Radiological Approach to solitary pulmonary nodule by garagier and allison
Reading File
Finding Sources
Finding Sources
Searching the Web
Grainger Allison radiological approach solitary pulmonary nodule
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the content needed. Let me now compose the comprehensive answer based on Grainger & Allison's Diagnostic Radiology.
Radiological Approach to the Solitary Pulmonary Nodule
Source: Grainger & Allison's Diagnostic Radiology (7th ed.), Chapter 8 - Lung Cancer and Pulmonary Nodules
Definition
A solitary pulmonary nodule (SPN) is a single, discrete, rounded opacity in the lung parenchyma that measures up to 3 cm in diameter and is not associated with mediastinal adenopathy, atelectasis, or pleural effusion. Lesions >3 cm are classified as masses and carry a higher probability of malignancy.
Clinical Significance
Nodule detection has become an everyday occurrence with multislice CT. Management presents three possible outcomes:
- No further action required
- CT surveillance
- Further investigation (PET/CT and/or biopsy)
Step 1: Assess Nodule Size and Growth Rate
Nodule size is the dominant parameter guiding management.
| Size | Interpretation |
|---|---|
| <5 mm (or <80 mm³) | Malignancy risk so low that follow-up not generally recommended in average-risk patients |
| 5-8 mm | Intermediate risk - CT surveillance guided by volumetry/VDT |
| >8 mm | Significant risk - further assessment with PET/CT or tissue sampling |
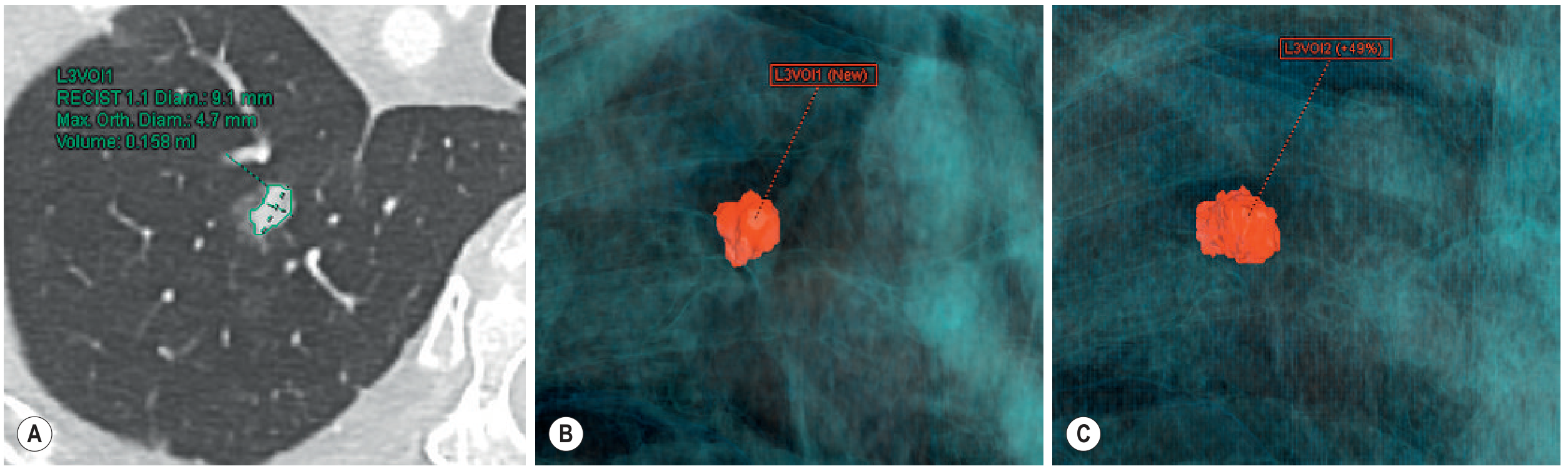
Volume Doubling Time (VDT): The BTS guidelines advocate volumetry to calculate VDT at follow-up. Growing nodules with a VDT <600 days are significantly more likely to be malignant. Some indolent adenocarcinomas (usually subsolid) have considerably prolonged VDTs.
