Part A: Vision 142. Functional Anatomy of Eye 1165 143. Image-forming Mechanism 1172 144. Photoreceptor Mechanism 1177 145. Visual Pathway and Visual Cortex 1181 146. Visual Acuity, Visual Field, Light and Dark Adaptations, and Visual Reflexes 1188 147. Color Vision 1193 148. Movements of the Eye Include pictures of pathways and give clinical co relation all the drugs and treatment of it give pictures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching the Web
visual pathway lesions clinical correlations drugs treatment glaucoma optic neuritis
Reading File
Reading File
Searching the Web
drugs for glaucoma color blindness macular degeneration eye movement disorders treatment 2024
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Reading File
Searching the Web
anti-VEGF treatment wet macular degeneration ranibizumab bevacizumab aflibercept 2024 guidelines
Loading Image
Finding Sources
Here is a thorough, integrated guide covering all seven vision chapters with pathway diagrams, clinical correlations, and drugs/treatments.
Part A: Vision - Complete Guide (Chapters 142-148)
Chapter 142 - Functional Anatomy of the Eye
Coats of the Eye
- Sclera: tough outer protective coat; continuous anteriorly with the cornea
- Cornea: transparent avascular tissue; provides ~40 diopters (2/3) of total refractive power
- Choroid: vascular, pigmented middle coat providing nutrition to outer retinal layers
- Retina: innermost coat; contains photoreceptors (rods and cones)
Refractive Media (in order)
Cornea → Aqueous humor → Lens → Vitreous humor
- Total refractive power of the eye = 59 diopters (accommodated for distance)
- Cornea contributes ~40 D; Lens contributes ~20 D in resting state
Lens and Accommodation
The lens is elastic, suspended by 70 suspensory ligaments from the ciliary muscle.
- For near vision: Ciliary muscle contracts (both meridional and circular fibers) → ligaments relax → lens becomes more spherical (more convex) → greater refractive power (up to 34 D in children)
- For distant vision: Ciliary muscle relaxes → ligaments taut → lens flattened
- Range of accommodation in children: up to 14 diopters; progressively lost with age (presbyopia)
Retinal Layers (inside to out)
- Internal limiting membrane
- Nerve fiber layer (ganglion cell axons)
- Ganglion cell layer - only output neurons of the retina
- Inner plexiform layer
- Inner nuclear layer (bipolar, horizontal, amacrine cells)
- Outer plexiform layer
- Outer nuclear layer (rod and cone nuclei)
- Photoreceptor layer (outer segments of rods and cones)
- Retinal pigment epithelium (RPE)
Fovea and Macula
- Fovea centralis: ~0.5 mm diameter; contains only cones (no rods, no overlying cells)
