Mpfl reconstruction in orthopaedics 10 marks pg answer with flow chart and images
MPFL reconstruction orthopaedics surgical technique anatomy graft fixation
MPFL reconstruction indications technique Schottle point graft isometry 10 marks exam answer
https://pmc.ncbi.nlm.nih.gov/articles/PMC7944812
MPFL anatomy Schottle point isometry graft semitendinosus gracilis complications rehabilitation site:pubmed.ncbi.nlm.nih.gov OR site:pmc.ncbi.nlm.nih.gov
MPFL reconstruction anatomy diagram Schottle point patella images site:radiopaedia.org OR site:orthopaedia.com OR site:boneandjoint.org
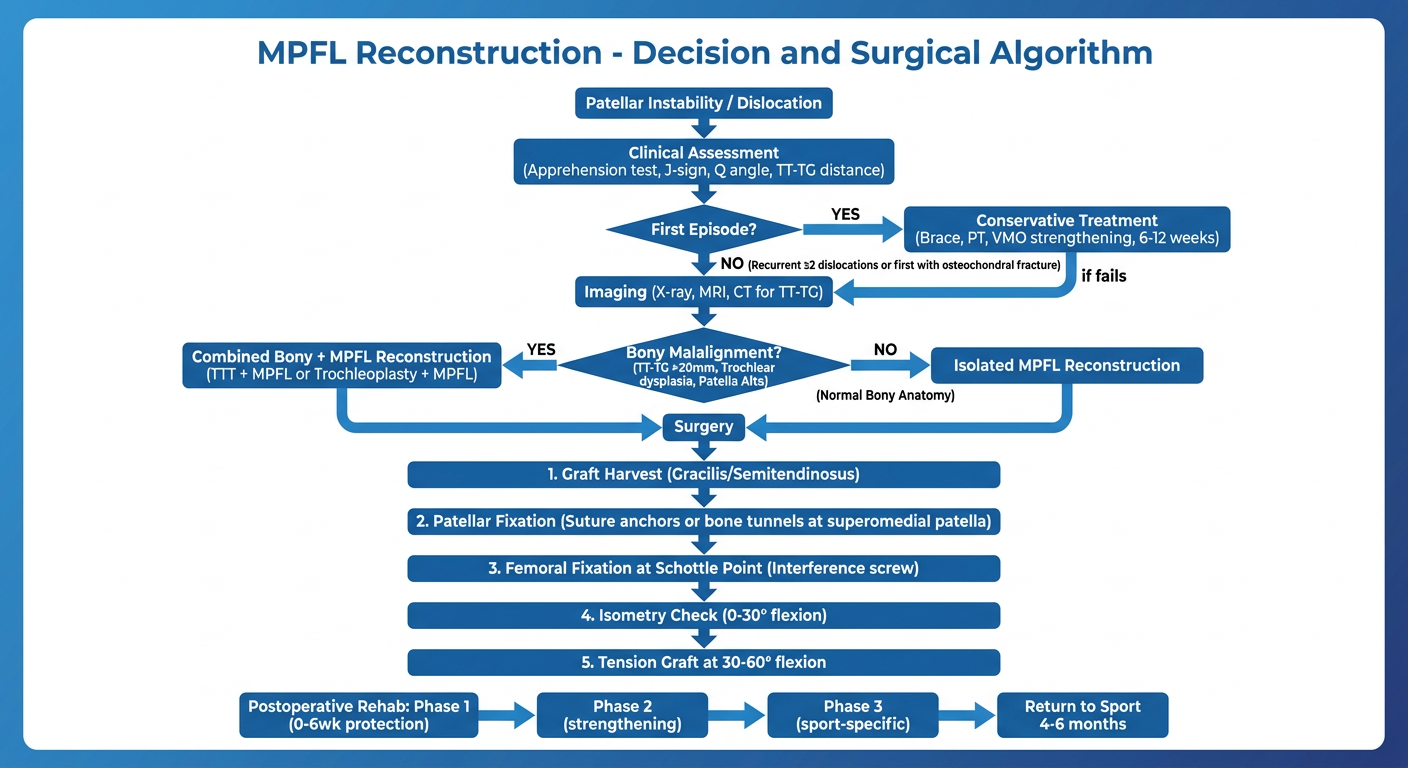
A clean medical flowchart titled "MPFL Reconstruction - Decision and Surgical Algorithm" with the following flow: Box 1: "Patellar Instability / Dislocation" → Box 2: "Clinical Assessment (Apprehension test, J-sign, Q angle, TT-TG distance)" → Decision diamond: "First Episode?" → YES branch: "Conservative Treatment (Brace, PT, VMO strengthening, 6-12 weeks)" → if fails → Surgery. NO branch (Recurrent ≥2 dislocations or first with osteochondral fracture): "Imaging (X-ray, MRI, CT for TT-TG)" → Decision diamond "Bony Malalignment? (TT-TG >20mm, Trochlear dysplasia, Patella Alta)" → YES: "Combined Bony + MPFL Reconstruction (TTT + MPFL or Trochleoplasty + MPFL)" → NO (Normal Bony Anatomy): "Isolated MPFL Reconstruction". Then below the surgery box: Step-by-step surgical steps in a vertical flow: "1. Graft Harvest (Gracilis/Semitendinosus)" → "2. Patellar Fixation (Suture anchors or bone tunnels at superomedial patella)" → "3. Femoral Fixation at Schottle Point (Interference screw)" → "4. Isometry Check (0-30° flexion)" → "5. Tension Graft at 30-60° flexion" → "Postoperative Rehab: Phase 1 (0-6wk protection) → Phase 2 (strengthening) → Phase 3 (sport-specific) → Return to Sport 4-6 months". Use blue and white color scheme, clean modern medical style, clear arrows and labels.
MPFL Reconstruction - 10 Marks PG Answer
Definition
Anatomy
| Structure | Details |
|---|---|
| Patellar attachment | Superomedial border of patella (upper 2/3 of medial border) |
| Femoral attachment | Schottle's point: midpoint between medial epicondyle and adductor tubercle, anterior to the posterior femoral cortex on lateral X-ray |
| Length | ~55 mm |
| Tensile strength | ~208 N (native) |
| Depth | Deep to the medial retinaculum, superficial to the medial joint capsule |

Patellofemoral Instability - Predisposing Factors (TAMP mnemonic)
- Trochlear dysplasia (most important bony risk factor)
- Alta - Patella alta (Caton-Deschamps index >1.2)
- Malalignment - Increased TT-TG distance (>20 mm = abnormal)
- Positional - Hyperlaxity, Q angle >20°, female sex, age <15 years
Indications for MPFL Reconstruction
Absolute Indications
