Viral exanthems
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
viral exanthem rash children measles rubella varicella
I now have comprehensive content. Let me compile the full response.
Viral Exanthems
A viral exanthem is a widespread cutaneous eruption that occurs as a manifestation of systemic viral infection — either from direct viral invasion of the skin, immune-complex deposition, or cytokine-mediated inflammatory responses. They are among the most common dermatologic presentations in children, though adults are also affected.
Classification Framework
| # | Eponym | Disease | Virus | Rash Morphology |
|---|---|---|---|---|
| 1st | — | Measles (Rubeola) | Measles virus (Paramyxoviridae) | Morbilliform (maculopapular), cephalocaudal |
| 2nd | — | Scarlet fever | Strep. pyogenes (bacterial) | Sandpaper texture |
| 3rd | — | Rubella (German measles) | Rubella virus (Togaviridae) | Fine maculopapular, face → trunk |
| 4th | — | Staphylococcal scalded skin | Staph. aureus (bacterial) | Bullous, erosive |
| 5th | Erythema infectiosum | Fifth disease | Parvovirus B19 | "Slapped cheek" + lacy reticular |
| 6th | Exanthem subitum | Roseola infantum | HHV-6B (HHV-7) | Rose-pink macules post-fever |
The numbered "diseases of childhood" classification is historical. Modern understanding maps exanthems by virus type and morphology.
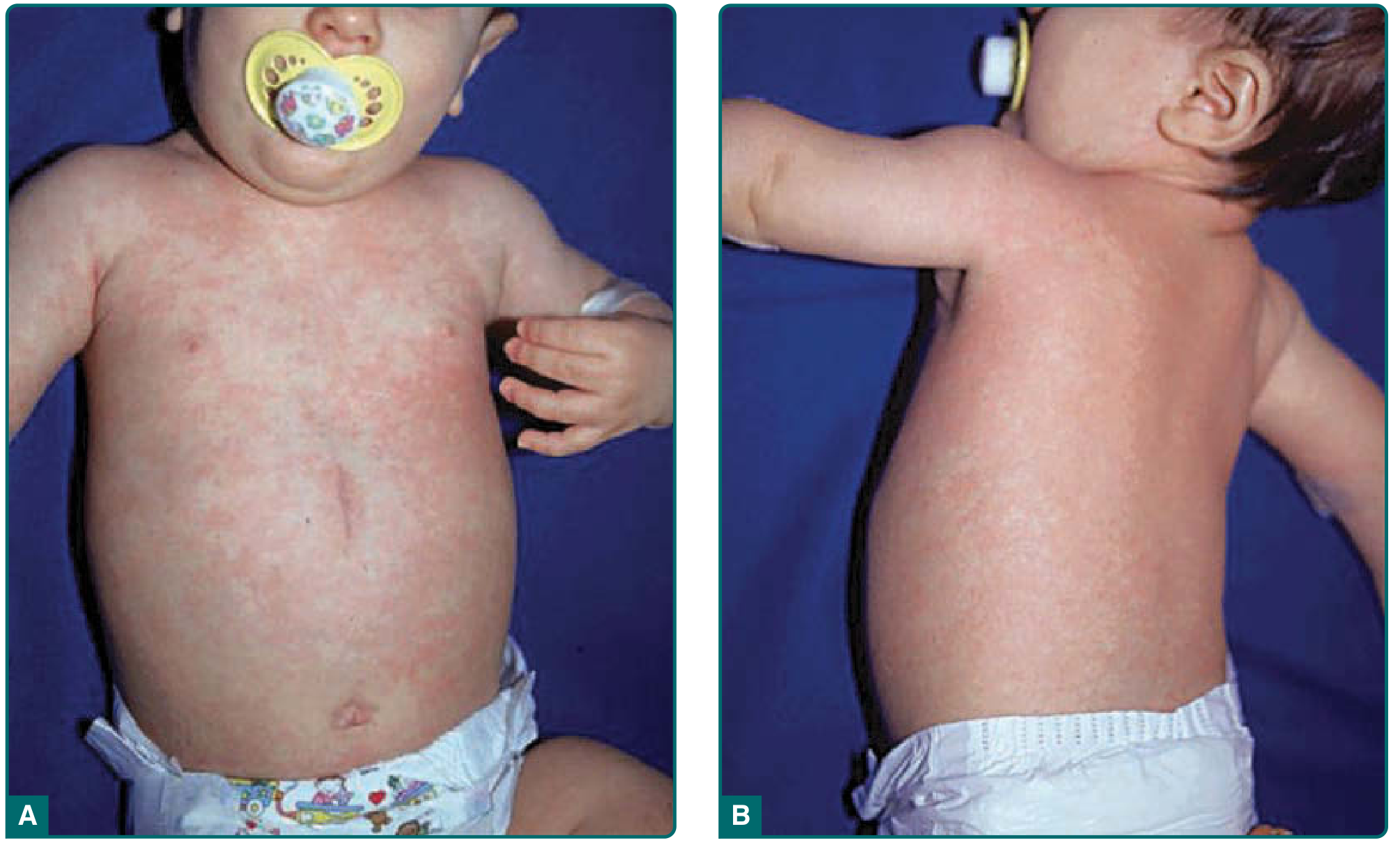
1. Measles (Rubeola) — "First Disease"
Virus: Morbillivirus, single-stranded RNA, Paramyxoviridae family. Humans are the only natural hosts. Transmission is airborne; infectious droplets persist for up to 2 hours in enclosed spaces.
