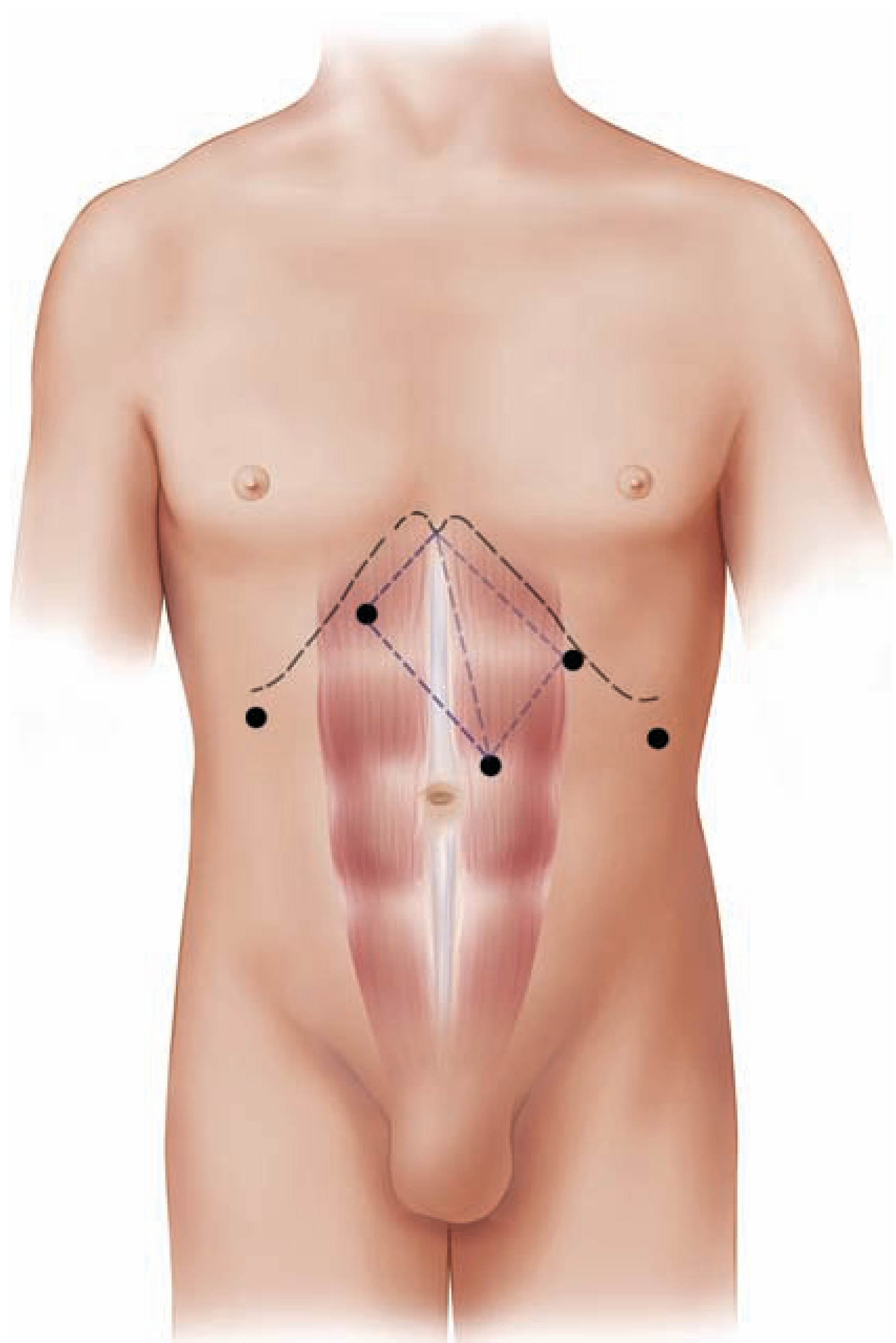
Laparoscopic entry points in abdomen
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have comprehensive textbook content and diagrams. Here is the full answer:
Laparoscopic Entry Points in the Abdomen
Overview of Access Methods
Two fundamental methods exist for establishing abdominal access in laparoscopy:
- Closed (Direct Puncture) technique - using a Veress needle
- Open (Hasson) technique - direct cut-down under vision
1. Primary Port (Camera Port) - Entry Sites
Umbilicus (Most Common)
The umbilicus is the preferred first point of access because:
- The abdominal wall is at its thinnest here, even in obese patients
- It provides a natural scar that heals well cosmetically
- The Veress needle, when angled toward the pelvis (away from the sacral promontory and great vessels), safely enters the peritoneal cavity
Veress Needle Technique at the Umbilicus:
- Abdominal wall is elevated with fingers or penetrating towel clips
- A small skin incision is made in/below the umbilicus
- The spring-loaded Veress needle is advanced - two distinct "pops" are felt as it passes through the fascia, then peritoneum
- CO2 is insufflated to 14-15 mmHg
- A 5 or 10 mm trocar is then placed through the same site
Hasson (Open) Technique at the Umbilicus:
- A small incision just below the umbilicus exposes the fascia under direct vision
- Two Kocher clamps are placed on the fascia; curved Mayo scissors incise the fascia and peritoneum
- A finger is inserted to confirm no adherent bowel
- A blunt, winged (Hasson) trocar is placed and secured with fascial sutures
- Preferred in: patients with previous abdominal surgery where bowel may be adherent to the undersurface of the anterior abdominal wall
Left Upper Quadrant - Palmer's Point
- Located in the left midclavicular line, 3 cm below the costal margin
- Used when the umbilical region is unsafe (previous midline laparotomy, umbilical hernia, suspected adhesions around the umbilicus)
