teach me lentigo maligna
Reading File
Finding Sources
Searching PubMed
"lentigo maligna" treatment diagnosis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive material. Let me compile the full structured response.
Lentigo Maligna (LM) and Lentigo Maligna Melanoma (LMM)
1. Definition and Relationship
Lentigo maligna (LM) is melanoma in situ arising within chronically photodamaged skin. It has a prolonged radial growth phase confined to the epidermis. When it becomes invasive (breaks through the basement membrane into the dermis), it is called lentigo maligna melanoma (LMM) - a distinct subtype of invasive melanoma.
LMM accounts for 10%-15% of all cutaneous melanomas, and its incidence is rising with an aging population. It is classified under the umbrella of high cumulative sun damage (CSD) melanoma.
- Dermatology 2-Volume Set 5e, p. 2406; Fitzpatrick's Dermatology, p. 2015
2. Epidemiology
| Feature | Details |
|---|---|
| Age | Most common in the 7th-8th decades; uncommon before age 40 |
| Sex | Scalp/ear involvement more common in older men with androgenetic alopecia |
| Site | Face (cheek, nose most common), neck, scalp, ears; virtually always chronically sun-exposed skin |
| Cause | Cumulative UV exposure (not intermittent) |
| Risk | Background of actinic damage (lentigines, actinic keratoses) |
Progression from LM (in situ) to LMM (invasive) is estimated to occur in about 5% of lesions, though the true rate is unknown.
3. Clinical Appearance
LM presents as a slowly enlarging, flat, freckle-like macule with:
- Irregular shape and ill-defined borders
- Varying shades of tan, brown, and black
- Background of photodamaged skin (makes clinical margins hard to see)
- Occasionally grey-white areas (regression)
When invasion occurs (LMM), a papule or nodule develops within the flat precursor macule. LM/LMM notoriously has extensive subclinical lateral spread - the lesion extends much further than is clinically visible, giving it higher recurrence rates with standard margins.
A particular surgical challenge is the "field effect": surrounding chronically UV-damaged dermis is vulnerable to infested skip lesions (foci of malignant cells discontinuous from the main lesion), making clean margin assessment unreliable on incisional biopsy.
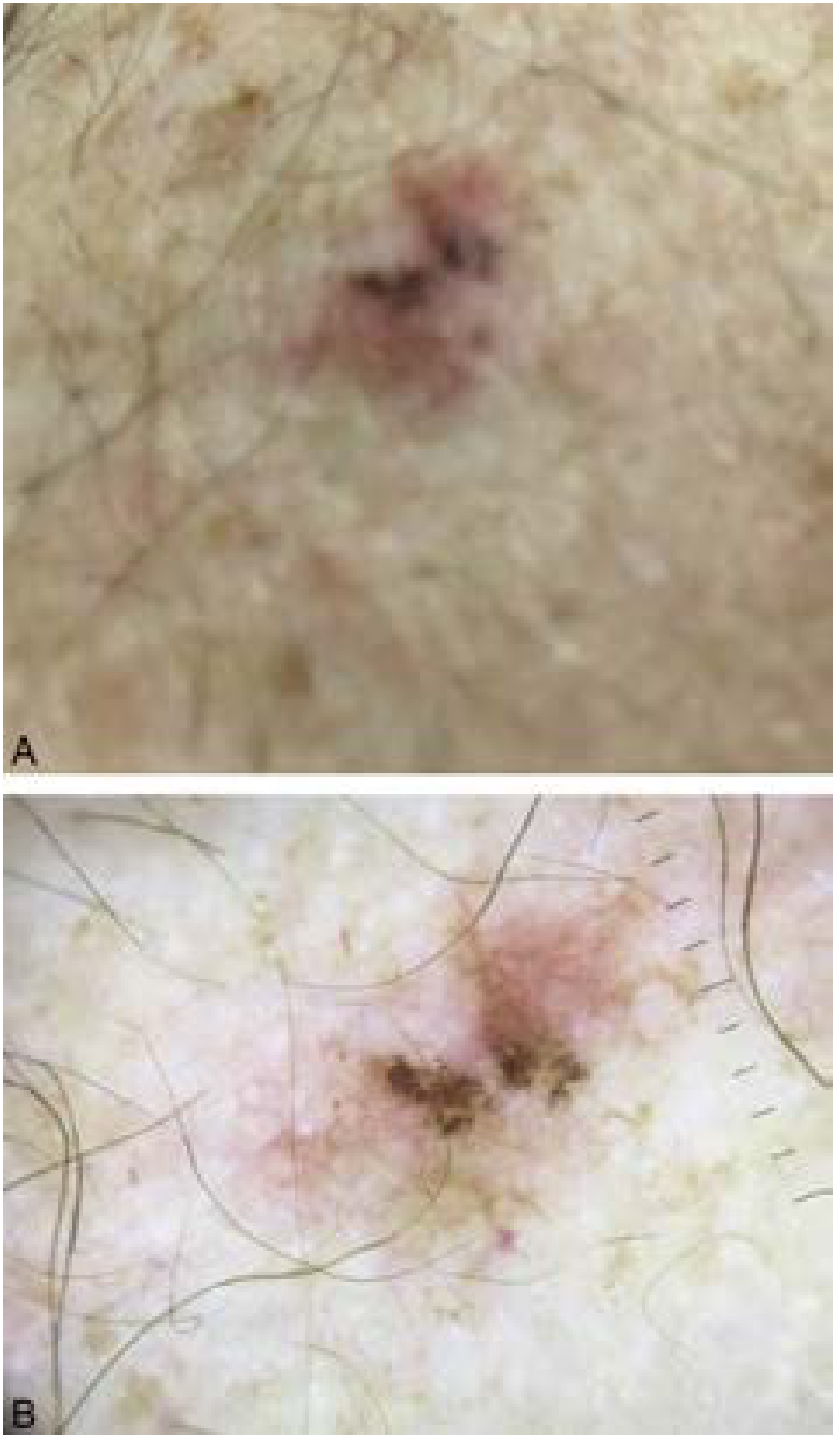
4. Dermoscopy
Dermoscopy of facial LM shows characteristic features unique to facial skin anatomy:
- Hyperpigmented follicular openings ("circle within a circle") - early sign as atypical melanocytes surround hair follicles
- Annular-granular pattern - irregular pigmented dots around follicular openings (more advanced)
