CIN 1
Reading File
Finding Sources
Searching PubMed
"cervical intraepithelial neoplasia" AND "CIN 1" AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of CIN 1, drawn from authoritative medical textbooks.
CIN 1 (Cervical Intraepithelial Neoplasia Grade 1)
Definition and Terminology
CIN 1 is the lowest grade of cervical precursor lesions. The classification system has evolved over time:
- Oldest system: mild dysplasia (CIN 1), moderate dysplasia (CIN 2), severe dysplasia/carcinoma in situ (CIN 3)
- Current 2-tier system: CIN 1 is now called Low-Grade Squamous Intraepithelial Lesion (LSIL); CIN 2 and CIN 3 are combined into High-Grade Squamous Intraepithelial Lesion (HSIL)
The shift to a two-tier system reflects the clinical reality that management is binary - observation vs. surgical treatment. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Etiology - HPV
CIN 1 is caused by Human Papillomavirus (HPV). Key facts:
- The squamo-columnar junction (SCJ) of the cervix is the most vulnerable site, due to its large area of immature squamous metaplastic epithelium
- High-risk HPV types: 16, 18, 31, 45 (and others) - use E6 and E7 oncoproteins to inactivate p53 and RB tumor suppressors
- Low-risk HPV types (e.g., 6, 11): E7 binds RB with lower affinity; E6 fails to bind p53 - instead disrupts Notch signaling
- In CIN 1/LSIL, viral DNA remains episomal (not integrated) - integration is associated with progression to cancer
- CIN 1 represents a productive HPV infection with high-level viral replication but only mild cellular growth disturbance
Risk cofactors: cigarette smoking, early first intercourse, multiple sexual partners, immunosuppression. - Robbins, Cotran & Kumar
Histopathology
Histological spectrum of CIN:
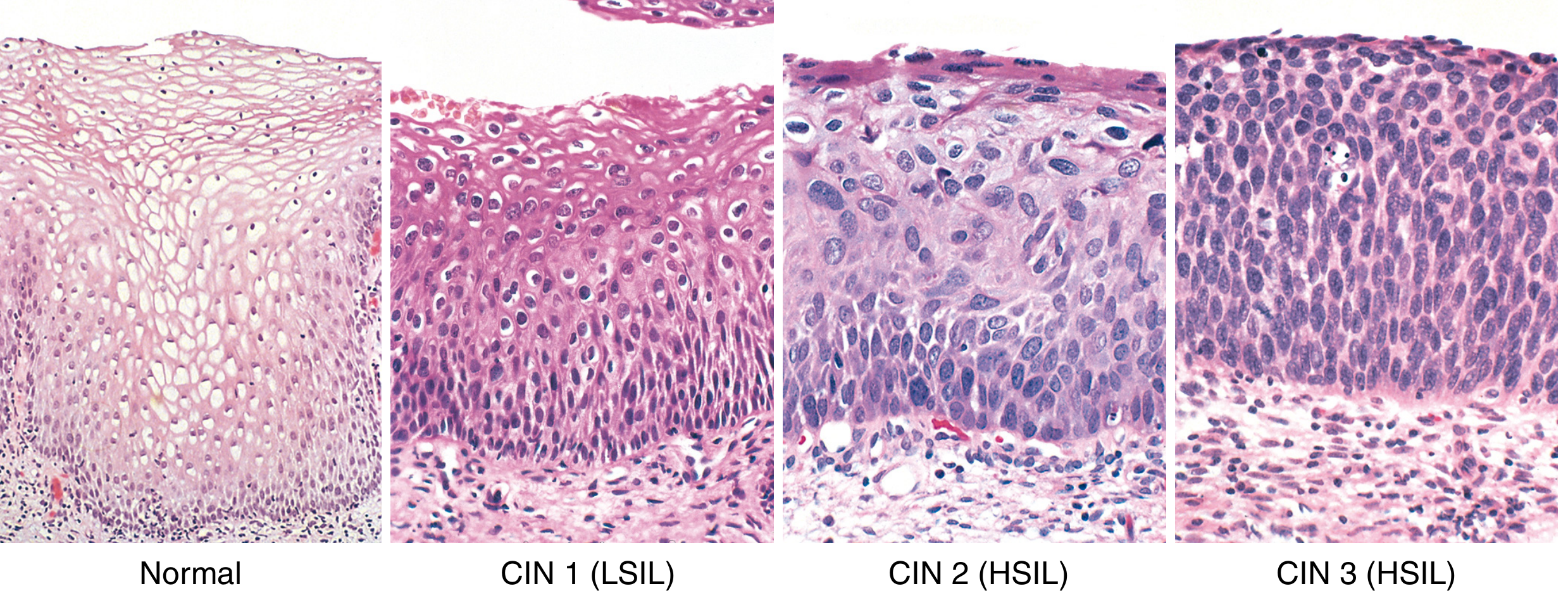
Fig. 22.14 - Spectrum of cervical intraepithelial neoplasia with normal squamous epithelium for comparison. From Robbins, Cotran & Kumar.
