Defone blood brain barrier
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a thorough, textbook-based definition of the Blood-Brain Barrier (BBB):
Blood-Brain Barrier (BBB)
Definition
The blood-brain barrier is a highly selective, semipermeable anatomical and physiological barrier that separates the circulating blood from the brain's extracellular fluid (parenchyma). It is formed primarily by the specialized endothelial cells lining the cerebral capillaries, and its principal function is to maintain the optimal microenvironment in the CNS required for normal neuronal activity.
"The blood-brain barrier is critical for maintaining the environment necessary for normal neuronal function."
- Goldman-Cecil Medicine
Historical Background
The existence of the BBB was first demonstrated over 100 years ago when scientists observed that vital dyes injected into the bloodstream stained virtually all organs except the brain. This "dye exclusion" experiment revealed that a barrier must exist between the bloodstream and neural tissue.
Anatomical Components
The BBB is not a single structure but a multi-layered complex:
| Component | Role |
|---|---|
| Capillary endothelial cells | The principal physical barrier; linked by tight junctions |
| Tight junctions (zonula occludens) | Seal the gaps between endothelial cells; prevent paracellular diffusion |
| Basement membrane | Structural scaffolding; contains pericytes |
| Pericytes | Regulate BBB permeability and integrity |
| Astrocytic end-feet (perivascular foot processes) | Wrap around capillaries; support and maintain barrier properties |
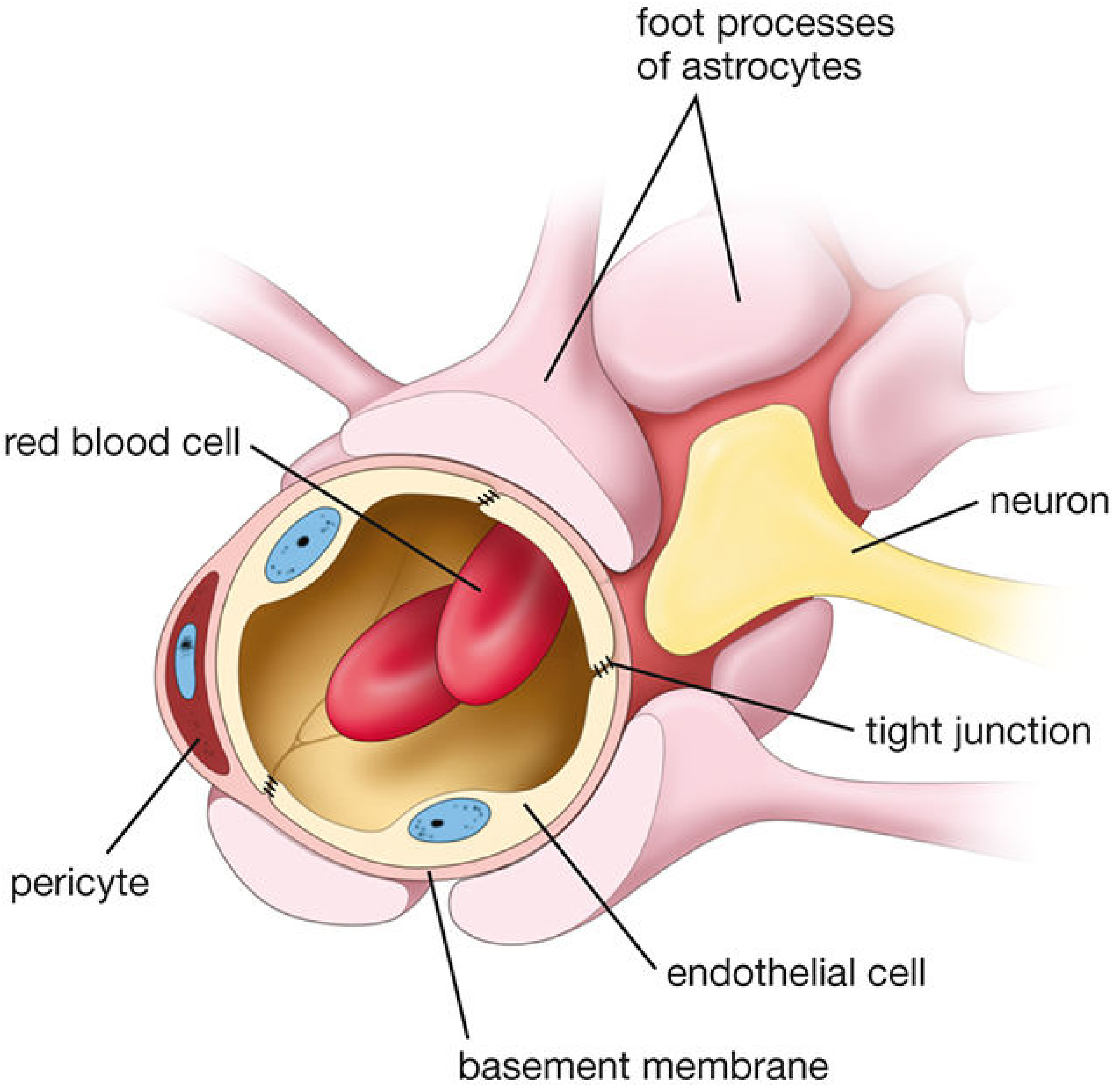
Figure: Schematic of the blood-brain barrier showing endothelial cells joined by tight junctions, pericytes, basement membrane, and astrocytic foot processes. (Histology: A Text and Atlas, 7e)
In the rest of the body, capillary endothelial cells are separated by clefts or fenestrations, allowing relatively free passage of fluids and solutes. In the brain, endothelial cells are sealed by tight junctions, forcing all transport to occur through (not between) the cells via active processes.