Prodrome (3–4 days): High fever, the 3 Cs — Cough, Coryza (rhinorrhea), Conjunctivitis.
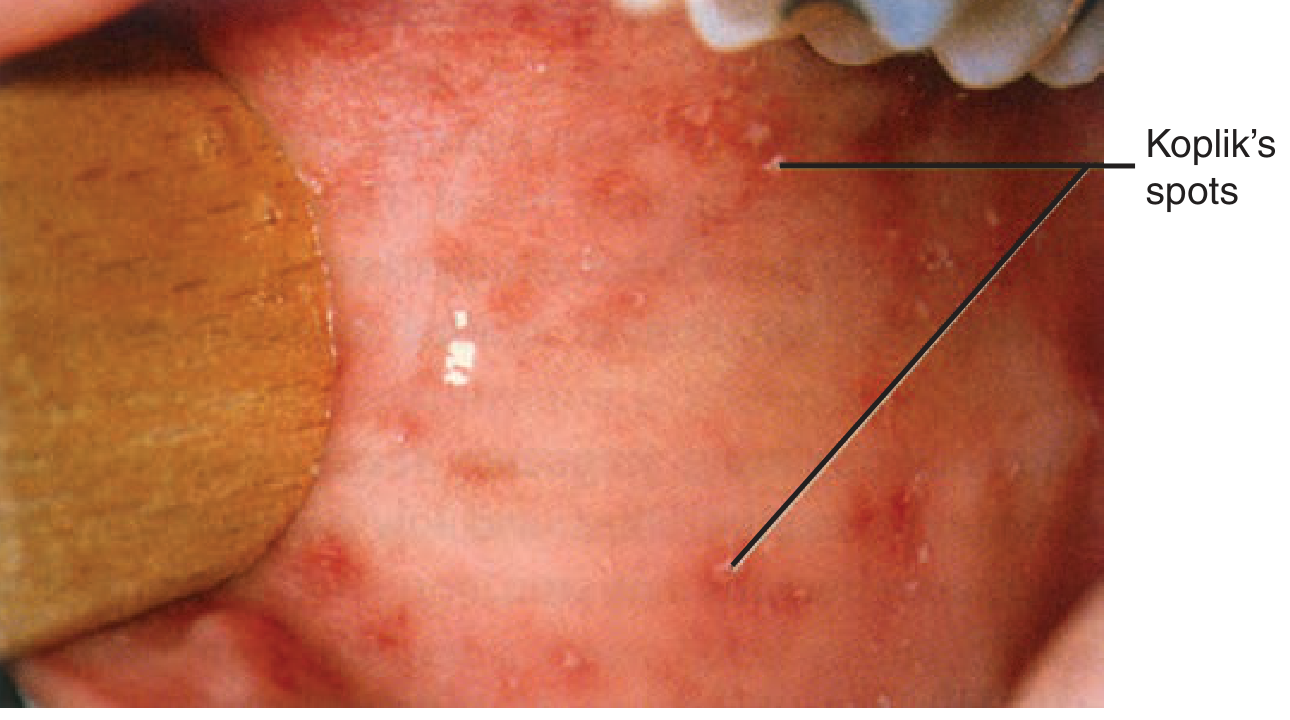
Pathognomonic sign — Koplik spots: Tiny white lesions ("grains of sand") on an erythematous buccal mucosa, appearing 1–2 days before the rash. They are transient and easily missed.

