |
| Neonates with congenital heart disease | Myocardial depression → hypotension |
| Airway obstruction (relative) | Inadequate laryngeal reflex suppression |
Adverse Effects & Complications
| Effect | Notes |
|---|---|
| Hypotension | Especially with rapid injection or hypovolemia |
| Apnea | Transient; nearly universal with induction doses |
| Laryngospasm / bronchospasm | If airway stimulated under light anesthesia |
| Intra-arterial injection | Excruciating pain + intense vasoconstriction → tissue gangrene; treat with stellate ganglion block |
| Extravasation | Local necrosis; dilute with 0.5% lidocaine 5–10 mL |
| Histamine release | Thiobarbiturates (sulfur-containing) evoke mast cell histamine release; oxybarbiturates do not |
| Anaphylaxis | Rare (~1 in 30,000 patients) |
| Context-sensitive accumulation | Prolonged infusions → unconsciousness lasting days |
| Hyperalgesia | Sub-anesthetic doses may lower pain threshold |
Drug Interactions
- Contrast media, sulfonamides: displace thiopentone from albumin → increased free drug → enhanced effect
- Alcohol, opioids, antihistamines, CNS depressants: potentiate sedation
- Acidic drugs (e.g., muscle relaxants at low pH): co-injection causes precipitation of thiopentone free acid in IV line — always flush the line between drugs
Comparison: Thiopentone vs Propofol (Key Differences)
| Feature | Thiopentone | Propofol |
|---|---|---|
| BP fall | Less | More |
| Baroreceptor blunting | Less | More |
| Laryngeal reflex suppression | Less | More |
| Recovery | Context-sensitive (slower with repeats) | Faster, more complete |
| Anticonvulsant | Yes | Yes (but activates epileptic foci less than methohexital) |
| Analgesia | No (hyperalgesia) | No |
Availability Note
Thiopentone has been unavailable in the USA due to shortage and controversy over its use in lethal injection protocols. It remains in use in other countries, particularly for resource-limited settings and neuroanesthesia.
— Barash, Cullen & Stoelting's Clinical Anesthesia, 9e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Morgan & Mikhail's Clinical Anesthesiology, 7e; Katzung's Basic & Clinical Pharmacology, 16e
This is a shared conversation. Sign in to Orris to start your own chat.