- Recurrent patellar dislocation (≥2 episodes) with failure of conservative treatment
- First-time dislocation with associated osteochondral fracture requiring fixation
- Ongoing symptoms of patellar instability after appropriate non-operative management
Relative Indications
- First-time dislocation in elite athletes
- Mild bony malalignment (TT-TG 15-20 mm) - combined with bony procedure
- Symptomatic patellar subluxation refractory to physiotherapy
Contraindications
- Significant trochlear dysplasia (Dejour C/D) - needs trochleoplasty first or combined
- TT-TG >20 mm - tibial tubercle transfer (TTT) required concomitantly
- Patella alta (Caton-Deschamps >1.4) - anteromedial TTT or distalization needed
- Uncorrected bony malalignment as isolated MPFL reconstruction will fail
Pre-operative Assessment
Clinical
- Apprehension test (positive at 0-30° flexion)
- J-sign (patella jumps laterally at terminal extension)
- Q-angle measurement (>20° abnormal)
- Hyperlaxity assessment (Beighton score)
Investigations
- X-ray (AP, lateral, skyline/axial): Patella alta (Caton-Deschamps, Insall-Salvati ratio), trochlear dysplasia, crossing sign, supratrochlear spur
- CT scan: TT-TG distance (normal <15 mm, borderline 15-20 mm, abnormal >20 mm), torsional alignment
- MRI: MPFL tear location, chondral injury, trochlear morphology, bone edema ("kissing contusion" at lateral trochlea and medial patella)
Surgical Technique
Graft Options
| Graft | Strength | Notes |
|---|---|---|
| Gracilis autograft | ~1800 N | Most common; thin, appropriate length |
| Semitendinosus autograft (doubled) | ~2330 N | Stronger; over-constraint risk if not careful |
| Quadriceps tendon | Good | No separate harvest incision needed |
| Allograft (ST/gracilis) | Similar | No donor site morbidity; useful in revision |
Step-by-Step Technique
- Supine with tourniquet; knee over bolster; fluoroscopy available
- Arthroscopy first to assess chondral surfaces and confirm diagnosis
- Gracilis or semitendinosus via 2-3 cm incision posteromedial to tibial tuberosity
- Prepare to ~180-200 mm length, tubularize with whip stitch
- Double the graft for adequate strength
- 3 cm incision over medial border of patella
- Identify the superomedial patella - attachment is at the junction of the proximal 1/3 and middle 1/3
- Suture anchors (most common): Two 1.8-3.5 mm anchors placed in the medial patella
- OR Bone tunnels: Two converging tunnels in the patella (risk of iatrogenic fracture if <25 mm bone width)
- The graft is split into two limbs for double-bundle attachment
Schottle's point is located on lateral fluoroscopy: anterior to the posterior femoral cortex line, at the level of the posterior edge of Blumensaat's line, 1 mm proximal to a line drawn along the posterior cortex of the medial femoral condyle.