Exanthem: Erythematous maculopapular rash beginning at the hairline/forehead, spreading cephalocaudally over 3–5 days. Lesions on the trunk can coalesce into broad, irregular patches. Clears from head downward.

Complications: Pneumonia (most common cause of death), post-measles encephalomyelitis (~1/1000 cases), subacute sclerosing panencephalitis (rare, years later), otitis media, diarrhea, and corneal ulceration.
Immunosuppression: Transient depression of T-cell counts and delayed-type hypersensitivity occurs during infection → increased susceptibility to bacterial superinfection.
Treatment: Supportive; Vitamin A supplementation reduces morbidity and mortality, particularly in children with deficiency. — Fitzpatrick's Dermatology, Vol. 1&2
2. Rubella (German Measles) — "Third Disease"
Virus: Rubella virus, single-stranded RNA (Togaviridae). Transmitted via respiratory droplets.
Prodrome: Mild fever, malaise. Notably, posterior cervical, suboccipital, and postauricular lymphadenopathy — often preceding the rash by up to 7 days — is the most characteristic feature.
Exanthem: Fine pink maculopapular rash beginning on the face, spreading to trunk and extremities within 24 hours, and clearing within 3 days. Unlike rubeola, lesions on the extremities remain discrete (do not coalesce significantly). Desquamation may follow. — Fitzpatrick's Dermatology

Enanthem: Forchheimer spots — petechiae on the soft palate (non-pathognomonic).
Arthritis: Up to 70% of adult women develop arthritis of small and large joints, appearing as the rash fades; can persist for weeks.
Diagnosis: Rubella-specific IgM antibody (detectable up to 8 weeks post-infection) or 4-fold rise in IgG titer. RT-PCR for genotyping in outbreak settings.
Congenital Rubella Syndrome (CRS)
Infection in the first 12 weeks of pregnancy causes severe teratogenicity in up to 85% of exposed fetuses:
- Classic triad: Cataracts, congenital heart disease (PDA, pulmonary artery stenosis, VSD), sensorineural deafness
- Microcephaly, retinopathy, glaucoma
- Neonatal: blueberry muffin lesions (dermal erythropoiesis), hepatosplenomegaly, thrombocytopenia — Fitzpatrick's Dermatology; Jawetz Medical Microbiology
3. Erythema Infectiosum (Fifth Disease) — Parvovirus B19
Virus: Parvovirus B19, single-stranded DNA; transmitted primarily via the respiratory route, also blood products and vertically.
Incubation: 4–12 days (some sources give 10–20 days).
Stage 1 — Prodrome: Fever, malaise, headache, myalgia, mild leukopenia.
Stage 2 — "Slapped-cheek" rash: Confluent, indurated, intensely erythematous rash on the face with circumoral pallor; child appears as if the cheeks were slapped. At this stage, the child is no longer infectious (viremia has cleared).
Stage 3 — Lacy reticular rash: 1–2 days later, a macular lace-like (reticular) pattern spreads to the arms, legs, and trunk (especially exposed surfaces). The rash may recur for 2–4 weeks, worsened by heat, sunlight, exercise, and emotional stress.
Arthropathy: Arthralgia/arthritis — especially in adolescent and adult women; can persist for weeks to months.
Serious complications:
- Aplastic crisis in patients with chronic hemolytic anemias (sickle cell, hereditary spherocytosis) — the virus infects erythroid progenitor cells (erythroblasts), causing transient red-cell aplasia
- Hydrops fetalis: Transplacental transmission in first 20 weeks of pregnancy → fetal anemia → high-output heart failure → generalized fetal edema; can be fatal
- Immunocompromised: chronic pure red-cell aplasia
Diagnosis: Parvovirus B19–specific IgM antibody in convalescence; PCR for DNA (especially useful in immunocompromised patients who may not mount antibody response). — Sherris & Ryan's Medical Microbiology
4. Exanthem Subitum (Roseola Infantum / Sixth Disease)
Virus: HHV-6B (primarily); HHV-7 causes a similar but less common illness. Both are β-herpesviruses; HHV-6 has tropism for CD4+ T lymphocytes. Transmitted via infected saliva.