Key Functions
- Protect the brain from blood-borne toxins, pathogens, and harmful substances
- Meet metabolic demands - actively transports glucose, oxygen, amino acids, and other nutrients into brain tissue
- Regulate CNS homeostasis - maintains stable concentrations of ions (Na+, K+, Ca2+, Mg2+) critical for synaptic transmission and action potential generation
- Restrict and control drug delivery - limits passage of most drugs into the CNS
What Can and Cannot Cross the BBB
Freely crosses:
- O2, CO2 (by simple diffusion)
- Lipid-soluble molecules (e.g., ethanol, steroid hormones, general anesthetics)
- Small, uncharged molecules
Requires active transport:
- Glucose - via GLUT1 (glucose transporter isoform 1); the brain's sole energy source
- Amino acids, ions, vitamins, nucleotides (via solute carrier [SLC] proteins)
- L-dopa - crosses via amino acid transporters (used clinically in Parkinson's disease, because dopamine itself cannot cross)
Cannot cross:
- Hydrophilic, polar, and large molecules (>500 Da generally excluded)
- Most antibiotics, many chemotherapy agents
- Dopamine, serotonin, and other charged neurotransmitters
Efflux transporters:
- ABC transporters (e.g., P-glycoprotein) actively pump substances back into the blood using ATP - a major reason many drugs fail to reach the CNS.
Development
The BBB develops early in embryonic life through interactions between glial astrocytes and capillary endothelial cells. Astrocytes release soluble factors that upregulate tight junction proteins and barrier properties. Notably, astrocyte end-feet do not form the physical barrier themselves but are essential for maintaining it.
Breakdown of the BBB
The BBB can be disrupted by:
- Severe hypertension
- Brain tumors (tumor vasculature lacks tight junctions - exploited in MRI contrast enhancement)
- Trauma, stroke, ischemia
- Infections (meningitis, encephalitis)
- Marked hypercapnia or hypoxia
- Sustained seizure activity
- Brain edema
When disrupted, there is extravasation of fluid and proteins into brain tissue, contributing to cerebral edema and neuronal injury.