- Rhomboidal structures - dark polygonal pigmentation between follicles (late sign)
- Asymmetric pigmentation of follicular openings
- Gray pseudonetwork
Distinguishing LM from pigmented actinic keratosis on dermoscopy is not always possible and remains a clinical challenge.
5. Histopathology
Key features:
- Atypical (dysplastic) melanocytes proliferating at the dermo-epidermal junction
- Predominantly single cells along the basal layer early; confluent nests develop later
- Extension down follicular epithelium (folliculotropism) - this is why atypical cells go deeper than the surface suggests, and why cryotherapy must freeze to follicular depth
- Background of severe solar elastosis (marker of chronic actinic damage)
- Pagetoid spread is less prominent than in superficial spreading melanoma
- Multinucleated giant melanocytes may be seen
- Regression (fibrosis, melanophages) common
The presence of atypical melanocytes in actinic-damaged skin creates a major challenge: distinguishing true LM from atypical/actinic melanocytic hyperplasia is difficult, especially at surgical margins. This confounds margin assessment with standard permanent sections and is a core reason why CCPDMA (Mohs/staged excision) is preferred.
6. Molecular Biology
Melanomas arising in chronically sun-damaged skin (LM/LMM type) have a distinct molecular profile:
- c-KIT aberrations (mutations and copy number changes): up to 28% of CSD melanomas
- BRAF mutations: only ~6% (much lower than non-CSD melanomas, where BRAF V600E predominates)
- This distinction is therapeutically important: imatinib/nilotinib (KIT inhibitors) may be relevant, while BRAF inhibitors (vemurafenib, dabrafenib) are less likely to be applicable
7. Differential Diagnosis
Conditions simulating LM on facial skin:
- Solar lentigo / macular seborrheic keratosis
- Pigmented actinic keratosis
- Lichenoid keratosis
- Pigmented superficial basal cell carcinoma
- Drug-induced pigmentation
8. Diagnosis
- Clinical + dermoscopy for initial assessment
- Biopsy - broad shave biopsy or punch biopsy of the darkest/most suspicious area; incisional biopsy risks sampling error given skip lesions
- Wood's lamp examination - extends visible borders; used to plan surgical/RT margins
- Reflectance confocal microscopy (RCM) - increasingly used for margin mapping before surgery; a 2025 systematic review/meta-analysis (PMID: 39548723) supports RCM for pre-surgical margin delineation
9. Treatment
First-line: Surgery
Surgery is the definitive treatment. Standard margins for melanoma in situ (MIS) are 0.5-1 cm, but LM type often requires ≥1 cm for histologic clearance due to subclinical spread.