- This is the point of maximum visual acuity
- The optic disc (blind spot) contains no photoreceptors; located ~15° nasal to the fovea
Clinical Correlations - Anatomy
| Condition | Anatomical Basis | Key Feature |
|---|---|---|
| Myopia (nearsightedness) | Eyeball too long; image focused in front of retina | Corrected with concave (diverging) lens |
| Hyperopia (farsightedness) | Eyeball too short; image focused behind retina | Corrected with convex (converging) lens |
| Astigmatism | Non-uniform corneal curvature | Corrected with cylindrical lenses |
| Presbyopia | Loss of lens elasticity with age | Reading glasses (convex lenses) |
| Cataract | Opacity of lens | Surgical removal + intraocular lens implant |
| Glaucoma | Raised IOP → optic nerve damage | See drug table below |
| Detached retina | Separation of retina from RPE | Laser photocoagulation, vitrectomy |
Drugs for Refractive Errors / Lens Disorders
- Cataract surgery (IOL): No pharmacological correction; post-op topical antibiotics (moxifloxacin), NSAIDs (ketorolac), steroids (prednisolone acetate)
- Cycloplegics (for refraction testing): Atropine, cyclopentolate, tropicamide (block muscarinic receptors → ciliary muscle paralysis)
- Mydriatics (pupil dilation): Phenylephrine (alpha-1 agonist), tropicamide
Chapter 143 - Image-Forming Mechanism
Optics of the Eye
- Light refracted at anterior corneal surface (main site) and at lens surfaces
- The "reduced eye" model: single refractive surface 17 mm in front of retina, 59 D total power
- Image formed on retina is inverted and reversed - the brain learns to interpret this as upright
Pupillary Light Reflex (regulates image quality)
- Smaller pupil → greater depth of focus, sharper image, but less light
- Pathway: Light → Retina → Optic nerve → Pretectal nucleus (midbrain) → Edinger-Westphal nucleus → Ciliary ganglion → Sphincter pupillae (constriction via muscarinic M3 receptors)
Accommodation Reflex (near triad)
Three simultaneous events:
- Lens becomes more convex (ciliary muscle contraction)
- Pupil constricts (increases depth of focus)
- Eyes converge (medial recti contract) All three driven by parasympathetic (Edinger-Westphal nucleus) and the frontal eye fields
Clinical Correlations - Image Formation
| Sign/Condition | Basis | Clinical Significance |
|---|---|---|
| Argyll Robertson pupil | Pretectal lesion (syphilis) | Light reflex lost; accommodation preserved ("prostitute's pupil") |
| Horner syndrome | Sympathetic chain interruption | Miosis, ptosis, anhidrosis - pupil doesn't dilate well |
| Adie's tonic pupil | Ciliary ganglion damage | Dilated pupil, slow light response; near reflex preserved |