Circumventricular Organs (Exceptions)
Certain brain regions lie outside the BBB - called circumventricular organs (CVOs). These allow direct chemical communication between the bloodstream and the brain:
| Organ | Function |
|---|---|
| Area postrema | Chemoreceptor trigger zone (vomiting) |
| Median eminence | Pituitary hormone regulation |
| Neurohypophysis | Hormone release (ADH, oxytocin) |
| Pineal gland | Melatonin/circadian rhythms |
| Subfornical organ | Fluid balance |
| Organum vasculosum of the lamina terminalis (OVLT) | Neuroendocrine function |
The Neurovascular Unit
A broader concept related to the BBB is the neurovascular unit - the physiological interrelationship among endothelial cells, vascular smooth muscle, astrocytes, pericytes, and neurons. Local neural activity and pH directly influence local cerebral blood flow through this unit, linking brain function to vascular regulation.
Blood-CSF Barrier (Related Concept)
A similar barrier - the blood-CSF barrier - exists at the choroid plexus. Here, the capillaries are freely permeable, but the choroid plexus epithelial cells form the barrier between blood and CSF. Substances can then pass relatively freely between CSF and brain parenchyma across the ependymal layer.
Sources: Goldman-Cecil Medicine; Histology: A Text and Atlas with Correlated Cell and Molecular Biology, 7e; Neuroanatomy through Clinical Cases, 3rd ed.
Difference between Nephritic syndrome and nephritis explain
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Excellent - I now have comprehensive textbook content. Let me compose the full answer.
Nephritis vs. Nephritic Syndrome - A Complete Explanation
These two terms are frequently confused. The key distinction is:
- Nephritis = a broad umbrella term for kidney inflammation (any compartment)
- Nephritic syndrome = a specific cluster of clinical signs and symptoms resulting from glomerular inflammation
Think of it this way: nephritis is the disease process; nephritic syndrome is the clinical presentation of one type of nephritis.
1. NEPHRITIS - The Broad Term
Definition: Nephritis refers to inflammation of the kidney, and can affect any of its three main compartments:
| Type | Compartment Affected | Example Diseases |
|---|---|---|
| Glomerulonephritis (GN) | Glomeruli | Post-streptococcal GN, IgA nephropathy, lupus nephritis |
| Tubulointerstitial Nephritis | Tubules + interstitium | Drug-induced (NSAIDs, antibiotics, PPIs), infection, sarcoidosis |
| Pyelonephritis | Renal pelvis + parenchyma | Bacterial kidney infection (E. coli most common) |
| Vasculitis-associated nephritis | Renal vessels | ANCA-associated vasculitis, Goodpasture syndrome |
"Interstitial nephritis is characterized by an inflammatory infiltrate in the interstitium of the kidney. It can be primary and begin in the tubulointerstitium or appear as a secondary event and spread from blood vessels, including the glomerular capillaries."
- Goldman-Cecil Medicine
Nephritis can be caused by:
- Autoimmunity (lupus, ANCA-associated disease)
- Toxic insult (drugs, heavy metals)
- Infection (bacterial, viral, fungal)
- Drugs - almost any class (especially antibiotics, NSAIDs, diuretics, proton pump inhibitors, immune checkpoint inhibitors)
2. NEPHRITIC SYNDROME - The Specific Clinical Syndrome
Definition: Nephritic syndrome is a specific constellation of clinical features that results from glomerular inflammation causing damage to the capillary wall.
"Nephritic syndrome is defined as the presence of glomerular hematuria in the form of dysmorphic red blood cells (RBCs) or RBC casts, in combination with hypertension, edema, reduced GFR with or without oliguria, and non-nephrotic-range proteinuria."
- NKF Primer on Kidney Diseases, 8e
The Classic 5 Features of Nephritic Syndrome (PHAROH):
| Feature | Mechanism |
|---|---|
| Hematuria (macro or micro) | Damaged capillary walls allow RBCs to escape into urine; dysmorphic RBCs and RBC casts are pathognomonic |
| Hypertension | Fluid retention + renin release from ischemic kidneys |
| Azotemia (elevated BUN/creatinine) | Reduced GFR from glomerular inflammation |
| Oliguria | Severely reduced GFR |
| Proteinuria | Usually sub-nephrotic (<3.5 g/day); glomerular wall injury, but not massive enough to cause hypoalbuminemia |
| Edema | Sodium and water retention secondary to reduced GFR; usually less severe than nephrotic syndrome |
"The inflammatory reaction severely injures the capillary walls, permitting blood to pass into the urine and inducing hemodynamic changes that lead to a reduction in GFR."