Step 2: Assess Location, Shape, and Morphology
Perifissural Nodules (Benign Features)
These small subpleural nodules frequently represent intrapulmonary lymphoid tissue or intraparenchymal lymph nodes. Characteristic features:
- <15 mm from the pleural surface
- Ellipsoid shape
- Connected to pleura by a fine linear opacity
- Lower lobe predominance
- Follow-up studies from the NELSON Screening Trial confirmed no perifissural nodule developed into lung cancer
Nodule Outline
- Concave surfaces on all sides, or a straight surface of contact with the pleura - benign features
- The less spherical a nodule (low sphericity index on volumetric CT), the less likely a malignant aetiology
- Flat or tubular nodules are more likely to be benign
- Solid, subpleural, polygonal nodules with low sphericity = highly unlikely to be malignant
- Spiculation ("corona radiata") - irregular spiculated margins are associated with malignancy
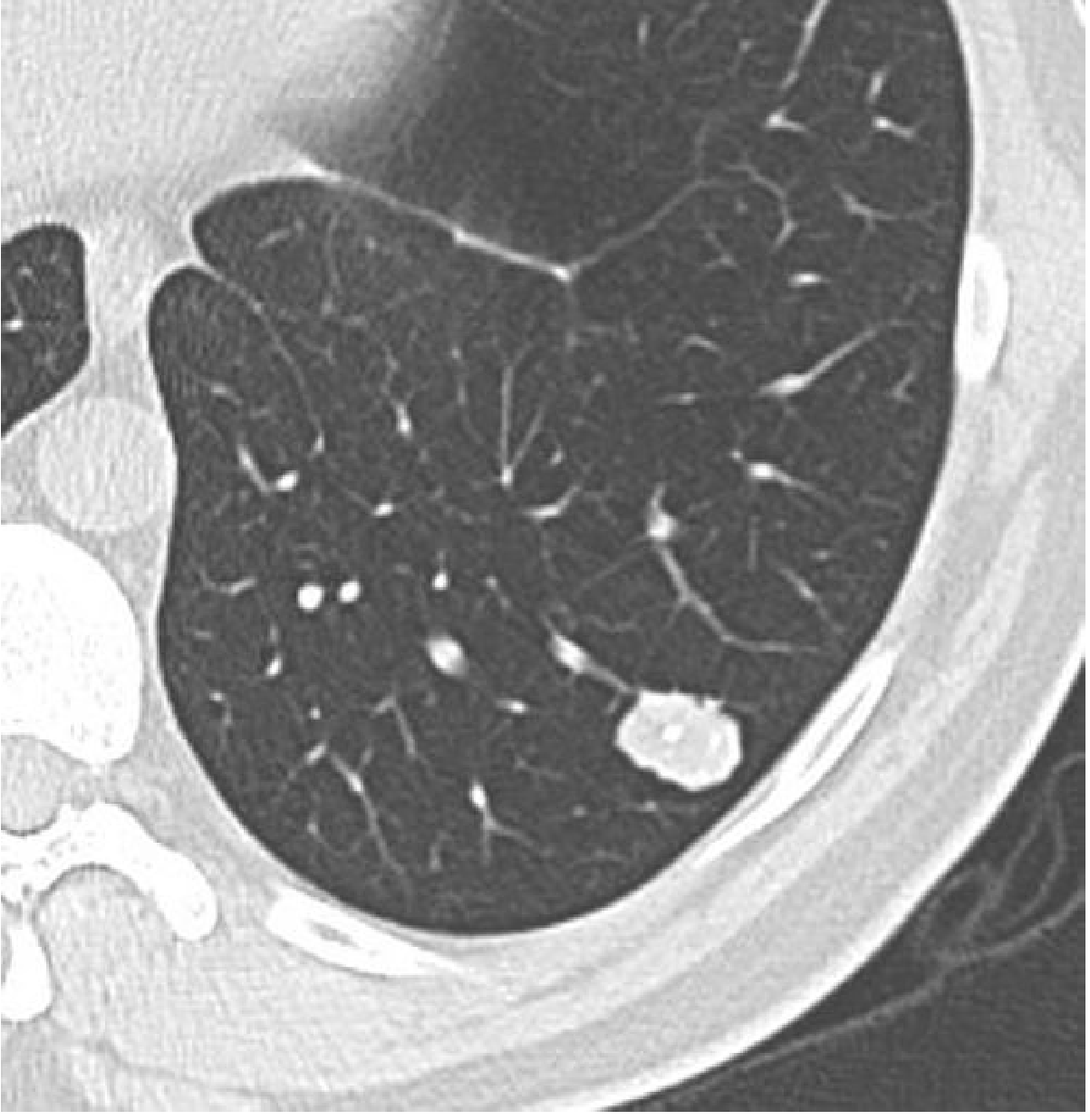
Step 3: Assess Calcification Pattern
Calcification pattern is one of the most reliable CT features for benign versus malignant assessment.