| RAPD (Marcus Gunn pupil) | Optic nerve lesion | Afferent limb defect; swinging flashlight test positive |
| Pilocarpine test | Dilute pilocarpine (0.1%) constricts Adie's (supersensitivity) | Differentiates from 3rd nerve palsy |
Drugs Acting on Pupil
| Drug | Mechanism | Use |
|---|---|---|
| Pilocarpine | Muscarinic agonist | Constricts pupil; used in glaucoma and Adie's pupil testing |
| Physostigmine | AChE inhibitor | Indirect muscarinic stimulation; miosis |
| Atropine | Muscarinic antagonist | Mydriasis, cycloplegia |
| Phenylephrine | Alpha-1 agonist | Mydriasis (no cycloplegia) |
| Cocaine | Blocks norepinephrine reuptake | Dilates normal pupil; no dilation in Horner's (confirms diagnosis) |
| Apraclonidine | Alpha-2 agonist | Reversal of anisocoria in Horner's (pharmacodiagnosis) |
Chapter 144 - Photoreceptor Mechanism
Rods vs Cones
| Feature | Rods | Cones |
|---|---|---|
| Number | ~120 million | ~6 million |
| Location | Peripheral retina | Concentrated in fovea |
| Vision type | Scotopic (dim light) | Photopic (bright light, color) |
| Sensitivity | Very high | Lower |
| Acuity | Low | High |
| Adaptation | Slow, large range | Fast, smaller range |
| Photopigment | Rhodopsin | Red (L), Green (M), Blue (S) opsins |
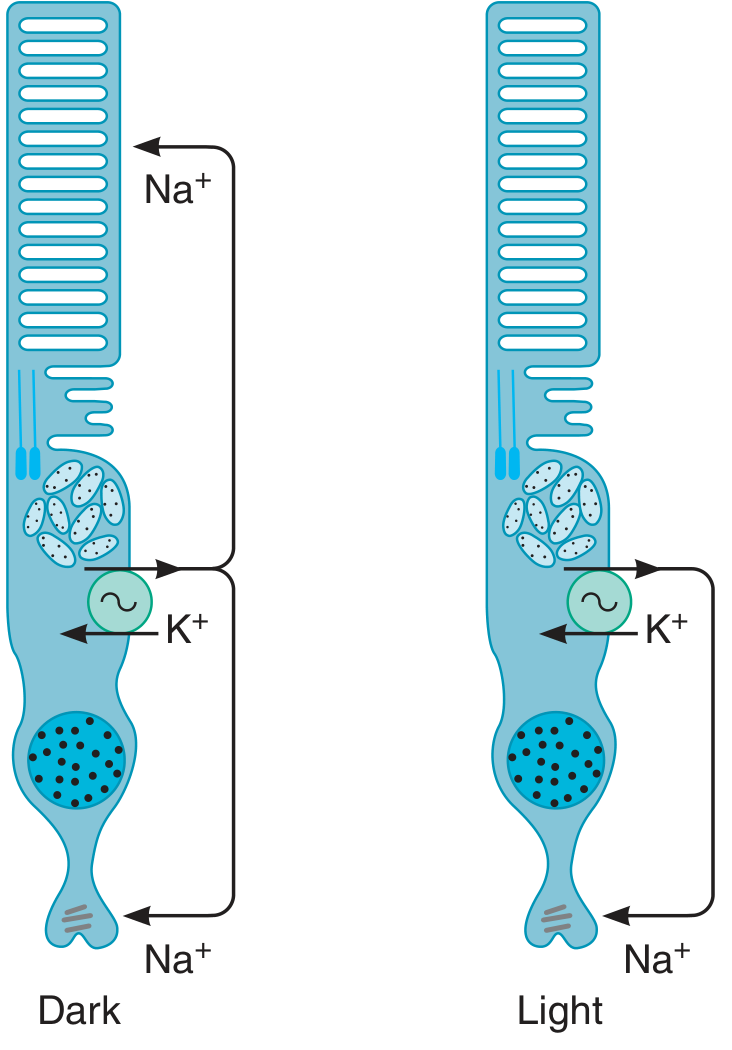
Phototransduction Cascade (Rods)
In the dark:
- High cGMP → cGMP-gated Na⁺ channels open → Na⁺ influx (dark current) → depolarized state → continuous glutamate release
When light hits:
- 11-cis retinal → all-trans retinal (structural change in rhodopsin)
- Rhodopsin activates Transducin (G protein)
- Transducin activates phosphodiesterase (PDE)
- PDE breaks down cGMP → decreased cGMP
- cGMP-gated Na⁺ channels close
- Cell hyperpolarizes (unique - opposite of other sensory receptors)
- Glutamate release decreases
- Signal transmitted to bipolar cells → ganglion cells → optic nerve
Rhodopsin Regeneration
- Rhodopsin = scotopsin + 11-cis retinal (derived from Vitamin A)
- After bleaching: all-trans retinal → (retinal isomerase) → 11-cis retinal → recombines with scotopsin
- Alternative: all-trans retinal → all-trans retinol (Vitamin A) → 11-cis retinol → 11-cis retinal
Retinal Cell Responses to Light
- Rods, Cones, Horizontal cells: Hyperpolarize (graded potentials)
- Bipolar cells: Either hyperpolarize or depolarize (graded)
- Amacrine cells: Depolarize, generate spikes
- Ganglion cells: Only cells generating action potentials (propagated spikes)
Clinical Correlations - Photoreceptors
| Condition | Mechanism | Treatment |
|---|---|---|
| Night blindness (Nyctalopia) | Vitamin A deficiency → insufficient rhodopsin | Vitamin A supplementation (oral or IV); IV reversal within 1 hour |