- Robbins & Kumar Pathologic Basis of Disease
3. The Key Difference - Summary Table
| Feature | Nephritis (General) | Nephritic Syndrome (Specific) |
|---|---|---|
| Nature | Broad pathological term (inflammation of kidney) | Specific clinical syndrome |
| Kidney compartment | Glomeruli, tubules, interstitium, or vessels | Glomeruli only |
| Defined by | Histopathology / etiology | Clinical + lab findings |
| Proteinuria | Variable | Sub-nephrotic (<3.5 g/day) |
| Hematuria | May or may not be present | Always present (dysmorphic RBCs, RBC casts) |
| Hypertension | Variable (present in GN, absent in interstitial) | Hallmark feature |
| Edema | Variable | Mild to moderate |
| Onset | Acute or chronic | Usually abrupt |
| Serum albumin | Usually normal (unless severe) | Normal or slightly reduced |
| Examples | Interstitial nephritis, pyelonephritis, GN, lupus nephritis | Post-strep GN, IgA nephropathy, RPGN, lupus GN |
4. Nephritic Syndrome vs. Nephrotic Syndrome (Bonus Comparison)
Since these two are also commonly confused:
| Feature | Nephritic Syndrome | Nephrotic Syndrome |
|---|---|---|
| Onset | Abrupt | Insidious |
| Edema | Mild (++) | Massive (++++) |
| Blood pressure | Raised | Normal |
| Proteinuria | Mild-moderate (++) | Massive (>3.5 g/day) (++++) |
| Hematuria | +++ (hallmark) | May or may not occur |
| RBC casts | Present (pathognomonic) | Absent |
| Serum albumin | Normal / slightly reduced | Low (hypoalbuminemia) |
| JVP | Raised | Normal/low |
| Mechanism | Glomerular inflammation | Glomerular permeability to protein |
(Table adapted from Comprehensive Clinical Nephrology, 7e)
5. Diseases That Cause Nephritic Syndrome (a type of nephritis)
These are all forms of glomerulonephritis (GN) - a subtype of nephritis - that present with nephritic syndrome:
- Post-infectious (Post-streptococcal) GN - classic example; children 6-10 years, 1-4 weeks after strep pharyngitis or impetigo
- IgA Nephropathy (Berger's disease) - most common primary glomerulopathy worldwide; synpharyngitic hematuria
- Rapidly Progressive (Crescentic) GN (RPGN) - most severe form; weeks to months to kidney failure
- Lupus Nephritis - can present as nephritic, nephrotic, or mixed
- ANCA-associated vasculitis (Granulomatosis with Polyangiitis, Microscopic Polyangiitis)
- Anti-GBM disease (Goodpasture syndrome) - may have pulmonary hemorrhage too
Analogy to Remember
Nephritis is like saying someone has "lung disease" - it could be pneumonia, asthma, TB, or cancer. Nephritic syndrome is like saying someone has "type 1 respiratory failure" - it's a specific set of measurable findings that tells you the type and location of injury (glomerular inflammation).
Sources: Robbins & Kumar Pathologic Basis of Disease; NKF Primer on Kidney Diseases, 8e; Comprehensive Clinical Nephrology, 7e; Goldman-Cecil Medicine; Tietz Textbook of Laboratory Medicine, 7e
Define variocele causes sign.symptoms dignoses treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content from multiple authoritative urology sources. Here is the complete answer:
Varicocele - Complete Overview
Definition
A varicocele is an abnormal dilation and tortuosity of the pampiniform venous plexus within the spermatic cord, caused by retrograde venous blood flow through incompetent (valve-deficient) internal spermatic veins. It is the male equivalent of varicose veins in the leg.
"Varicocele is the result of retrograde venous blood flow through incompetent veins of the pampiniform plexus of the spermatic cord... described as the most common surgically correctable cause of male subfertility."