CIN 1 / LSIL specific features:
| Feature | Description |
|---|---|
| Immature cell layer extent | Confined to the lower 1/3 of the epithelium |
| Koilocytic atypia | Nuclear enlargement, hyperchromasia, perinuclear cytoplasmic halos |
| Nuclear changes | Coarse chromatin, variation in nuclear size/shape |
| Ki-67 expression | Abnormally expressed in upper epithelium (normally basal only) |
| p16 expression | Overexpressed (cyclin-dependent kinase inhibitor) |
| HPV DNA | Highest viral loads in maturing keratinocytes in the upper epithelium |
The perinuclear halos ("koilocytes") are caused by the HPV-encoded E5 protein localizing to endoplasmic reticulum membranes. - Robbins, Cotran & Kumar
In comparison: CIN 2 expands to the upper 2/3; CIN 3 has diffuse atypia and loss of maturation spanning the full epithelial thickness.
Natural History and Prognosis
- Most CIN 1 cases regress spontaneously - CIN 1/LSIL is approximately 10 times more common than HSIL
- Only a small percentage progresses to HSIL
- Because of the high spontaneous regression rate, CIN 1 is not treated as a premalignant lesion - it is managed conservatively
Management
Management flowchart for CIN 1 (ASCCP guidelines):
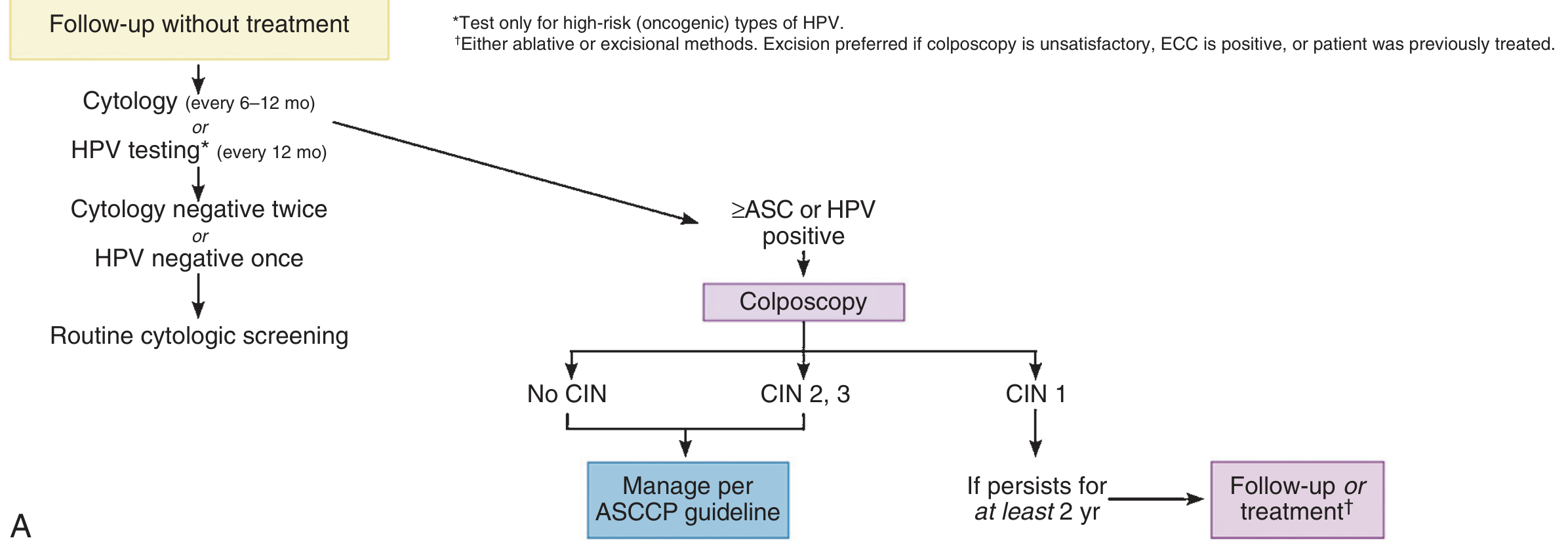
ASCCP consensus guidelines for CIN 1 preceded by ASC-US, ASC-H, or LSIL cytology. From Pfenninger & Fowler's Procedures for Primary Care.
Standard management options for biopsy-confirmed CIN 1:
-
Follow-up without treatment (preferred initial approach)
- Cytology every 6-12 months, or
- High-risk HPV testing every 12 months
- If cytology negative twice OR HPV negative once → return to routine screening
- If cytology ≥ASC or HPV positive → colposcopy
-
Treatment (if CIN 1 persists for at least 2 years):
- Cryotherapy of the cervix
- LEEP (Loop Electrosurgical Excision Procedure)