| Age-related macular degeneration (AMD) | Degeneration of macular RPE and photoreceptors | Anti-VEGF injections (wet AMD); AREDS2 supplements (dry AMD) |
| Retinitis pigmentosa | Progressive rod death (genetic) | Vitamin A palmitate (slows progression); gene therapy (Luxturna for RPE65 mutations) |
| Leber congenital amaurosis | RPE65 mutation → no 11-cis retinal regeneration | Voretigene neparvovec (Luxturna) - FDA approved gene therapy |
Key Drugs
- Vitamin A (retinol): Essential for rhodopsin synthesis; deficiency → night blindness → xerophthalmia → blindness
- Sildenafil (Viagra): Inhibits retinal PDE (same enzyme as penile PDE-5) → transient blue-green color weakness (side effect)
- Anti-VEGF agents (wet AMD): Ranibizumab (Lucentis), Bevacizumab (Avastin, off-label), Aflibercept (Eylea), Brolucizumab, Faricimab - intravitreal injection
- AREDS2 formula (dry AMD): Vitamin C, Vitamin E, Lutein, Zeaxanthin, Zinc, Copper
- Luxturna (voretigene neparvovec): First FDA-approved gene therapy for inherited retinal dystrophy due to RPE65 mutations
Chapter 145 - Visual Pathway and Visual Cortex
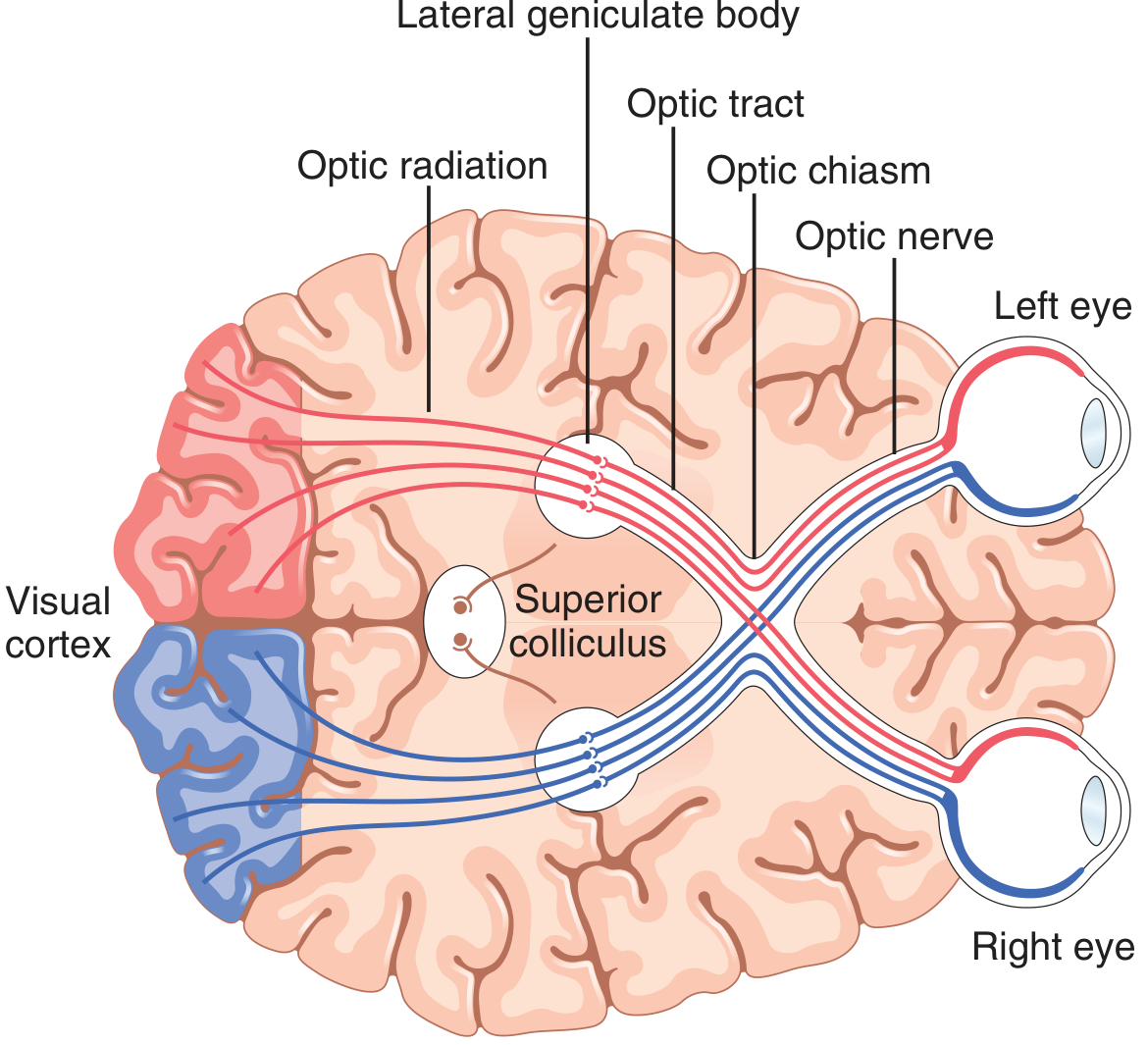
Complete Visual Pathway
Retina (photoreceptors → bipolar cells → ganglion cells)
↓
Optic nerve (CN II)
↓
Optic chiasm [nasal fibers CROSS; temporal fibers stay ipsilateral]
↓
Optic tract
↓
Lateral Geniculate Nucleus (LGN) of Thalamus
↓
Optic radiation (Geniculocalcarine tract)
↓
Primary Visual Cortex (V1) - calcarine fissure, occipital lobe (Area 17)
Key Anatomical Details
Optic Chiasm:
- Nasal retinal fibers (serving temporal visual fields) decussate
- Temporal retinal fibers (serving nasal visual fields) remain ipsilateral
- Therefore: Right optic tract = left half of both retinas = left visual field
Lateral Geniculate Nucleus (LGN) - 6 Layers:
- Layers I, IV, VI: crossed fibers (contralateral nasal retina)
- Layers II, III, V: uncrossed fibers (ipsilateral temporal retina)
- Signals from the two eyes remain segregated in LGN
- Magnocellular layers (1-2): movement, depth, flicker (M pathway)
- Parvocellular layers (3-6): color, texture, fine detail, shape (P pathway)
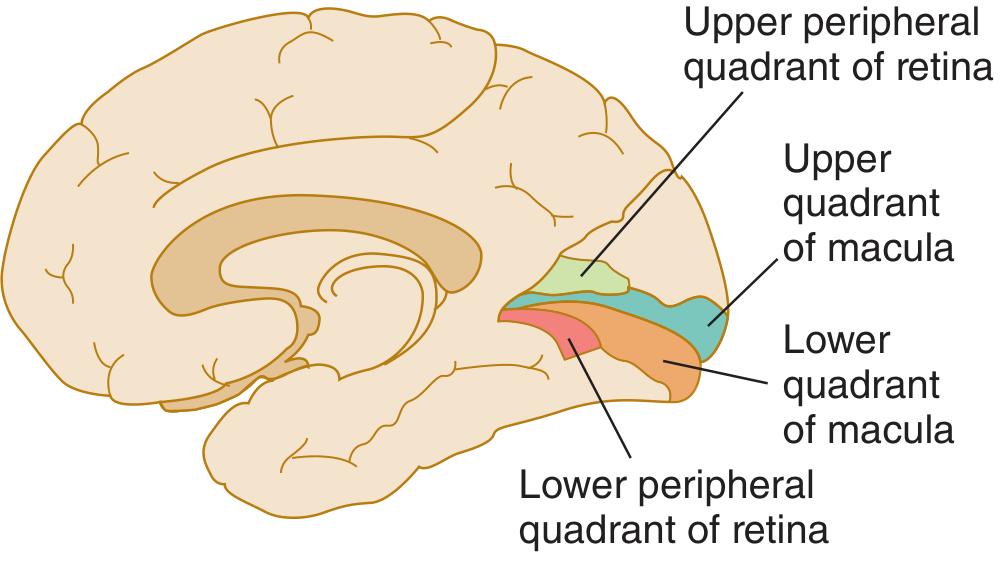
Optic Radiations:
- Upper fibers (from lower visual field) → superior lip of calcarine fissure
- Lower fibers (Meyer's loop, temporal lobe) → inferior lip of calcarine fissure
- Macular representation is largest and most posterior
Visual Cortex Areas:
- V1 (Area 17, striate cortex): Primary visual cortex in calcarine fissure
- V2 (Area 18): Secondary visual processing
- V4: Color processing
- V5/MT: Motion processing