- Smith & Tanagho's General Urology, 19e
Epidemiology
| Population | Prevalence |
|---|---|
| General healthy young men | ~15% |
| Subfertile men | ~40% (left-sided) |
| Adolescents (clinically diagnosed) | 8-16% |
| Bilateral (healthy men) | <10% |
| Bilateral (subfertile men) | Up to 20% |
- Varicoceles do not spontaneously regress
- Rarely detected before age 10; peak incidence at Tanner stage 3 (puberty)
Why Predominantly LEFT-Sided? (Anatomy)
Several anatomical factors explain the left-side predominance (85-95% of cases):
| Anatomical Factor | Effect |
|---|---|
| Left internal spermatic vein is longer than the right | Greater hydrostatic pressure column |
| Left spermatic vein drains into left renal vein at a right angle | Higher resistance to flow; back-pressure |
| Right spermatic vein drains obliquely into the IVC | Lower venous pressure; less reflux |
| Left renal vein compressed between aorta and SMA ("nutcracker phenomenon") | Increased venous pressure transmitted down |
"The left internal spermatic vein... typically joins the left renal vein at a right angle compared to the oblique insertion of the right spermatic vein into the inferior vena cava. As a result, higher venous pressures are transmitted to the left spermatic cord veins and result in retrograde reflux of blood."
- Smith & Tanagho's General Urology, 19e
Important: An isolated right-sided varicocele should always prompt investigation for a renal tumor, retroperitoneal lymphadenopathy, or anatomical variants (e.g., situs inversus), as this is an uncommon and potentially sinister finding.
Causes & Pathogenesis
Primary Cause
- Valvular incompetence of the internal spermatic veins - the fundamental defect allowing retrograde blood flow
- Genetic predisposition - increased incidence in first-degree relatives of affected men
Mechanisms of Testicular Damage (Theories):
-
Elevated intratesticular temperature (most accepted theory)
- Incompetent reflux of warm venous blood disrupts normal countercurrent heat exchange in the pampiniform plexus
- Spermatogenesis requires temperatures 2-4°C below core body temperature
- Elevated temperature directly inhibits spermatogenesis
-
Oxidative stress
- Increased reactive oxygen species in semen → DNA fragmentation in sperm
-
Hypoperfusion / venous stasis
- Stagnant blood causes hypoxia and toxic metabolite accumulation in the testis
-
Reflux of renal/adrenal metabolites
- Retrograde flow may carry hormonal byproducts from the renal/adrenal veins back into the testicular venous system
-
Pituitary-gonadal hormonal dysfunction
- Varicoceles are associated with elevated FSH and LH, reduced testosterone
Signs & Symptoms
Symptoms
| Symptom | Details |
|---|---|
| Dull, dragging scrotal ache | The most common complaint; usually in the left testicle |
| Worse with prolonged standing, physical exertion, or end of day | Due to increased venous pooling |
| Infertility | Often the presenting complaint - abnormal semen parameters |
| Many patients are completely asymptomatic | Discovered incidentally during infertility workup or routine exam |
Signs
| Sign | Details |
|---|---|
| "Bag of worms" (pathognomonic) | Soft, irregular, tortuous veins felt superior to the testis and epididymis - classic description |
| Positive cough impulse / Valsalva test | Veins become more prominent and palpable when the patient performs Valsalva maneuver; confirms diagnosis |
| Ipsilateral testicular atrophy | Smaller left testis compared to right; reflects impaired spermatogenesis |
| Disappears on lying down | Unlike a solid mass - venous engorgement reduces when supine |
Grading System (Dubin-Amelar Classification):
| Grade | Description |
|---|---|
| Grade 0 (subclinical) | Not palpable; only detected on Doppler US |
| Grade 1 | Palpable only during Valsalva maneuver |
| Grade 2 | Palpable at rest without Valsalva |
| Grade 3 | Visible through the scrotal skin; easily palpable |
Effect on Fertility
- Sperm quality - decreased concentration, motility (most profound effect), and morphology
- Testicular volume decreases progressively (atrophy) if untreated
- Associated with higher semen DNA fragmentation
- Left varicocele can cause bilateral testicular damage due to shared venous and lymphatic connections
Diagnosis
1. Physical Examination (Gold Standard)
- Examine patient standing in a warm room
- Palpate above and around the testis with and without Valsalva
- Classic finding: tortuous, soft, compressible veins - "bag of worms"
2. Scrotal Doppler Ultrasound
- Most sensitive and specific imaging modality
- Venous diameter >3 mm with demonstrable retrograde flow on Valsalva = diagnostic
- Reserved for: subclinical cases, uncertain physical exam, evaluating testicular volume
3. Semen Analysis
- Evaluate concentration, motility, morphology
- Abnormalities (especially reduced motility) are the most common indication for treatment
4. Hormonal Profile
- FSH, LH, testosterone - if fertility is a concern
- Elevated FSH suggests impaired spermatogenesis
5. Venography (rarely needed)
- Selective catheterization of testicular vein; shows reflux definitively
- Used when planning percutaneous embolization
Treatment
Treatment is indicated for:
- Infertility with abnormal semen parameters
- Symptomatic pain
- Testicular atrophy (especially in adolescents)
- Large, clinically apparent varicocele in adolescents
The goal of all treatments: stop retrograde venous flow in the internal spermatic veins.