Benign Patterns (specific enough to preclude further evaluation):
- Central (bull's eye) - granuloma
- Diffuse/homogeneous - old granuloma
- Laminated/concentric rings - granuloma
- Popcorn calcification - hamartoma (cartilaginous nodule)
Malignant / Indeterminate Patterns:
- Eccentric / amorphous calcification within soft-tissue density - may be seen in malignancy (dystrophic calcification within a tumour)
- Note: metastases from bone-forming or cartilage-forming tumours may occasionally show benign-appearing calcification
Step 4: Classify as Solid vs. Subsolid
Subsolid Nodules
| Type | Definition | CT Appearance | Histological Correlate |
|---|---|---|---|
| Pure Ground-Glass Nodule (GGN) | Focal increased attenuation, lung architecture visible | Hazy, no solid component | Atypical adenomatous hyperplasia, adenocarcinoma in situ |
| Part-Solid Nodule | GGN with a central solid component that obscures architecture | Mixed density | Minimally invasive adenocarcinoma, invasive adenocarcinoma |
The Fleischner Society and BTS have published dedicated guidelines for subsolid nodules, recognising they may represent early forms of adenocarcinoma.
New adenocarcinoma classification (replacing bronchoalveolar carcinoma):
- Pre-malignant: Atypical adenomatous hyperplasia + adenocarcinoma in situ - appear as pure GGN, ≤1 cm, pure lepidic growth, no solid components. Small GGNs (<5-6 mm) do not require surveillance.
- Minimally invasive adenocarcinoma (MIA): Predominantly lepidic growth, ≤3 cm, invasive component ≤5 mm, generally subsolid with solid component usually <5 mm. May grow slowly.
- Invasive adenocarcinoma: Solid component >5 mm.
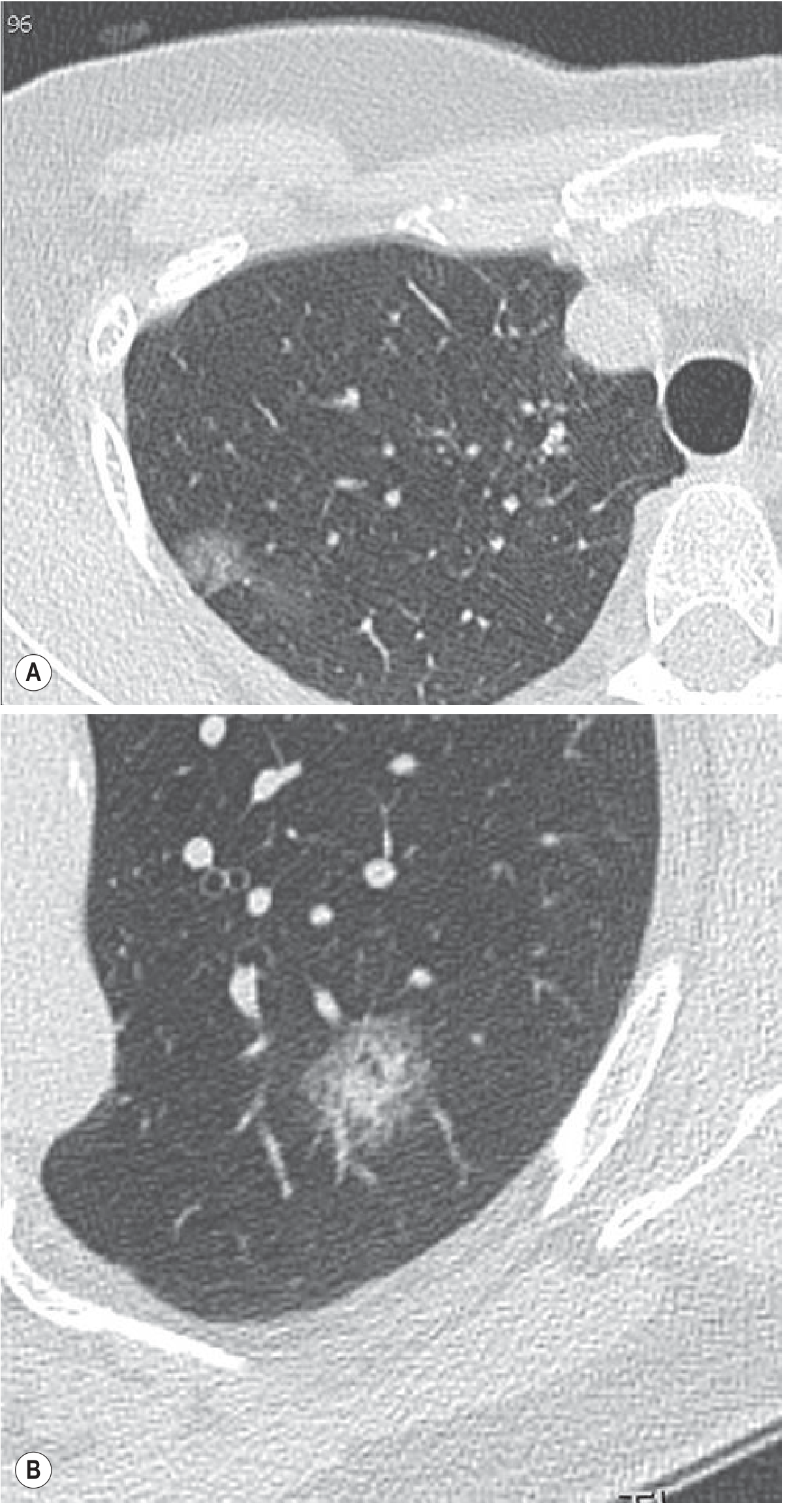
The solid component of a part-solid nodule is the invasive portion and drives management. A part-solid nodule that started as a pure GGN and develops a solid centre (Fig. 8.5B) requires prompt evaluation.