- Dorsal pathway (parietal, "where"): Motion, spatial processing
- Ventral pathway (temporal, "what"): Object recognition, faces, color
Other Visual Projections (non-geniculostriate "old system"):
- Suprachiasmatic nucleus (hypothalamus) - circadian rhythm entrainment
- Pretectal nuclei (midbrain) - pupillary light reflex, focus
- Superior colliculus - rapid saccadic eye movements
- Ventral thalamus/basal regions - behavioral responses
Visual Field Defects - Clinical Correlation (MOST IMPORTANT)
| Site of Lesion | Visual Field Defect | Common Cause |
|---|---|---|
| Optic nerve (1 eye) | Unilateral blindness; RAPD present | Optic neuritis (MS), ischemic optic neuropathy, glaucoma |
| Optic chiasm (central) | Bitemporal hemianopia | Pituitary adenoma, craniopharyngioma |
| Optic chiasm (lateral) | Binasal hemianopia | Bilateral carotid aneurysms |
| Optic tract | Contralateral incongruous homonymous hemianopia | Trauma, tumor |
| Meyer's loop (temporal) | "Pie in the sky" - upper contralateral quadrantanopia | Temporal lobectomy |
| Parietal lobe radiation | Lower contralateral quadrantanopia | Parietal tumor/stroke |
| Occipital cortex (unilateral) | Congruent contralateral homonymous hemianopia with macular sparing | PCA stroke |
| Occipital cortex (bilateral) | Cortical blindness (pupils normal!) | Bilateral PCA infarction |
Key rule: Lesions before chiasm = monocular; lesions at or after chiasm = binocular (homonymous)
Macular sparing occurs with occipital cortex lesions because the macula has dual blood supply (PCA + MCA) and very large cortical representation.
Drugs/Treatment for Visual Pathway Disorders
Optic Neuritis:
- IV Methylprednisolone 1g/day x 3 days (hastens recovery, doesn't change final outcome)
- Then oral prednisone taper
- For NMOSD (NMO spectrum disorder): Eculizumab, Inebilizumab, Satralizumab, Ravulizumab (FDA-approved)
- Long-term immunosuppression: Azathioprine, Mycophenolate mofetil, Rituximab
Ischemic Optic Neuropathy (AION):
- NAION (non-arteritic): Aspirin; risk factor control
- AAION (arteritic, GCA): High-dose oral prednisone immediately (60-80 mg/day); may need IV methylprednisolone
Chapter 146 - Visual Acuity, Visual Field, Light & Dark Adaptation, and Visual Reflexes
Visual Acuity
- Defined as the minimum angle of separation between two point sources that can be distinguished
- Normal: 25 seconds of arc (minimum resolvable angle); 20/20 Snellen chart at 20 feet
- Determined by cone density in the fovea (cone diameter ~1.5 µm; minimum spacing ~2 µm)
- 20/200 vision = "legal blindness" in the USA
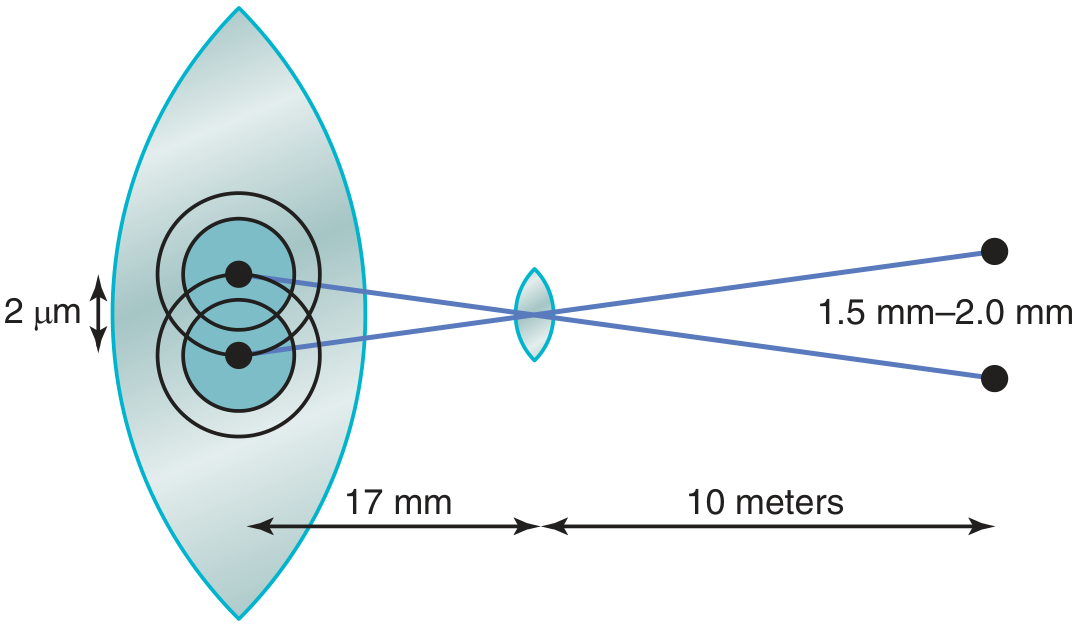