Epidemiology: Affects children 6 months–3 years; peak incidence 6–12 months when maternal IgG wanes. Seroprevalence reaches 90–100% by age 3–4 years. Most common in spring.
Clinical pattern — distinctive temporal sequence:
- Fever phase: Abrupt onset of high fever (38–40°C) lasting 3–7 days, often with irritability, rhinorrhea, diarrhea. Febrile seizures occur in ~10–15%. "Sleepy" appearance from palpebral edema.
- Defervescence → rash: The exanthem appears 1 day before to 2 days after the fever breaks — this temporal pattern (fever then rash) is the hallmark distinguishing ES from most other viral exanthems where they occur simultaneously.
- Exanthem: Rose-pink (2–5 mm) macules and papules with a white halo, distributed on the neck and trunk; less commonly face and proximal extremities. Lasts 3–5 days.
Nagayama spots: Erythematous papules on the soft palate/uvula that may precede the exanthem.
Diagnosis: Clinical; PCR or serology for confirmation. HHV-6 DNA can integrate into germline (chromosomally integrated HHV-6) in ~1% of the population.
HHV-6 reactivation: Common in immunocompromised patients (especially stem cell transplant recipients — up to 50% reactivation); can cause encephalitis, pneumonitis, morbilliform rash. — Fitzpatrick's Dermatology; Dermatology 2-Volume Set 5e
5. Hand-Foot-Mouth Disease (HFMD)
Virus: Enteroviruses — classically Coxsackievirus A16 and Enterovirus 71 (EV71); also CVA5, A6, A7, B1–B5, echoviruses. CVA6 causes atypical HFMD with more widespread bullous involvement.
Epidemiology: Children <10 years; peak in summer and fall in temperate climates.
Transmission: Fecal-oral and respiratory. Incubation: 3–6 days; viral shedding up to 5 weeks.
Prodrome: Low-grade fever (38–39°C), malaise, sore mouth, occasionally abdominal pain and upper respiratory symptoms.
Exanthem (pathognomonic pattern):
- Oral enanthem: Erosions on tongue, buccal mucosa, hard palate — painful, with erythematous halo
- Cutaneous vesicles: Begin as pink macules/papules → 4–8 mm vesicles → oval "football-shaped" erosions with gray center and erythematous halo on the palms, soles, sides of hands/feet, buttocks
Complications: Mostly self-limiting. EV71 is associated with serious neurological complications — aseptic meningitis, encephalitis, acute flaccid paralysis, and potentially fatal brainstem encephalitis.
Diagnosis: Clinical; PCR or viral culture from vesicle fluid, throat, or stool for confirmation. CSF PCR if neurological involvement. — Fitzpatrick's Dermatology
6. Varicella (Chickenpox)
Virus: Varicella-zoster virus (VZV), HHV-3, α-herpesvirus.
Prodrome: 1–2 days of mild fever, malaise.
Exanthem: Begins on scalp/face → trunk → extremities. Hallmark: "dew drop on a rose petal" — clear vesicle on an erythematous base. Lesions progress: macule → papule → vesicle → pustule → crust within 24–48 hours. Characteristic finding of lesions in multiple stages simultaneously (pleomorphic) in any given area.
Distinguishing features from smallpox: Centripetal distribution (trunk > extremities), pleomorphic lesions (different stages), mucous membrane involvement.
Complications: Secondary bacterial infection, varicella pneumonia (adults, immunocompromised), cerebellar ataxia, encephalitis, Reye syndrome (with aspirin use), neonatal varicella (if maternal infection 5 days before to 2 days after delivery — high mortality without treatment).
7. CMV — Congenital Infection
Virus: Human Cytomegalovirus (HCMV, HHV-5), β-herpesvirus. Most common congenital viral infection (0.5–2% of live births in the USA).
Cutaneous findings:
- Petechiae/purpura from thrombocytopenia
- Blueberry muffin lesions (dermal erythropoiesis): dark-blue to violaceous papules (2–10 mm) present at birth, fading over 6 weeks. Histology: nucleated red cells + nonnucleated erythrocytes in the reticular dermis.
