Treatment algorithm of strock and pathophysiology in flow chart
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Both key flowcharts are retrieved. Here is the complete, structured response:
Stroke: Pathophysiology & Treatment Algorithm
Sources: Harrison's Principles of Internal Medicine 22E (2025), Bradley and Daroff's Neurology in Clinical Practice
1. Pathophysiology of Ischemic Stroke — Cascade Flowchart
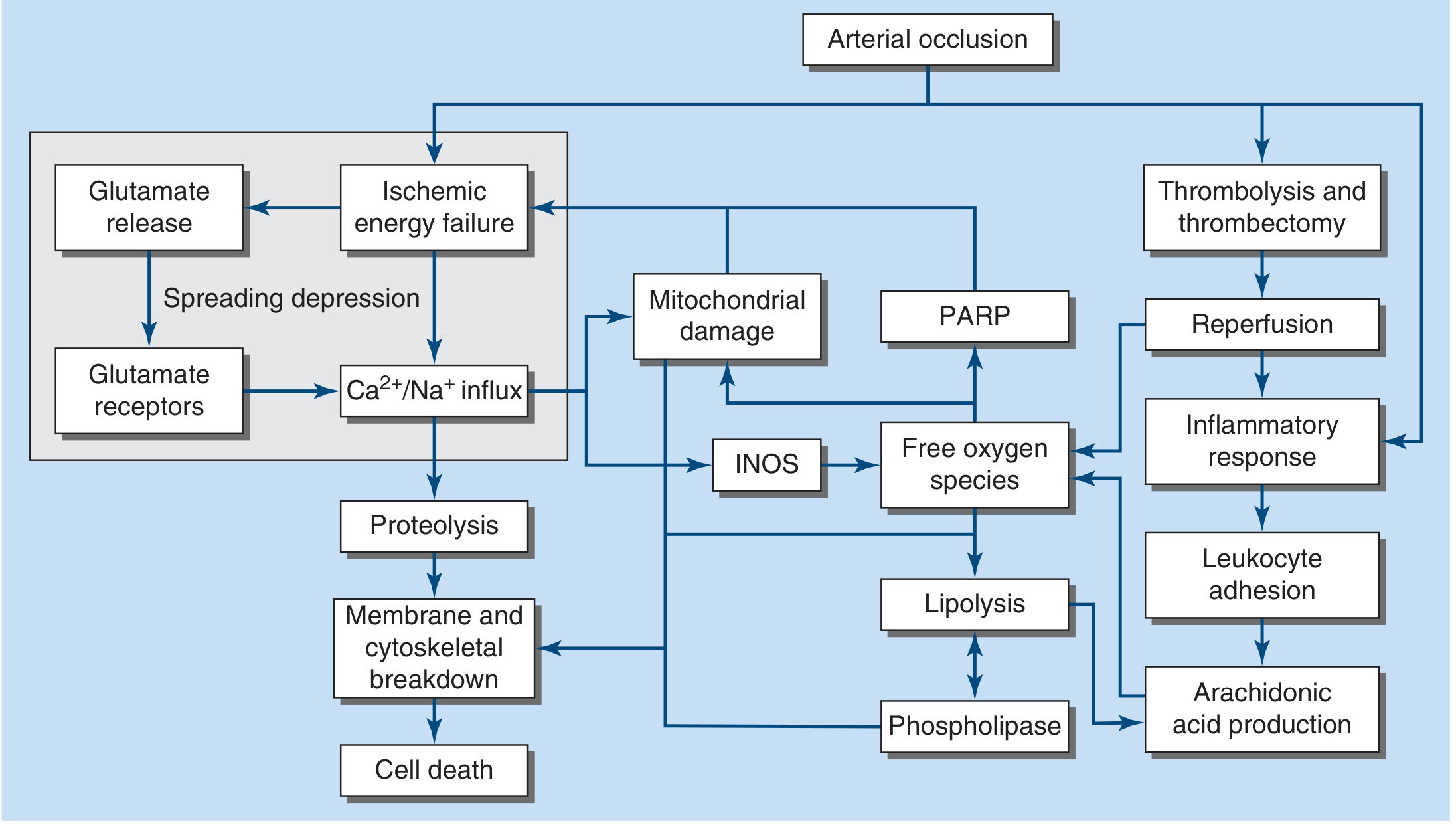
Figure 438-1 — Major steps in the cascade of cerebral ischemia. NOS, inducible nitric oxide synthase; PARP, poly-A ribose polymerase. — Harrison's Principles of Internal Medicine 22E
Key Steps Explained
| Step | Mechanism |
|---|---|
| Arterial occlusion | Thrombotic, embolic, or lacunar; reduces CBF |
| Ischemic energy failure | CBF <16–18 mL/100 g/min → ATP depletion within minutes |
| Glutamate release | Excitotoxicity via NMDA/AMPA receptor activation |
| Ca²⁺/Na⁺ influx | Membrane depolarisation → ionic pump failure → spreading depression |
| Proteolysis | Calpain/caspase activation → cytoskeletal breakdown |
| Mitochondrial damage | ROS generation, cytochrome c release → apoptosis |
| iNOS activation | → Free oxygen species → lipid peroxidation, PARP activation |
| Phospholipase/Lipolysis | Membrane phospholipid degradation → arachidonic acid → inflammation |
| Reperfusion injury | Thrombolysis/thrombectomy restores flow but triggers inflammatory response, leukocyte adhesion, arachidonic acid production |
| Cell death | Necrosis (core) and apoptosis (penumbra) |
Core vs. Penumbra: CBF to zero → tissue death in 4–10 min. The ischemic penumbra — surrounding tissue with reduced but not zero flow — is salvageable if reperfusion occurs promptly.
2. Acute Stroke Treatment Algorithm — Flowchart
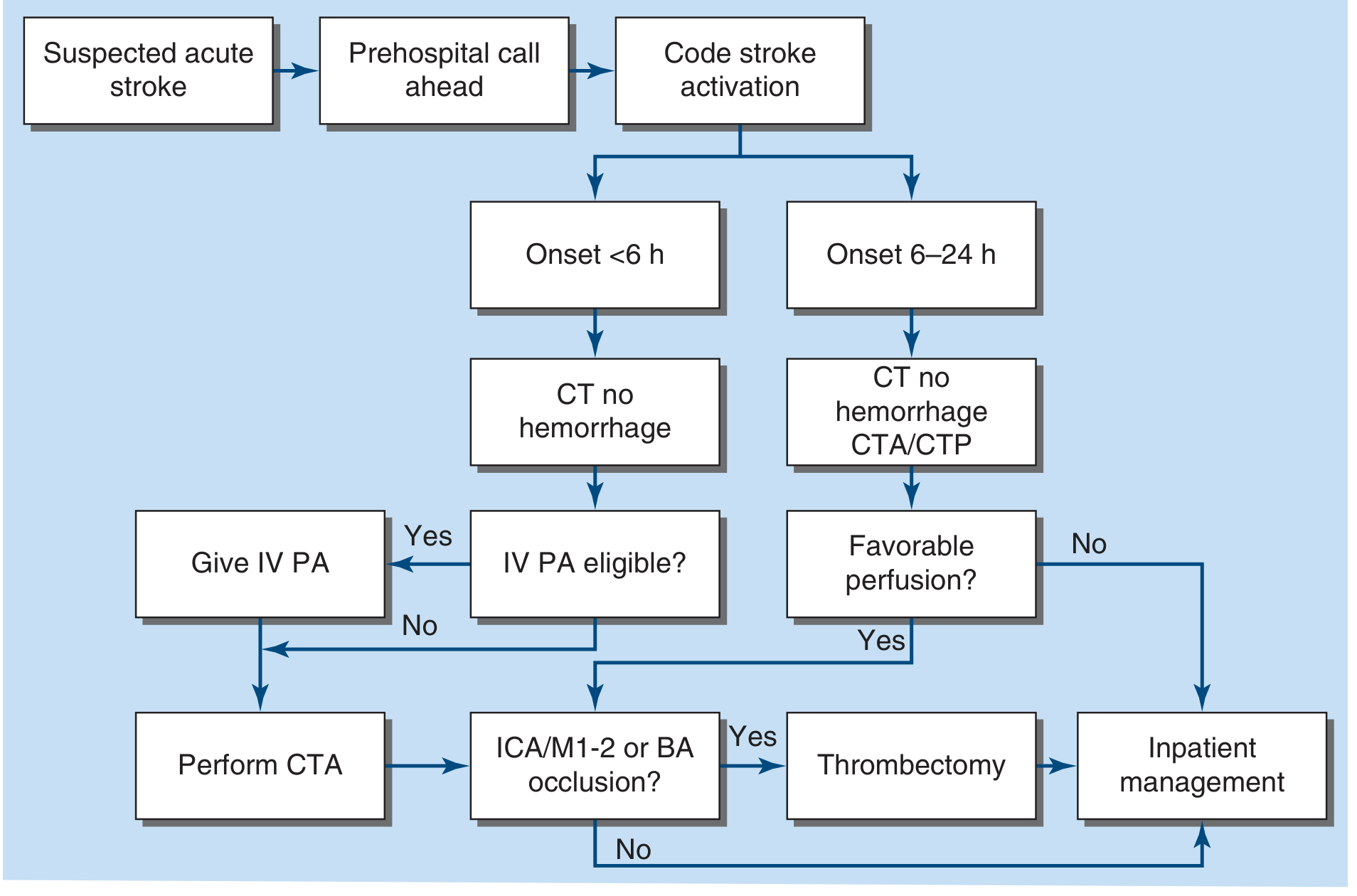
Figure 438-2 — Management of acute stroke. PA = plasminogen activator (tPA or tenecteplase); ICA = internal carotid artery; M1/M2 = MCA divisions; BA = basilar artery; CTA = CT angiography; CTP = CT perfusion. — Harrison's Principles of Internal Medicine 22E
3. Structured Treatment Algorithm (Text Supplement)
Step 1 — Recognition & Prehospital
- Identify stroke signs (FAST: Face, Arm, Speech, Time)
- Prehospital call ahead → Code Stroke activation on arrival
Step 2 — Immediate ED Assessment (ABCs + glucose)
- Airway, breathing, circulation