Snellen Notation: Fraction - numerator = test distance (20 ft); denominator = distance at which a normal eye can read that letter size
Visual Field Testing
- Confrontation test: Bedside screening
- Goldmann perimetry: Manual kinetic perimetry (good for peripheral fields)
- Humphrey automated perimetry: Standard for glaucoma monitoring
- Amsler grid: Tests central 10° field; detects macular distortion (metamorphopsia)
Light and Dark Adaptation
Dark adaptation (entering a dark room after bright light):
- First 5-10 min: cone adaptation (faster, less sensitive)
- After 20-40 min: rod adaptation (slower, increases sensitivity ~25,000-fold)
- This bi-phasic "dark adaptation curve" is a classic exam feature
- Overall sensitivity change: 500,000 to 1 million-fold between full light and dark adaptation
Mechanisms of adaptation:
- Photochemical: Rhodopsin regeneration (main mechanism, slow - minutes to hours)
- Pupillary changes: ~30-fold, very fast (fraction of a second)
- Neural adaptation: Only a few-fold, but rapid (seconds)
Light adaptation (entering bright light from darkness):
- Rhodopsin bleaches → rods saturate → cones take over
- Initial visual bleaching (temporary blindness) → adapts within minutes
Visual Reflexes
Pupillary Light Reflex:
- Afferent: CN II → pretectal nucleus (midbrain)
- Efferent: Edinger-Westphal nucleus → CN III → ciliary ganglion → sphincter pupillae
- Both direct (same eye) and consensual (opposite eye) responses occur
- Absent in optic nerve lesion (no consensual in affected eye); preserved if lesion is cortical
Accommodation-Convergence Reflex:
- Blur on retina → frontal cortex → Edinger-Westphal → ciliary muscle + pupil constriction + medial rectus convergence
Clinical Correlations
| Condition | Defect | Cause |
|---|---|---|
| Night blindness | Impaired dark adaptation (rod dysfunction) | Vitamin A deficiency, retinitis pigmentosa |
| Metamorphopsia | Distorted central vision on Amsler grid | Macular degeneration, epiretinal membrane |
| Glare sensitivity | Impaired light adaptation | Cataract |
Drugs for Visual Acuity Disorders
- See glaucoma table in Chapter 147 for IOP management
- Anti-VEGF for AMD (as above)
- Brinzolamide/Dorzolamide: Topical CAIs for ocular hypertension
Chapter 147 - Color Vision
Trichromatic Theory (Young-Helmholtz)
Three types of cones with peak sensitivity:
- L-cones (Red): peak ~560 nm (wavelength 647-723 nm)
- M-cones (Green): peak ~530 nm (wavelength 492-575 nm)
- S-cones (Blue): peak ~420 nm (wavelength 450-492 nm)
Color perception = relative frequency of impulses from each cone type. All colors (and even extraspectral purple) can be produced by mixing red, green, and blue (primary colors).