- Either ablative or excisional methods are acceptable; excision is preferred if colposcopy is unsatisfactory, ECC is positive, or patient was previously treated
Special scenarios:
| Situation | Management |
|---|---|
| CIN 1 preceded by HSIL or AGC-NOS cytology | Review all results; if no change in diagnosis, either observation or diagnostic excisional procedure |
| Adolescents (≤20 years) | Repeat cytology at 12 months (observation preferred; screen typically deferred until age 21) |
| Persistent CIN 1 ≥2 years | Follow-up OR treatment |
| Total hysterectomy (no history of CIN 2/3) | No further screening needed |
Pfenninger & Fowler's Procedures for Primary Care; Swanson's Family Medicine Review
Treatment NOT appropriate: Total hysterectomy is not an acceptable management option for CIN 1. - Swanson's Family Medicine Review
Cytology Context
On Pap smear, CIN 1 corresponds to an LSIL result. The cytology finding of LSIL should prompt referral for colposcopy. Liquid-based cytology allows reflex HPV testing in cases of ASC-US. - Swanson's Family Medicine Review
The cervical biopsy (histology) uses the CIN classification, while cytology uses the Bethesda system (LSIL/HSIL). A biopsy diagnosis of CIN 1 correlates to LSIL. - Tietz Textbook of Laboratory Medicine
Immunohistochemistry Markers
- Ki-67: Marks actively dividing cells; abnormally present in upper epithelium in CIN 1
- p16: Cyclin-dependent kinase inhibitor; overexpressed due to HPV-mediated cell cycle disruption
- Both Ki-67 and p16 are useful for confirming diagnosis in equivocal cases
HPV Vaccine (Prevention)
Gardasil 9 provides immunity against HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58, covering both low-risk (condyloma) and high-risk (dysplasia/cancer) types. Recommended universally for girls aged 11-12 (can be given 9-26 in females, 9-21 in males). - Swanson's Family Medicine Review
What distinguishes CIN 1 from CIN 2 and CIN 3 histologically?