1. Surgical Ligation
| Approach | Notes |
|---|---|
| Subinguinal / Inguinal (open) | Most common; ligates the veins in the inguinal canal or below; aponeurosis of external oblique divided |
| Retroperitoneal | High ligation; higher recurrence rate |
| Laparoscopic | Less invasive; higher complication rate |
| Microsurgical subinguinal | Gold standard surgical approach; lowest recurrence (0-15%), identifies and preserves lymphatics and testicular artery |
2. Percutaneous Embolization (Radiological)
- Catheter inserted via right femoral or jugular vein → IVC → left renal vein → left testicular vein
- Venography confirms reflux and delineates anatomy
- Metal coils placed from distal to proximal to occlude the vein
- Advantages: day-case procedure, minimal pain, fastest return to work (1 day)
- Disadvantages: technical failure in 10-15%, higher recurrence possible
Outcomes Comparison:
| Outcome | Open Surgical | Laparoscopic | Radiologic Embolization |
|---|---|---|---|
| Semen improvement | 66% | 50-70% | 60% |
| Pregnancy rate | 35% | 12-32% | 10-50% |
| Recurrence | 0-15% | 5-25% | 0-10% |
| Return to work | 5 days | 5.3 days | 1 day |
| Overall complications | 1% | 4% | 10-15% |
3. Watchful Waiting
- For asymptomatic, subclinical, or grade 1 varicoceles with normal semen
- Expected natural pregnancy rate ~16% without intervention
Note: NICE guidelines state that varicocele surgery should not be offered as a standalone fertility treatment because it does not reliably improve pregnancy rates - discuss all options including IVF (pregnancy rate ~35%) with the patient.
Summary
| Aspect | Key Point |
|---|---|
| Definition | Dilated, tortuous pampiniform plexus veins due to venous valvular incompetence |
| Side | 85-95% left-sided; isolated right = rule out renal tumor |
| Most common symptom | Dull, dragging scrotal ache |
| Classic sign | "Bag of worms" above the testis |
| Key investigation | Physical exam + scrotal Doppler US |
| Clinical importance | Most common correctable cause of male infertility |
| Best treatment | Microsurgical subinguinal ligation (lowest recurrence) |
Sources: Campbell Walsh Wein Urology, 3-Volume Set; Smith & Tanagho's General Urology, 19e; Gray's Anatomy for Students; Grainger & Allison's Diagnostic Radiology
Infertility occur after operation
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative surgical and urology textbooks. Here is the complete answer:
Male Infertility Occurring After Surgery (Iatrogenic Male Infertility)
Overview
Iatrogenic (surgery-induced) male infertility refers to infertility caused by surgical procedures that damage the anatomical structures or neural pathways essential for sperm production, transport, or ejaculation. It falls under the broader category of acquired male infertility.
"Surgeons must be aware of iatrogenic causes of infertility in groin and pelvic surgical procedures from damage to the spermatic cord vasculature, vas deferens, and ejaculatory duct region or vasal entrapment from mesh used for inguinal hernia repair."