- Finger-stick glucose (treat hypo- and hyperglycaemia; target 60–180 mg/dL)
- Establish time last seen normal (LSN)
- NIHSS scoring
Step 3 — Emergency Neuroimaging
| Finding | Action |
|---|---|
| Hemorrhage on CT | → Hemorrhagic stroke pathway (neurosurgery, BP control, reverse anticoagulation) |
| No hemorrhage, onset <4.5 h | → Assess IV thrombolysis eligibility |
| No hemorrhage, onset <6 h | → IV PA if eligible; proceed to CTA |
| Onset 6–24 h | → CT perfusion (CTP) + CTA to assess penumbra |
Step 4 — Reperfusion Decisions
IV Thrombolysis
- Agent: Alteplase 0.9 mg/kg IV (max 90 mg) OR Tenecteplase (single bolus)
- Window: ≤4.5 h from LSN (AHA/ASA 2019 guidelines)
- Key contraindication: BP >185/110 mmHg (must be controlled first), prior intracranial hemorrhage, active bleeding
- Give bolus in CT scanner → start infusion immediately
Endovascular Thrombectomy (EVT)
- Indicated if CTA shows ICA, M1, M2, or basilar artery occlusion
- Window: up to 24 h from LSN if favorable perfusion imaging (DAWN/DEFUSE-3 criteria)
- Can be combined with IV tPA ("bridging therapy")
Step 5 — Medical Support (all stroke patients)
| Domain | Intervention |
|---|---|
| Blood pressure | Allow permissive HTN if not thrombolysing; lower only if >220/120 mmHg (or >185/110 before tPA) |
| Glucose | Target 60–180 mg/dL |
| Fever | Antipyretics + surface cooling |
| DVT prophylaxis | Subcutaneous heparin or pneumatic compression stockings |
| Cerebral oedema | Mannitol / hypertonic saline; hemicraniectomy for malignant MCA infarct |
Step 6 — Secondary Prevention (post-acute)
| Aetiology | Agent |
|---|---|
| Non-cardioembolic stroke | Dual antiplatelet (aspirin 81 mg + clopidogrel or ticagrelor) for 21–30 days → aspirin monotherapy |
| Atrial fibrillation | Oral anticoagulation (apixaban 5 mg BD preferred) |
| Significant carotid stenosis (>50%) | Carotid endarterectomy (same admission) |
| Intracranial atherosclerosis | Dual antiplatelet ≥3 months |
| All patients | High-intensity statin (atorvastatin 80 mg or rosuvastatin 40 mg); target LDL <70 mg/dL |
| Long-term BP | Target systolic <120 mmHg (after acute phase) |
Step 7 — Rehabilitation
- Early mobilisation, speech therapy, physiotherapy
- Stroke unit care reduces mortality and disability independent of thrombolysis
Quick Summary Mnemonic