- Jaundice from hepatitis
Other sequelae: Sensorineural hearing loss (most common sequela — ~50% of symptomatic neonates), microcephaly, periventricular calcifications, chorioretinitis, intrauterine growth restriction. — Fitzpatrick's Dermatology
Comparison Table — Key Differentiators
| Feature | Measles | Rubella | Roseola | Parvovirus B19 | HFMD |
|---|---|---|---|---|---|
| Causative virus | Morbillivirus | Rubivirus | HHV-6B | Parvovirus B19 | CVA16/EV71 |
| Prodrome | 3–4 d fever, 3Cs | Mild fever, LAP | High fever 3–7 d | Fever, malaise | Low fever, sore mouth |
| Rash timing | Day 4–5 of fever | Day 1–3 | After fever breaks | After viremia clears | Day 2–4 |
| Rash morphology | Morbilliform, coalescing | Fine maculopapular | Rose-pink macules, halo | Slapped cheek → lacy | Oval vesicles, palms/soles |
| Spread direction | Cephalocaudal | Face → trunk (24h) | Neck/trunk | Face → extremities | Acral + oral |
| Pathognomonic sign | Koplik spots | — | Nagayama spots | Slapped cheek | Football-shaped oral erosions |
| Key complication | Pneumonia, SSPE | Congenital rubella | Febrile seizures | Aplastic crisis, hydrops | EV71 encephalitis |
| Enanthem | Koplik spots (buccal) | Forchheimer (palate) | Nagayama spots | None | Oral erosions |
Approach to the Morbilliform/Viral Exanthem Patient
When evaluating a morbilliform rash:
- Timing relative to fever: Rash with fever (measles, rubella, enterovirus) vs. rash after fever resolves (roseola, Kawasaki)
- Distribution: Cephalocaudal (measles) | Centripetal (varicella) | Acral (HFMD, parvovirus)
- Morphology: Vesicular/pleomorphic (varicella, HFMD) | Petechial (meningococcemia, RMSF — rule out first) | Maculopapular (most viral)
- Mucosal involvement: Koplik spots (measles), oral erosions (HFMD), Forchheimer spots (rubella)
- Lymphadenopathy pattern: Postauricular/suboccipital (rubella), generalized (EBV, CMV), mesenteric (adenovirus)
- Drug eruption exclusion — Viral exanthem vs. drug eruption is a common diagnostic dilemma; drug-induced morbilliform eruptions are the leading mimicker.
Sources: Fitzpatrick's Dermatology (Vols. 1–2); Dermatology 2-Volume Set, 5th ed.; Sherris & Ryan's Medical Microbiology, 8th ed.
Viral exanthems in er
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
petechial rash meningococcemia emergency dangerous viral exanthem differential
Reading File
Finding Sources
I now have strong Emergency Medicine–oriented content from Tintinalli's and Harrison's. Here is the EM-focused synthesis:
Viral Exanthems in the Emergency Department
The ER approach to viral exanthems is fundamentally a triage and diagnosis-by-exclusion task: benign viral rashes vastly outnumber dangerous ones, but the dangerous ones — meningococcemia, RMSF, TSS, Kawasaki — kill quickly and cannot be missed. The workflow must be "rule out the killers first."
Step 1 — The First Question: Does This Rash Blanch?
This is the single most important assessment in the ED.
| Blanching | Meaning | Urgency |
|---|---|---|
| Blanches (erythematous, maculopapular) | Vasodilation — blood in vessels; viral, drug, allergic | Low-moderate |
| Does NOT blanch (petechiae, purpura, ecchymoses) | Extravasated blood in dermis | EMERGENCY — do not delay workup |
Step 2 — Non-Blanching Rash: Rule Out Immediately Life-Threatening Causes
Any petechial or purpuric rash + fever is a medical emergency until proven otherwise.