Finding Sources
Finding Sources
The content we need is already in our context from the previous turn. Here is the detailed histological comparison:
Histological Distinctions: CIN 1 vs CIN 2 vs CIN 3
The Core Principle: Depth of Immature Cell Expansion
The single most important grading criterion is how far the layer of immature, undifferentiated (dysplastic) squamous cells extends upward from the basement membrane through the epithelial thickness. In a normal cervix, immature cells are confined to the basal layer only; maturation progresses toward the surface.
Grade-by-Grade Comparison
| Feature | CIN 1 (LSIL) | CIN 2 (HSIL) | CIN 3 (HSIL) |
|---|---|---|---|
| Immature cell layer extent | Lower 1/3 of epithelium | Lower 2/3 of epithelium | Full thickness / upper 2/3 to surface |
| Surface maturation | Preserved in upper 2/3 | Partially preserved | Absent (lost) |
| Koilocytic atypia | Prominent - characteristic feature | Less prominent | Minimal or absent |
| Nuclear atypia | Mild - enlargement, hyperchromasia, coarse chromatin | Moderate - progressive atypia | Severe - diffuse atypia throughout |
| Nuclear-to-cytoplasmic ratio | Mildly increased | Moderately increased | Markedly increased |
| Mitotic figures | Rare, confined to lower 1/3 | Present in lower 2/3 | Numerous, may extend to upper 1/3 or surface; abnormal mitoses may be seen |
| Loss of polarity | Minimal | Moderate | Severe |
| HPV viral replication | High (productive infection) | Intermediate | Low - virus often integrating into host genome |
| p16 overexpression | Present | Diffuse, strong (diagnostic of HSIL) | Diffuse, strong |
| Ki-67 (MIB-1) | Abnormally expressed in upper epithelium | Extends into middle/upper thirds | Throughout full thickness |
From Robbins, Cotran & Kumar Pathologic Basis of Disease
Visual Reference
Fig. 22.14 - Spectrum of CIN. CIN 1 shows koilocytic atypia in the upper layers with preserved maturation. CIN 2 shows expanding basal-type cells. CIN 3 shows near-total loss of differentiation. From Robbins, Cotran & Kumar.
Key Diagnostic Clues in Detail
CIN 1
- The upper 2/3 of the epithelium still matures normally - cells flatten and acquire cytoplasm as they approach the surface
- The hallmark is koilocytic atypia: cells with enlarged, irregular, hyperchromatic nuclei surrounded by a clear perinuclear halo (cytoplasmic vacuole), created by HPV E5 protein acting on the endoplasmic reticulum
- This reflects active, high-level HPV replication in maturing cells
- Viral DNA is episomal (extrachromosomal) - not yet integrated
CIN 2
- Immature atypical cells now occupy the lower two-thirds
- Surface maturation is reduced but not absent
- Koilocytes are less conspicuous
- This is the most reproducibility-challenged grade - interobserver variability is highest at CIN 2, which is why some systems treat it as HSIL and others as a borderline lesion
CIN 3
- Immature cells span full thickness or nearly so - the epithelium looks like a sheet of undifferentiated cells from base to surface
- No surface maturation - cells at the surface resemble basal cells
- Nuclear atypia is severe and diffuse
- Abnormal mitoses (tripolar, multipolar) may be present
- Viral DNA tends to be integrated into the host genome, increasing E6/E7 expression and driving further genomic instability
- The lesion is at highest risk for progression to invasive carcinoma
Why CIN 2 and 3 Were Merged into HSIL
The three-tier CIN classification was simplified to a two-tier system (LSIL / HSIL) because clinical management is binary:
- CIN 1 = observe (high spontaneous regression rate, low cancer risk)
- CIN 2 + CIN 3 = treat (excision or ablation - LEEP, cone biopsy)
CIN 2 and 3 share the same management pathway, and the distinction between them carries limited clinical consequence. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Ancillary IHC Summary
- p16: A surrogate marker for high-risk HPV-mediated RB inactivation. Diffuse block-positivity strongly favors CIN 2/3 (HSIL). Patchy or absent in CIN 1. Used in equivocal cases to separate CIN 1 from CIN 2.