"Time = Brain" — 1.9 million neurons die every minute without reperfusionPathway: Suspect → CT (exclude bleed) → Time window → tPA if eligible → CTA → Thrombectomy if large vessel occlusion → Medical support → Secondary prevention → Rehab
Non pharmacological treatment
Asking for Preferences
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple sources. Here is the complete answer:
Non-Pharmacological Treatment of Stroke
Sources: Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine, Rosen's Emergency Medicine
Non-pharmacological treatments span three phases: acute interventions, rehabilitation, and long-term lifestyle modification for secondary prevention.
Phase 1 — Acute Non-Pharmacological Interventions
1. Reperfusion Procedures (Mechanical)
| Procedure | Details |
|---|---|
| Mechanical Thrombectomy (EVT) | Catheter-based clot retrieval for large vessel occlusion (ICA, M1/M2, basilar artery); up to 24 h window with favourable perfusion imaging |
| Carotid Endarterectomy (CEA) | For significant internal carotid stenosis (>50%); ideally performed during the same admission to prevent recurrence |
| Carotid Artery Stenting | Alternative to CEA in surgically high-risk patients |
2. Decompressive Hemicraniectomy
- Indicated for malignant MCA infarct with severe cytotoxic oedema
- Most beneficial when performed <48 hours in patients <60 years of age
- Reduces 6-month mortality significantly (RescueICP data)
- Surgical options also include: ventriculostomy (CSF drainage) for raised ICP, evacuation of intracranial haematoma (for haemorrhagic stroke)
3. Temperature Management
- Fever is detrimental — every 1°C rise increases cerebral metabolic demand by 8–13%, escalates glutamate release and free radical production
- Treat all temperatures >38°C aggressively with surface cooling devices
- Targeted hypothermia (32–36°C) is an option in refractory raised ICP, though evidence for routine use in ischaemic stroke is limited
4. Airway & Positioning
- Maintain airway patency; intubate if GCS ≤8 or aspiration risk
- Head-of-bed positioning: generally 0–30° flat to optimise cerebral perfusion pressure in acute phase (unless oedema or aspiration risk mandates elevation)
5. DVT Prophylaxis (Mechanical)
- Pneumatic compression stockings — proven benefit in reducing DVT risk; safe alternative when heparin is contraindicated
- Early mobilisation when medically stable
Phase 2 — Rehabilitation (Post-Acute)
Stroke Unit Care