- 3 cm incision over medial femoral condyle
- Dissect between the superficial MCL and the vastus medialis
- Under fluoroscopic guidance, place a guide wire at Schottle's point
- Confirm isometry: anchor a suture at the femoral point, tie to patella, and check tension is equal from 0-90° flexion
- Drill a 7-8 mm tunnel; dock the graft with an interference screw at 30-60° knee flexion
- Fixation tension: patella should allow <1/4 width lateral translation; tracking must be smooth
- Fix the graft with knee at 30-60° flexion (patella fully engaged in trochlea at 60°)
- Graft should be non-isometric: slightly tighter in extension, looser in deeper flexion - avoid over-constraint
- Final check: patella tracks centrally with no excessive medial or lateral tilt
- Deep fascia repair, subcutaneous and skin closure
- Drain optional
Flowchart
Complications
Intraoperative
- Patellar fracture (bone tunnel technique; incidence 0.9-3.6%)
- Femoral guide-wire misplacement - nonanatomic graft leads to over-constraint
Early Postoperative
- Infection, haematoma
- Deep vein thrombosis
- Wound complications
Late Complications
| Complication | Cause |
|---|---|
| Recurrent instability (4-8%) | Tunnel malposition, inadequate tension, missed bony pathology |
| Patellofemoral pain/arthritis | Over-tensioning (too proximal/anterior femoral tunnel) → excessive medial PF compression |
| Stiffness / loss of flexion | Over-tightening; inadequate rehab |
| Graft failure | Technical error; fixation failure |
| Medial patellar chondral erosion | Excess medial loading from over-constraint |
Rehabilitation Protocol
| Phase | Timeline | Goals |
|---|---|---|
| Phase 1 - Protection | 0-6 weeks | Pain/swelling control, gentle ROM 0-90°, quadriceps activation, partial weight-bearing |
| Phase 2 - Strengthening | 6-12 weeks | Full ROM, closed chain strengthening (squat, leg press), proprioception, full weight-bearing |
| Phase 3 - Advanced Strengthening | 3-5 months | Sport-specific training, plyometrics, dynamic balance |
| Phase 4 - Return to Sport | 4-6 months | Full sports participation when quad strength ≥90% contralateral, limb symmetry index ≥90% |
Outcomes
- Success rates: 83-93% across all techniques
- Return to prior activity: ~90% of patients
- Re-dislocation rate with anatomic technique: <2-4%
- Key predictor of failure: nonanatomic femoral placement (accounts for 50% of graft failures)
Special Considerations
Skeletally Immature Patients
- Avoid drilling through the distal femoral physis
- Femoral fixation around the adductor magnus tendon (physeal-sparing technique) instead of a bone tunnel
- Tibial tubercle transfer deferred until skeletal maturity
Concomitant Procedures
- TT-TG >20 mm: Anteromedial tibial tubercle transfer (Fulkerson osteotomy) + MPFL
- Trochlear dysplasia (Dejour B/C/D): Trochleoplasty + MPFL
- Patella alta: Tubercle distalization or Caton-Deschamps correction + MPFL
- Osteochondral fragment: MPFL + fragment fixation or microfracture
Key Points to Remember for Exam
- MPFL provides 50-60% of medial restraint to lateral patellar translation
- Schottle's point is the femoral isometric attachment - the most critical step
- Graft fixed at 30-60° flexion to ensure correct length-tension relationship
- Over-tensioning → medial patellofemoral arthritis (most common pitfall)
- TT-TG >20 mm mandates bony realignment in addition to MPFL reconstruction
- Patellar fracture risk with bone tunnels - use suture anchors if patella width <25 mm
- Overall outcomes are excellent: >90% return to sport, <4% re-dislocation with anatomic technique