- Accessed with a Veress needle or 5 mm optical trocar
- Also used as the initial entry site in laparoscopic ventral hernia repair and IPOM procedures
2. Secondary Ports (Working Ports)
Secondary/accessory trocars are placed after the pneumoperitoneum is established and the abdomen is being viewed through the primary camera port.
Key principles for secondary port placement:
- The abdominal wall must be transilluminated before puncture to avoid the inferior epigastric vessels (which run lateral to the rectus sheath)
- The trocar entry must be watched laparoscopically as it enters the abdomen
- Ports should not be placed too close together (to avoid "sword fighting" of instruments)
Common secondary port sites:
| Site | Size | Purpose |
|---|---|---|
| Epigastric (midline, 5-10 cm above umbilicus) | 5-12 mm | Liver retractor, working port for upper GI procedures |
| Right/Left hypochondrium (midclavicular) | 5-12 mm | Working ports for cholecystectomy, fundoplication |
| Right/Left iliac fossa | 5-12 mm | Working ports for appendicectomy, colorectal, gynaecological procedures |
| Suprapubic | 5-12 mm | Bladder procedures, pelvic dissection |
| Right/Left lateral flank | 5-12 mm | Retroperitoneal access, splenic/adrenal procedures |
3. The "Diamond of Success" - Optimal Port Configuration
The optimal port arrangement follows a baseball diamond (or diamond/rhombus) pattern:
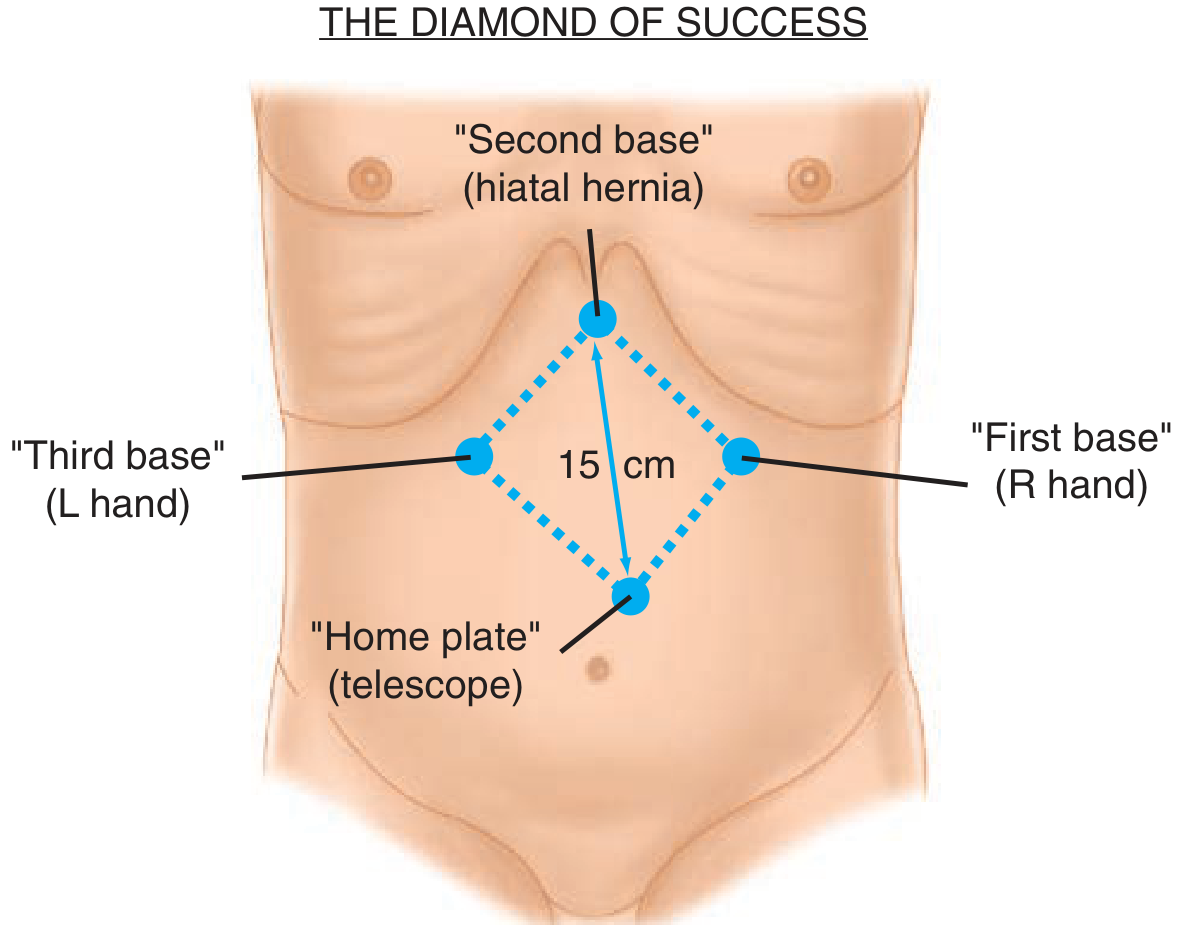
- Home plate = telescope port (periumbilical)
- Second base = surgical target (e.g., hiatus for fundoplication)
- First base = right-hand working port
- Third base = left-hand working port
- Ideal distance between telescope and target = 15 cm
- Ideal angle between the two working instruments at the target = 60-90 degrees
This configuration prevents instrument collision ("sword fighting") and optimizes ergonomics.
4. Anatomical Hazards at Each Entry Zone
| Entry Site | Key Structures at Risk |