- Dedicated stroke units with multidisciplinary teams reduce mortality and disability independent of any drug therapy — one of the most evidence-based interventions in stroke care
- Telestroke/telemedicine services extend specialist care to peripheral hospitals
- Standardised stroke order sets and clinical pathways improve outcomes
Core Rehabilitation Therapies
| Therapy | Goals |
|---|---|
| Physiotherapy (PT) | Restore motor function, balance, gait; prevent contractures and falls |
| Occupational Therapy (OT) | Restore ADLs (dressing, feeding, hygiene); adaptive equipment |
| Speech and Language Therapy (SLT) | Address aphasia, dysarthria, and dysphagia (swallow assessment critical before oral feeding) |
| Neuropsychological support | Cognitive rehabilitation; treat post-stroke depression |
Constraint-Induced Movement Therapy (CIMT)
- Immobilises the unaffected limb to force use of the paretic limb
- Shown to improve hemiparesis even years after stroke, demonstrating neural plasticity
- Evidence supports recruitment of previously unused neural pathways
Emerging Neuromodulation Therapies (Under Investigation)
| Modality | Mechanism |
|---|---|
| Transcranial Magnetic Stimulation (TMS) | Non-invasive cortical excitability modulation |
| Transcranial Direct Current Stimulation (tDCS) | Low-level current to enhance cortical plasticity |
| Robotic-assisted therapy | Repetitive, high-intensity task-specific training |
| Virtual reality rehabilitation | Immersive task practice for motor and cognitive recovery |
Swallowing & Nutrition
- All stroke patients require formal swallow assessment before oral intake
- Nasogastric feeding or PEG tube for persistent dysphagia
- Nutritional support prevents aspiration pneumonia (a leading cause of post-stroke mortality)
Psychological & Social Support
- Post-stroke depression affects ~30% of patients — psychological counselling, peer support groups
- Family and carer education on assisting with exercises and preventing learned non-use
- Community reintegration and vocational rehabilitation
Phase 3 — Long-Term Lifestyle Modification (Secondary Prevention)
These address the modifiable risk factors that caused or contributed to the stroke:
| Risk Factor | Non-Pharmacological Intervention |
|---|---|
| Hypertension | Dietary sodium restriction (<2 g/day), DASH diet, weight loss, regular aerobic exercise, limit alcohol |