Step 5: Risk Stratification and Management Algorithms
Fleischner Society 2017 vs. BTS 2015 Guidelines
| Parameter | Fleischner 2017 | BTS 2015 |
|---|---|---|
| Population | Age ≥35, incidentally detected | Age ≥18, all presentations |
| Sizing method | Mean diameter (long + short axis) | Volumetry preferred |
| Follow-up threshold | 6 mm | 80 mm² (or 5 mm) |
| Growth definition | ≥2 mm diameter increase | >25% volume increase |
| Small nodule (<6 mm) | No follow-up in low risk | Discharge; follow if definitely new vs. prior 1-2y CT |
| Medium nodule (6-8 mm) | CT at 6-12 months, then 18-24 months | CT at 3 months; further follow-up based on VDT |
| Large nodule (>8 mm) | CT at 3 months, PET/CT or biopsy | Brock model risk estimation |
BTS Brock Model (>8 mm nodules)
- Brock model risk <10%: CT surveillance
- Brock model risk 10-70%: Consider image-guided biopsy, excision, or surveillance; further risk stratification with Herder model (incorporating FDG-PET result)
- Herder score <10%: CT surveillance
- Herder score 10-70%: Image-guided biopsy, excision, or surveillance
- Herder score >70%: Consider definitive treatment (resection)
Step 6: Advanced Imaging Modalities
FDG-PET / PET-CT
- Indicated for solid nodules >8 mm that cannot be resolved by CT morphology alone
- Sensitivity: 82-97%, Specificity: 78-82% for malignancy
- False positives: Active granulomas (TB, sarcoidosis, aspergillosis)
- False negatives: Hyperglycaemia; low metabolic tumours (carcinoid, BAC/lepidic adenocarcinoma); nodules <8 mm in diameter
- Integrated PET/CT provides anatomical and functional assessment
CT Enhancement
- Nodule enhancement >15 HU after contrast suggests increased vascularity (malignancy)
- Limited specificity; largely superseded by PET-CT
MRI
- Limited role in nodule characterisation; useful in selected cases
Step 7: Tissue Sampling
Once imaging favours malignancy, tissue diagnosis is required:
- CT-guided percutaneous biopsy - for peripherally located nodules accessible to needle
- Bronchoscopy / EBUS - for centrally located or hilar lesions
- VATS / surgical resection - if non-diagnostic biopsy or high surgical fitness and high malignancy probability
Summary: Radiological Features Favouring Benign vs. Malignant
| Feature | Favours Benign | Favours Malignant |
|---|---|---|
| Size | <5 mm | >8 mm |
| Shape | Polygonal, flat, tubular, low sphericity | Round, spherical |
| Margins | Smooth, well-defined, concave surfaces | Spiculated (corona radiata), lobulated |
| Location | Subpleural, perifissural, lower lobe | Upper lobe (especially right) |
| Calcification | Central, diffuse, laminated, popcorn | Absent, eccentric, amorphous |
| Density | Solid with fat density (hamartoma) | Part-solid (solid component >5mm) |
| VDT | >600 days or stable >2 years | <400 days |
| FDG-PET | No uptake | Uptake > mediastinal blood pool |
| CT enhancement | <15 HU | >15 HU |
Source: Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging (ISBN 9780323760751), Chapter 8, pp. 184-208. Supplementary content from Harrison's Principles of Internal Medicine and pulmonology references.
This is a shared conversation. Sign in to Orris to start your own chat.