- Sabiston Textbook of Surgery
Classification of Post-Surgical Infertility by Mechanism
1. OBSTRUCTIVE AZOOSPERMIA - Blockage of Sperm Transport
The most common surgical cause. Sperm are produced normally but cannot reach the ejaculate due to a mechanical obstruction.
A. Vas Deferens Injury (Most Common Culprit - Inguinal Hernia Repair)
| Type of Injury | How It Happens |
|---|---|
| Transection / laceration | Direct cutting of the vas during open herniorrhaphy |
| Crush injury | Endoscopic grasping of the vas deferens during laparoscopic repair |
| Mesh entrapment | Synthetic mesh wraps around and slowly compresses the vas; causes chronic scarring → obstruction → azoospermia |
| Cicatrization | Mesh-induced inflammation causes progressive fibrosis around the vas |
"Injury to the vas deferens within the cord may lead to infertility. In open inguinal hernia repairs, isolating the vas deferens along with the cord structures using digital manipulation may cause injury or disruption. In endoscopic approach, grasping the vas may result in a crush injury."
- Schwartz's Principles of Surgery, 11e
"Herniorrhaphy especially with mesh may result in obstruction of the vas deferens in the inguinal canal. If both vasa are occluded, azoospermia likely results."
- Campbell Walsh Wein Urology
Management of vas transection: Immediate urological consultation and early vas-to-vas anastomosis (vasovasostomy) if diagnosed intraoperatively gives the best outcome.
B. Epididymal Injury
- Scrotal surgery (hydrocele repair, epididymal cyst excision, spermatocele removal) can damage the delicate epididymal tubules
- The epididymis is the site of sperm maturation and storage - even partial obstruction here causes reduced motility and count
C. Ejaculatory Duct Obstruction
- Transurethral resection of the prostate (TURP) or bladder neck surgery can damage or scar the ejaculatory ducts at the level of the prostate
- Results in low-volume ejaculate or azoospermia
2. TESTICULAR DAMAGE - Impaired Sperm Production
A. Ischemic Orchitis
- Cause: Injury to the pampiniform venous plexus during inguinal hernia repair → venous congestion and inflammation
- Presentation: Enlarged, indurated, painful testis within 1 week of surgery
- Occurs in <1% of primary hernia repairs but higher for recurrent repairs
- Usually self-limiting - treat with NSAIDs and reassurance
- Diagnosis: Scrotal Doppler US to confirm blood flow (differentiate ischemia from necrosis)
- Emergency orchiectomy only if frank testicular necrosis is confirmed
B. Testicular Atrophy
- Cause: Injury to the testicular artery during hernia repair or orchidopexy
- The testicular artery runs within the spermatic cord - at risk in inguinal surgery
- Even when the artery is injured, collateral flow from inferior epigastric, vesical, prostatic, and scrotal arteries can preserve viability - but insufficient flow causes progressive atrophy
- Develops slowly (weeks to months) after surgery
- Results in decreased spermatogenesis and reduced testosterone
C. Orchidopexy for Undescended Testis
- Surgery to bring down a cryptorchid testis can devascularize the testis if the vessels are under tension
- Even successful orchidopexy may not fully restore fertility if the testis was already damaged by prolonged intra-abdominal position and heat
3. EJACULATORY DYSFUNCTION - Failure of Sperm Delivery
A. Retrograde Ejaculation
The most common ejaculatory complication of pelvic/retroperitoneal surgery.
Mechanism: During normal ejaculation, the sympathetic nervous system (T10-L2) causes:
- Contraction of the vas deferens, epididymis, seminal vesicles, and prostate (emission)
- Closure of the internal urethral sphincter (bladder neck) - prevents backflow into bladder
When sympathetic nerves are damaged, the bladder neck fails to close → semen is ejected backward into the bladder instead of forward through the urethra.
Surgeries that cause retrograde ejaculation:
| Surgery | Nerve at Risk |
|---|---|
| Retroperitoneal lymph node dissection (RPLND) for testicular cancer | Superior hypogastric plexus (sympathetic) |
| Aorto-iliac vascular surgery | Sympathetic chain, hypogastric plexus |
| Colorectal surgery (anterior resection, sigmoid colectomy) | Pelvic sympathetic nerves |
| TURP / bladder neck surgery | Internal urethral sphincter directly |
| Lumbar spine surgery (L4/L5/S1) | Superior hypogastric plexus |
"Retrograde ejaculation may also occur as a result of nerve damage associated with certain surgical procedures, including bladder neck surgery, transurethral resection of the prostate, colorectal surgery, and retroperitoneal lymph node dissection."