| Obesity | Caloric restriction, structured weight-loss programme; target BMI <25 |
| Physical inactivity | ≥150 min/week moderate aerobic exercise (e.g., walking, swimming) |
| Smoking | Smoking cessation — single most impactful modifiable risk factor after hypertension |
| Excess alcohol | Limit to ≤1 unit/day (women) / ≤2 units/day (men); heavy use markedly increases risk |
| Poor diet | Mediterranean or DASH diet; increase fruits, vegetables, whole grains, fish; reduce saturated fat |
| Diabetes | Glycaemic control through diet and exercise; target HbA1c <7% |
| Sleep apnoea | CPAP therapy — untreated OSA is an independent stroke risk factor |
| Atrial fibrillation | Rate control via exercise and weight loss; avoid triggers (alcohol, caffeine excess) |
Summary Framework
NON-PHARMACOLOGICAL TREATMENT OF STROKE
│
├── ACUTE PHASE
│ ├── Mechanical thrombectomy (large vessel occlusion)
│ ├── Carotid endarterectomy / stenting
│ ├── Decompressive hemicraniectomy (malignant MCA oedema)
│ ├── Temperature control (surface cooling)
│ ├── Airway management & positioning
│ └── Mechanical DVT prophylaxis (compression stockings)
│
├── REHABILITATION PHASE
│ ├── Stroke unit care (multidisciplinary team)
│ ├── Physiotherapy — motor recovery, gait
│ ├── Occupational therapy — ADLs
│ ├── Speech therapy — aphasia, dysphagia
│ ├── Constraint-induced movement therapy
│ ├── Swallowing assessment & nutrition support
│ ├── Neuromodulation (TMS, tDCS) — investigational
│ ├── Robotic therapy — investigational
│ └── Psychological support / post-stroke depression
│
└── SECONDARY PREVENTION (Lifestyle)
├── Smoking cessation
├── Aerobic exercise ≥150 min/week
├── DASH/Mediterranean diet
├── Weight reduction
├── Alcohol restriction
├── Sleep apnoea treatment (CPAP)
└── Glycaemic control through diet
Key principle: Stroke unit care + early multidisciplinary rehabilitation is among the most powerful non-pharmacological interventions available — with outcome benefits equivalent to or exceeding most individual drug therapies. — Harrison's Principles of Internal Medicine 22E
Write introduction, definition,etiology , pathophysiology,signs and symptoms,pharmacotherapy, treatment algorithm, adr of drugs moa , types
Asking for Preferences
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
For peptic ulcer
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.