Options for margin control:
| Technique | Notes |
|---|---|
| Staged excision with permanent sections (CCPDMA) | Complete circumferential peripheral and deep margin assessment; preferred for LM on face |
| Mohs micrographic surgery (MMS) | Comparable to staged excision; uses MART-1/Melan-A immunostaining for intraoperative margin assessment; local recurrence ~0.61% vs 7.8% for WLE in head/neck melanomas |
| Wide local excision (WLE) | Local recurrence ~7.8% for head/neck - significantly higher; sufficient for trunk/extremity MIS with clear borders |
Note: A systematic review of ~14,000 head/neck melanomas showed MMS had the lowest local recurrence (0.61%), followed by staged excision (1.8%), then WLE (7.8%) - though significant heterogeneity exists between studies.
For minimally invasive (T1a) LMM in anatomically constrained facial sites, MMS may be considered.
Second-line (when surgery not possible)
Topical imiquimod (TLR-7 agonist)
- Used off-label when surgery is not feasible or as adjuvant therapy post-surgery
- Clinical clearance ~72%-84% when used as primary therapy
- Histologic clearance ~82%-83% as neoadjuvant (prior to conservative staged excision)
- At least 60 applications at >5 times/week associated with best response
- Major caveat: difficult to confirm clearance without tissue
Radiotherapy
- Well-established for large LM on the face in elderly patients who cannot undergo surgery
- Excellent 5-year cure rates of 90%-95%
- Doses: 40-50 Gy in 10-20 fractions (or 35-100 Gy in 5-10 fractions)
- Field margins of 1-1.5 cm beyond Wood's lamp/RCM-delineated borders; depth ≥5 mm
- Dermatology 2-Volume Set 5e, p. 2883
Cryotherapy
- Historically used; double freeze-thaw cycle of 30-60 seconds each
- Recurrence rates vary widely (0-50%) across studies; overall ~9%
- Major disadvantage: no tissue for margin confirmation; recurrent invasive melanoma may hide under scarring
10. Key Comparisons with Other Melanoma Subtypes
| Feature | LM / LMM | Superficial Spreading | Nodular | Acral Lentiginous |
|---|---|---|---|---|
| % of melanomas | 10-15% | ~70% | ~15% | ~2-5% |
| Sun exposure type | Chronic, cumulative | Intermittent | Variable | Not UV-related |
| Typical age | 7th-8th decade | Middle-aged adults | Any age | 7th decade |
| Site | Face, head/neck | Trunk, extremities | Any | Palms, soles, nails |
| Growth phase | Long radial | Radial then vertical | Early vertical | Radial then vertical |
| Nevi association | Lowest (~3%) | Common | Moderate | Low |
| Desmoplastic melanoma | Highest association | Rare | Rare | Rare |
| Dominant mutation | c-KIT (28%) | BRAF V600E (~50%) | BRAF/NRAS | Variable |
11. Clinical Pearls
- Subclinical extension is the defining surgical challenge - LM extends far beyond visible/palpable margins
- Skip lesions mean a single punch biopsy can miss invasive disease; LMM can coexist with in-situ areas
- Atypical melanocytes extend down hair follicles - surgical depth and cryotherapy depth must account for this
- Background actinic damage (lentigines, actinic keratoses) can mask the lesion borders and confound histology
- LM has the highest rate of association with desmoplastic melanoma of all melanoma subtypes
- SLNB positivity rate for LMM is lower than for nodular/superficial spreading melanoma of similar Breslow thickness; desmoplastic component further decreases nodal metastasis rate
Sources: Fitzpatrick's Dermatology Vol. 1 & 2 | Dermatology 2-Volume Set 5e (Bolognia) | Current Surgical Therapy 14e | Pfenninger and Fowler's Procedures for Primary Care
Recent evidence: A 2025 meta-analysis on RCM for LM margin mapping (PMID 39548723, JEADV) supports RCM as a non-invasive pre-surgical tool. A 2023 systematic review on immunohistochemistry in Mohs for melanoma (PMID 37603089) confirms MART-1/Melan-A staining as the preferred adjunct for intraoperative margin assessment.
This is a shared conversation. Sign in to Orris to start your own chat.