|---|---|
| Umbilicus | Aorta/IVC bifurcation (~4-5 cm below in lean patients), adherent bowel in re-operative abdomen |
| Supraumbilical | Greater omentum, stomach (with distension), left lobe of liver |
| Epigastric | Falciform ligament, left lobe of liver |
| Lateral abdominal wall | Inferior epigastric vessels (transilluminate first!), circumflex iliac vessels |
| Right iliac fossa | Iliac vessels, right ureter, cecum/appendix |
| Left iliac fossa | Sigmoid colon, left ureter |
5. Entry in Special Situations
- Previous midline surgery: Use Palmer's point (LUQ) or an area away from previous scars; Hasson technique preferred
- Pregnancy: Entry point moves cephalad as the uterus enlarges; left upper quadrant or supra-fundal entry
- Obesity: Umbilicus remains thin despite overall obesity; Veress needle angle must be more perpendicular (abdominal wall is thicker)
- Port-site metastasis risk (cancer surgery): Extract specimen in a bag; fascial closure of ports >10 mm
- Children: Smaller abdomen means reduced safe working distances; use 3 mm and 5 mm trocars
6. Confirming Correct Intraperitoneal Placement (Veress Needle Tests)
Before insufflation, several checks confirm correct needle tip placement:
- Hanging drop test - saline placed at needle hub is drawn in by negative intraperitoneal pressure
- Aspiration test - no blood or bowel content on aspiration
- Insufflation pressure - initial pressure <8 mmHg with free flow indicates intraperitoneal position; high pressure suggests extraperitoneal/omental placement
- Volume of gas - first 1 L should insufflate easily and symmetrical abdominal distension should be visible
Sources:
- Schwartz's Principles of Surgery, 11th ed. - Chapter 14 (Minimally Invasive Surgery)
- Maingot's Abdominal Operations - Chapter 4 (Port Placement, "Diamond of Success")
- Fischer's Mastery of Surgery, 8th ed.
- Mulholland and Greenfield's Surgery, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.