Meningococcemia (Neisseria meningitidis)
- Begins as blanching maculopapular rash → rapidly progresses to non-blanching petechiae and purpura over hours
- Characteristic: palpable purpura in axilla, trunk, extremities
- Associated: high fever, toxic appearance, meningismus, hypotension (septic shock)
- Purpura fulminans = large confluent areas of hemorrhagic necrosis — indicates DIC and imminent death
- Action: Immediate blood cultures → IV ceftriaxone without waiting for LP if patient is unstable

Rocky Mountain Spotted Fever (RMSF) — Rickettsia rickettsii
- Classic triad: fever + headache + rash — but the triad is only present in ~60% at time of presentation
- Rash begins on wrists and ankles (acral) → spreads centripetally to trunk; starts as blanching macules → becomes petechial
- Critical: rash may be absent in the first 3 days (treatment must begin before rash appears)
- Action: Do not wait for serology (sensitivity is low in acute phase); treat empirically with doxycycline
Dengue Fever
- Maculopapular or petechial rash, thrombocytopenia, severe myalgia ("breakbone fever")
- Travel history to tropical/subtropical regions is key
- Dengue hemorrhagic fever → shock, bleeding diatheses
Viral Hemorrhagic Fevers (Ebola, Marburg, Lassa)
- Rare; history of travel to endemic regions is essential
- Petechiae, ecchymoses, mucosal hemorrhage + fever
- Immediate isolation and infectious disease consultation
Step 3 — Blanching Maculopapular Rash: Common Viral Exanthems in the ED
The "Rash and Fever Together vs. Rash After Fever" Rule
| Timing | Diagnosis to consider |
|---|---|
| Rash WITH fever | Measles, rubella, enterovirus, EBV, scarlet fever, drug |
| Rash AFTER fever resolves | Roseola (HHV-6), Kawasaki disease |
| Rash WITHOUT fever | Drug reaction, parvovirus B19 (slapped cheek stage) |
Measles (Rubeola) — ER Protocol Required
- Most infectious virus known; airborne transmission; infectious before symptoms begin
- ED action: Any patient with fever + cough + coryza + conjunctivitis → immediately place in airborne isolation (negative-pressure room or N95 mask)
- Koplik's spots on buccal mucosa (1 mm white lesions opposite lower molars) = pathognomonic — confirm before rash appears
- Morbilliform rash starts behind ears/hairline → cephalocaudal spread over 3 days
- ED management:
- Supportive; vitamin A (reduces pneumonia risk and mortality)
- Admit if: pneumonia, encephalitis, immunocompromised, severe malnutrition
- Mandatory reporting to local/state public health before discharge
- Log potential ED staff and patient exposures
- Offer MMR vaccination to unvaccinated contacts identified in the ED
- Serum measles IgM confirms; may be negative in first 3–4 days of rash → repeat or use PCR of urine/throat
"Because measles is so highly infectious, EDs should have protocols for identification of measles suspects at initial point of contact based on characteristic symptoms." — Tintinalli's Emergency Medicine
Rubella
- Mild illness; posterior auricular and suboccipital lymphadenopathy preceding rash by up to 7 days is the key clue
- Fine pink maculopapular rash, face → trunk, clears in 3 days; no significant cough
- Key ED concern: Identify pregnant contacts — first-trimester exposure carries >85% risk of congenital rubella syndrome (cataracts, deafness, congenital heart disease)
- Report to public health
Roseola (HHV-6B) — Exanthem Subitum
- Classic ED presentation: infant brought in for febrile seizure → by the time of the ED visit, fever has broken and the rose-colored truncal rash has appeared
- The temporal sequence is diagnostic: high fever 3–5 days → fever defervesces → rash appears
- Reassure parents: rash signifies resolution, not worsening
- No specific antiviral needed; manage febrile seizure per standard protocol
Parvovirus B19 (Erythema Infectiosum / Fifth Disease)
- Child with "slapped cheek" (confluent facial erythema with circumoral pallor) + lacy reticular rash on extremities
- Important ED considerations:
- Aplastic crisis in sickle cell, hereditary spherocytosis, thalassemia patients: can present with severe anemia, pallor, tachycardia → blood transfusion may be needed