- Ki-67: Marks proliferating cells. In CIN 1, it abnormally appears in the upper epithelial layers (normally confined to the basal layer). Progressively extends upward with higher grades.
The combination of diffuse p16 + Ki-67 extending beyond the lower third is the IHC signature of HSIL and helps resolve diagnostically difficult cases.
What does lower 1/3 means
Great question - this refers to the physical layers of the cervical squamous epithelium when viewed under the microscope.
The Cervical Squamous Epithelium - Divided into Thirds
Imagine the full thickness of the epithelium (from basement membrane at the bottom to the surface at the top) divided into three equal horizontal zones:
SURFACE ────────────────────────────────
│ Upper 1/3 │ mature cells, flat, abundant cytoplasm
├──────────────┤
│ Middle 1/3 │ intermediate cells
├──────────────┤
│ Lower 1/3 │ basal & parabasal cells ← immature, small, high N:C ratio
BASEMENT ────────────────────────────────
MEMBRANE
What "Lower 1/3" Means
The lower 1/3 is the zone immediately above the basement membrane - this is where the basal and parabasal cells normally live.
- These cells are normally immature: small, round, high nuclear-to-cytoplasmic (N:C) ratio, actively dividing
- In a normal cervix, only these basal cells divide; as cells move upward they mature - they flatten, gain cytoplasm, and lose their nuclei near the surface
- This upward maturation is called normal epithelial differentiation
How This Applies to CIN Grading
The question the pathologist asks is: "How far up have the abnormal, immature, undifferentiated cells spread?"
Normal CIN 1 CIN 2 CIN 3
SURFACE ───────────────────────────────────────────────────────
Upper │ mature │ mature │ mature │ ABNORMAL│ ABNORMAL│
1/3 │ cells │ cells │ cells │ cells │ cells │
├─────────┼─────────┼─────────┼─────────┼─────────┤
Middle │ intermed│ intermed│ ABNORMAL│ ABNORMAL│ ABNORMAL│
1/3 │ cells │ cells │ cells │ cells │ cells │
├─────────┼─────────┼─────────┼─────────┼─────────┤
Lower │ basal │ ABNORMAL│ ABNORMAL│ ABNORMAL│ ABNORMAL│
1/3 │ cells │ cells │ cells │ cells │ cells │
BASEMENT ───────────────────────────────────────────────────────
| Grade | Abnormal cells reach... | Surface maturation |
|---|---|---|
| Normal | Stay at very base only | Full maturation to surface |
| CIN 1 | Lower 1/3 only | Upper 2/3 still matures normally |
| CIN 2 | Lower 2/3 | Only upper 1/3 matures |
| CIN 3 | Full thickness | No maturation at all |
Why This Matters
The deeper principle is loss of maturation = loss of differentiation = more malignant potential.
- In CIN 1, most of the epithelium still behaves normally - cells mature and differentiate as they should. The abnormal zone is small and near the base. This is why CIN 1 regresses spontaneously in most cases - the tissue still has strong differentiation signals.
- In CIN 3, the entire epithelium is filled with undifferentiated, rapidly dividing cells that no longer know how to mature. This closely resembles what cancer looks like - and if the basement membrane is breached, it becomes invasive carcinoma.
Think of it as a "takeover" - the more of the epithelium that the abnormal immature cells have colonized, the higher the grade and the greater the risk.
This is a shared conversation. Sign in to Orris to start your own chat.