Opponent-Color Theory (Hering): Further processing occurs where:
- Red-Green opponent cells subtract one input from another
- Blue-Yellow opponent cells
- This occurs at ganglion cell level and LGN
Color Vision Processing in Cortex
- P-cells (parvocellular) → LGN layers 3-6 → V1 layer 4 → "Blobs" in V1 layers 2-3 → V4 (color processing area)
- Lesion of V4 → Achromatopsia (cerebral color blindness, color looks grey)
- V8 area: specifically concerned with color vision in humans; lesion → achromatopsia
Color Blindness
| Type | Defect | Genetics | Prevalence |
|---|---|---|---|
| Protanopia | Red cone absent | X-linked recessive | ~1% males |
| Deuteranopia | Green cone absent | X-linked recessive | ~1% males |
| Tritanopia | Blue cone absent | Autosomal; no sex predilection | Rare |
| Anomalous trichromacy | Shifted pigment sensitivity | X-linked | ~6% males (most common) |
| Achromatopsia | All cone function lost or V4 lesion | Autosomal recessive or cortical | Rare |
Total color blindness: Males 8%, Females 0.4% (X-linked)
- X-linked color blindness skips generations and appears in males of every second generation
Testing:
- Ishihara plates: Colored spot figures on similar-colored background; screens red-green defects
- Farnsworth-Munsell 100 hue test: Quantitative, detects all types
- Anomaloscope: Gold standard for type/severity
Clinical / Drug Correlations - Color Vision
| Drug/Condition | Color Effect | Mechanism |
|---|---|---|
| Sildenafil (Viagra), tadalafil | Transient blue-green weakness | Inhibit retinal PDE (same as PDE-5) |
| Digoxin toxicity | Xanthopsia (yellow-green halos) | Cone toxicity |
| Ethambutol toxicity | Red-green color loss; optic neuritis | Toxic optic neuropathy |
| Chloroquine/hydroxychloroquine | Bull's-eye maculopathy, color loss | Binds melanin in RPE, toxic to cones |
| Amiodarone | Corneal microdeposits; color halos | Lipid deposits in cornea |
| Methanol poisoning | Sudden visual loss, color defects | Formate toxicity to optic nerve |
No pharmacological treatment exists for inherited color blindness. Enchroma glasses (chromatic filters) partially enhance color contrast in some anomalous trichromats.
Chapter 148 - Movements of the Eye
Types of Eye Movements
| Type | Function | Neural Control |
|---|---|---|
| Saccades | Rapid, conjugate, voluntary/reflexive jumps | Frontal Eye Fields (FEF), Superior Colliculus |
| Smooth Pursuit | Following a moving target | Occipital/parietal cortex (MT area) |
| Vergence | Convergence/divergence for depth | Midbrain (near reflex center) |
| Vestibulo-ocular reflex (VOR) | Stabilize image during head movement | Vestibular nuclei, cerebellum |
| Optokinetic reflex | Stabilize image during sustained motion | Brainstem, cerebellum |
| Fixation | Maintain gaze on stationary target | Frontal eye fields |
Neural Control of Eye Movements
Extraocular Muscles and their Nerves:
- CN III (Oculomotor): Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae
- CN IV (Trochlear): Superior oblique
- CN VI (Abducens): Lateral rectus
Horizontal Gaze Control:
- Frontal Eye Field (FEF) → Pontine Paramedian Reticular Formation (PPRF) → ipsilateral CN VI nucleus → lateral rectus (ipsilateral) AND via MLF → contralateral CN III nucleus → medial rectus
- PPRF = horizontal gaze center
Vertical Gaze Control:
- RiMLf (Rostral Interstitial Nucleus of MLF) - vertical gaze center in midbrain
- Also Interstitial Nucleus of Cajal
Internuclear Pathway:
- Medial Longitudinal Fasciculus (MLF): connects CN VI and CN III nuclei for conjugate horizontal gaze
Clinical Correlations - Eye Movements
| Lesion | Deficit | Cause |
|---|---|---|
| CN III palsy | "Down and out" eye, ptosis, fixed dilated pupil | Posterior communicating artery aneurysm (pupil-involving = surgical emergency!) |
| CN IV palsy | Vertical diplopia, head tilt | Trochlear nerve damage (closed head injury) |
| CN VI palsy | Failure of abduction; medial deviation | Raised ICP (false localizing sign), pontine lesion |
| MLF lesion (INO) | Internuclear ophthalmoplegia: ipsilateral adduction failure + contralateral nystagmus | MS (bilateral INO pathognomonic of MS) |
| PPRF lesion | Horizontal gaze palsy ipsilateral | Pontine stroke |
| FEF lesion | Gaze deviation TOWARD lesion (ipsilateral) | Stroke |
| Parinaud syndrome | Loss of upward gaze, convergence-retraction nystagmus, light-near dissociation | Pineal tumor, dorsal midbrain compression |