- Hydrops fetalis if pregnant patient or pregnant contacts are exposed during first 20 weeks
- By the time the rash appears, the child is no longer infectious (viremia has resolved)
Hand-Foot-Mouth Disease (Coxsackievirus A16/EV71)
- Painful oral erosions + vesicles on palms/soles in a young child in summer/fall
- Key concern: Enterovirus 71 (EV71) can cause aseptic meningitis, encephalitis, acute flaccid paralysis — admit if neurological signs
- Check hydration status: mouth pain often leads to refusal to eat/drink → dehydration
- LP if meningism: CSF shows lymphocytic pleocytosis, normal glucose; PCR confirms
Varicella (Chickenpox)
- Pruritic vesicles in multiple stages simultaneously ("dew drop on a rose petal")
- ED concerns:
- Secondary bacterial infection (Group A strep, Staph aureus) — cellulitis, necrotizing fasciitis
- Varicella pneumonia in adults and smokers: bilateral interstitial infiltrates, hypoxia → admit, IV acyclovir
- Reye syndrome if aspirin given — never use ASA in children with varicella
- Neonatal varicella: maternal illness 5 days before to 2 days after delivery → 20–30% neonatal mortality without IV acyclovir
- Immunocompromised: IV acyclovir; disseminated varicella can be fatal
- Treatment: acyclovir (valacyclovir) within 24 hours of rash onset in adults; supportive in uncomplicated childhood cases
Dangerous Mimickers and Differential Diagnosis
| Condition | Key Differentiator in ED | Action |
|---|---|---|
| Drug eruption (morbilliform) | No enanthem, no URTI symptoms, new medication in past 1–14 days; pruritic | Discontinue drug; monitor for DRESS |
| DRESS syndrome | Facial edema, eosinophilia, internal organ involvement, fever | Admit, stop offending drug |
| SJS/TEN | Mucosal erosions (≥2 sites), skin detachment, Nikolsky sign | ICU, immediate dermatology |
| Kawasaki disease | Fever >5 days, conjunctival injection, lip erythema, strawberry tongue, desquamation of fingertips, LAP; rash appears after fever, not with it | Echocardiogram, IVIG + aspirin |
| Scarlet fever | Sandpaper rash, strawberry tongue, pharyngitis, Pastia lines in antecubital fossa | Penicillin |
| Toxic shock syndrome (TSS) | Diffuse macular erythroderma ("sunburn-like"), hypotension, multiorgan dysfunction | ICU, antibiotics, source control |
| Meningococcemia | Non-blanching, rapid progression, toxic | Immediate ceftriaxone |
ED Approach Algorithm — Fever + Rash
FEVER + RASH
│
├─ NON-BLANCHING? ──── YES ──→ EMERGENCY
│ • Blood cultures → ceftriaxone NOW
│ • Consider RMSF → doxycycline
│ • Consider dengue, VHF (travel hx)
│
└─ BLANCHING (maculopapular)?
│
├─ Toxic / unstable? → Consider TSS, Kawasaki, DRESS
│
├─ Timing: rash WITH fever
│ ├─ 3Cs + Koplik's → MEASLES (airborne isolation, report)
│ ├─ Mild, postauricular LAP → Rubella (check pregnancy)
│ ├─ Pharyngitis + sandpaper → Scarlet fever (penicillin)
│ └─ Oral erosions + acral vesicles → HFMD (EV71?)
│
├─ Timing: rash AFTER fever
│ ├─ Infant, truncal macules → Roseola (reassure)
│ └─ Fever >5 days, no other dx → Kawasaki (echo, IVIG)
│
├─ "Slapped cheek" + lacy rash → Parvovirus B19
│ (check CBC if hemolytic anemia; alert if pregnant)
│
└─ No fever, new medication → Drug eruption
(monitor for mucosal involvement → SJS/TEN risk)
Key ED Disposition Guidance
| Condition | Disposition |
|---|---|
| Uncomplicated viral exanthem (roseola, fifth disease, HFMD in child) | Discharge with return precautions |
| Measles | Usually discharge; mandatory public health report; airborne precautions until 4 days after rash onset |
| Varicella in adult / immunocompromised / pneumonia | Admit, IV acyclovir |
| EV71-associated HFMD with neuro signs | Admit |
| Any petechial rash + fever | Admit, urgent sepsis workup |
| Kawasaki suspected | Admit, echo, pediatric cardiology |
| TSS / SJS-TEN | ICU |
Sources: Tintinalli's Emergency Medicine: A Comprehensive Study Guide; Harrison's Principles of Internal Medicine 22nd ed. (2025); Fitzpatrick's Dermatology; Sherris & Ryan's Medical Microbiology 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.