- Medical Physiology (Boron & Boulpaep)
Diagnosis: >15 sperm per high-power field in post-ejaculation urine confirms retrograde ejaculation.
Treatment:
- Sympathomimetic drugs (alpha-adrenergic agonists) can restore bladder neck tone:
- Phenylephrine, ephedrine, imipramine (norepinephrine reuptake inhibitor)
- Sperm harvesting from post-ejaculation urine for IVF/IUI if pharmacological treatment fails
B. Anejaculation (Absence of Ejaculation)
- Complete sympathetic denervation causes neither emission nor ejaculation
- Seen after radical prostatectomy, cystoprostatectomy, extensive pelvic surgery
- Treatment: Penile vibratory stimulation (PVS) or electroejaculation to retrieve sperm
4. HORMONAL / PRETESTICULAR CAUSES
Pituitary Surgery
- Transsphenoidal surgery for pituitary adenoma can damage gonadotroph cells
- Results in reduced/absent FSH and LH → secondary hypogonadism → impaired spermatogenesis
- Present with: low testosterone, low LH/FSH, azoospermia or severe oligospermia
- Treatable with exogenous gonadotropin replacement (hCG + recombinant FSH)
5. VARICOCELE REPAIR - Paradoxical Infertility Risk
(From the previous topic context)
- Ligation of the testicular artery during varicocele repair can cause testicular atrophy
- Lymphatic injury can cause post-operative hydrocele
- This is why microsurgical subinguinal repair is preferred - allows identification and preservation of the testicular artery and lymphatics under magnification
Summary Table - Surgeries and Their Infertility Mechanisms
| Surgery | Mechanism | Resulting Problem |
|---|---|---|
| Inguinal hernia repair | Vas deferens injury, mesh entrapment, testicular artery injury | Obstructive azoospermia, testicular atrophy |
| Scrotal surgery (hydrocele, epididymal cyst) | Epididymal tubule damage | Obstructive azoospermia |
| TURP / bladder neck surgery | Bladder neck sphincter damage, ejaculatory duct scarring | Retrograde ejaculation, azoospermia |
| RPLND (testicular cancer) | Sympathetic nerve damage (hypogastric plexus) | Retrograde ejaculation / anejaculation |
| Colorectal / rectal surgery | Pelvic sympathetic + parasympathetic nerve damage | Retrograde ejaculation, erectile dysfunction |
| Aorto-iliac vascular surgery | Sympathetic chain injury | Retrograde ejaculation |
| Pituitary surgery | Gonadotropin deficiency (FSH/LH) | Non-obstructive azoospermia |
| Orchidopexy | Devascularization, prolonged cryptorchidism | Testicular atrophy, impaired spermatogenesis |
| Varicocele repair | Testicular artery ligation (if not microsurgical) | Testicular atrophy |
| Lumbar spine surgery | Superior hypogastric plexus injury | Retrograde ejaculation |
Management Approach After Surgery-Related Infertility
| Finding | Next Step |
|---|---|
| Suspected vas deferens transection | Urgent urology referral; vasovasostomy if feasible |
| Retrograde ejaculation | Sympathomimetics; post-ejaculate urine sperm harvest for IUI/IVF |
| Testicular atrophy + azoospermia | Hormonal evaluation; surgical sperm retrieval (TESE/MESA) + IVF/ICSI |
| Pituitary injury | FSH, LH, testosterone levels; gonadotropin replacement therapy |
| Obstructive azoospermia (patent testes) | Vasal/epididymal reconstruction or sperm retrieval + ICSI |
Sources: Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery; Campbell Walsh Wein Urology; Smith & Tanagho's General Urology, 19e; Medical Physiology (Boron & Boulpaep); Mulholland & Greenfield's Surgery, 7e
This is a shared conversation. Sign in to Orris to start your own chat.