| Nystagmus | Repetitive involuntary eye oscillation | Vestibular disorders, cerebellar disease, drug toxicity |
Drugs Affecting Eye Movements
| Drug | Eye Movement Effect |
|---|---|
| Aminoglycosides (gentamicin) | Vestibulotoxicity → loss of VOR, oscillopsia |
| Phenytoin | Nystagmus (horizontal gaze-evoked) at toxic levels |
| Carbamazepine | Nystagmus, diplopia |
| Vigabatrin | Visual field constriction, eye movement disorder |
| Barbiturates/benzodiazepines | Nystagmus (horizontal) |
| Metronidazole (high dose) | Cerebellar toxicity → nystagmus |
| Botulinum toxin | Used therapeutically for strabismus, blepharospasm; blocks ACh at NMJ |
| Baclofen | May reduce periodic alternating nystagmus |
| Memantine | Treatment of acquired nystagmus (pendular type) |
| 4-aminopyridine | Downbeat nystagmus treatment (K⁺ channel blocker) |
Master Drug Table for All Eye Disorders
Glaucoma (Most Tested Pharmacology)
| Drug Class | Examples | Mechanism | IOP Effect |
|---|---|---|---|
| Prostaglandin analogs (1st line) | Latanoprost, bimatoprost, travoprost, tafluprost | Increase uveoscleral outflow | ↓↓↓ |
| Beta-blockers | Timolol, betaxolol, levobunolol | Decrease aqueous secretion | ↓↓ |
| Alpha-2 agonists | Brimonidine, apraclonidine | Decrease secretion + increase outflow | ↓↓ |
| Carbonic anhydrase inhibitors | Dorzolamide, brinzolamide (topical); Acetazolamide, methazolamide (oral) | Decrease aqueous secretion | ↓↓ |
| Cholinomimetics | Pilocarpine, carbachol | Ciliary muscle contraction → open trabecular meshwork | ↓ (older agents) |
| Rho kinase inhibitors | Netarsudil | Increase trabecular outflow | ↓ |
| Acute angle-closure (emergency) | Pilocarpine + acetazolamide + mannitol IV | Constrict pupil, reduce aqueous, osmotic dehydration | ↓↓↓ |
New 2024-2026 Developments:
- iDose TR implant: Sustained-release travoprost implant; continuous drug delivery for ~3 years
- Durysta: Bimatoprost intracameral implant lasting ~30 months
- SLT (Selective Laser Trabeculoplasty): Now considered first-line in some guidelines; 2024 studies show slight superiority over drops for visual field preservation
- MIGS (Minimally Invasive Glaucoma Surgery): iStent, Hydrus microstent
Wet AMD
| Drug | Type | Route |
|---|---|---|
| Ranibizumab (Lucentis) | Anti-VEGF-A Fab | Intravitreal injection |
| Bevacizumab (Avastin) | Anti-VEGF-A (off-label) | Intravitreal injection |
| Aflibercept (Eylea) | VEGF trap (VEGF-A + VEGF-B + PlGF) | Intravitreal injection |
| Brolucizumab (Beovu) | Anti-VEGF-A scFv | Intravitreal injection |
| Faricimab (Vabysmo) | Anti-VEGF-A + anti-Ang-2 bispecific | Intravitreal injection |
| Pegcetacoplan (Syfovre) | Complement C3 inhibitor | For geographic atrophy (dry AMD) |
| Avacincaptad pegol (Izervay) | Complement C5 inhibitor | For geographic atrophy |
Summary of All Treatment Targets
Photoreceptor defects → Vitamin A, gene therapy (Luxturna)
Intraocular pressure ↑ → Prostaglandins, β-blockers, CAIs, cholinomimetics
Wet AMD (new vessels) → Anti-VEGF injections
Dry AMD (geographic atrophy) → Complement inhibitors (C3/C5)
Optic neuritis (MS/NMOSD) → IV Methylprednisolone; biologic immunotherapy
Giant cell arteritis → High-dose steroids (immediate)
Color vision drug toxicity → Withdraw offending drug (ethambutol, chloroquine)
Eye movement disorders → Botulinum toxin (strabismus); memantine/4-AP (nystagmus)
Pupillary disorders → Pilocarpine, atropine, phenylephrine (diagnostic/therapeutic)
Quick Clinical Summary - Visual Field Defects at a Glance
Left Eye Right Eye
___ ___
| | 1. ON → Blind one eye (monocular)
|___|
CHIASM → Bitemporal hemianopia (nasal fibers cross)
⊗ ⊗
LEFT OPTIC TRACT → Right homonymous hemianopia
_ ▓ ▓ _
MEYER'S LOOP (temporal) → Upper right quadrantanopia ("pie in sky")
PARIETAL RADIATION → Lower right quadrantanopia
OCCIPITAL CORTEX → Congruent right homonymous hemianopia + MACULAR SPARING
Sources: Guyton & Hall Textbook of Medical Physiology, 14th ed.; Ganong's Review of Medical Physiology, 26th ed.; Katzung's Basic and Clinical Pharmacology, 16th ed.; Neuroanatomy through Clinical Cases, 3rd ed.; Review of Optometry - Visual Field Loss and Lesions; Frontiers Neurology - Optic Neuritis Therapies 2025; BrightFocus - Glaucoma Treatments 2024
This is a shared conversation. Sign in to Orris to start your own chat.