Post partum sterilization
Reading File
Finding Sources
Finding Sources
Searching PubMed
postpartum sterilization tubal ligation
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple textbooks. Let me compile the full answer.
Postpartum Sterilization
Definition
Postpartum tubal ligation (PTL) refers to sterilization performed within 72 hours of delivery. It is the most convenient time to perform female sterilization because the enlarged uterus brings the fallopian tubes high into the abdomen, making them easily accessible.
Timing Options
Postpartum sterilization may be performed at three time points:
- Immediately during cesarean section - performed after delivery and uterine repair; adds only a slight prolongation of operating time and poses no additional significant risk
- Delayed 8-48 hours after vaginal delivery - allows elective fasting, equilibration of fluid shifts (especially if blood loss was a concern), and observation of the newborn
- Deferred (interval procedure) - performed 6+ weeks postpartum; interval tubal ligation as early as 6 weeks after delivery is equally effective
Sterilization is technically easier in the immediate postpartum period because of uterine enlargement and the elevated position of the tubes.
Importantly, PTL remains an elective procedure. Never assume that a patient who underwent emergency cesarean section (especially for fetal concern) still wishes to proceed with sterilization - consent must be reconfirmed.
Contraindications to PTL
- Maternal fever
- Pregnancy-related hypertension (preeclampsia/eclampsia)
- Uncontrolled diabetes mellitus
- Excessive blood loss during delivery
- Concern over viability or health of the newborn
Surgical Approach: Minilaparotomy
Minilaparotomy is the preferred and safest method in the postpartum period. Laparoscopy is not as safe in the immediate postpartum period due to the engorged pelvic vasculature and altered anatomy.
Technique Steps
- Drain the bladder by voiding immediately before surgery or by straight catheterization
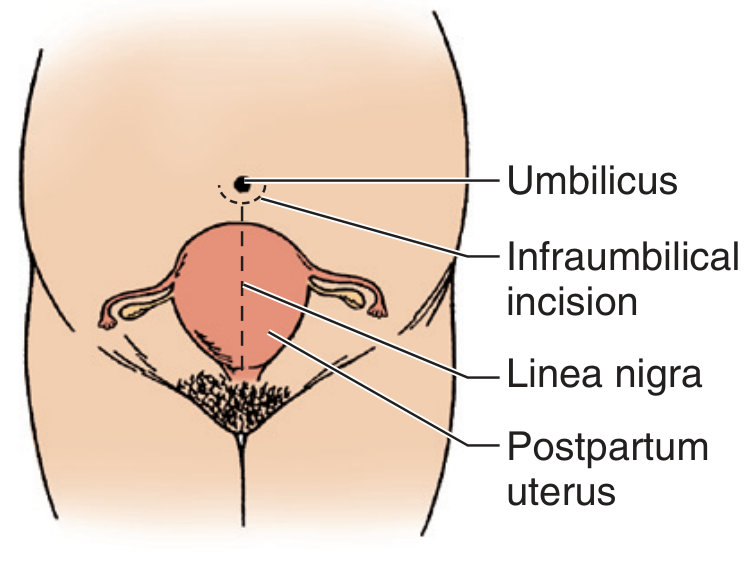
- Incision: Curved infraumbilical incision (4-5 cm), placed close to or within the umbilical crater - the enlarged postpartum uterus brings the tubes up to this level
- Entry: Blunt dissection with Kelly clamps to enter the peritoneal cavity; uterus is gently pushed to one side to rotate adnexal structures into view
- Tube identification: Babcock clamps are used to identify the fallopian tube, which is characteristically swollen and engorged in the postpartum state. Each tube must be followed to its fimbriated end and the ovary identified to confirm correct structure
- Caution with mesosalpinx: Vessels within the mesosalpinx are hugely dilated postpartum - extremely gentle traction is required to avoid profuse bleeding
- Tubal occlusion: Perform as for interval sterilization (see below). If the tube cannot be delivered through the incision, clips may be applied in situ
- Closure: Layered closure, ensuring definitive fascial closure
Tubal Occlusion Techniques
The following methods are used (listed with key features):
| Technique | Description | Notes |
|---|---|---|
| Modified Pomeroy (most common for PTL) | Loop of tube ligated at base with absorbable suture, then excised | Favored for fragile postpartum mesosalpinx; quick and hemostatic |
| Parkland (Partial salpingectomy) | Midportion of tube ligated with two separate absorbable sutures, then excised | Also called "separate sutures technique" |
| Irving method | Midportion excised; proximal stump buried into uterine wall | Extremely low failure rate; more technically demanding |
| Uchida method | Saline-epinephrine injected submucosally; mucosal segment excised; proximal stump buried | >20,000 cases with no reported pregnancies |
| Clips (Hulka, Filshie) | Mechanical occlusion | Used when tube cannot be delivered; Filshie clip has largely supplanted Hulka clip |
| Silastic band (Falope ring) | Ischemic necrosis of a loop | More reversible than electrocautery |
| Bipolar electrocoagulation | 3 cm of tube coagulated at midsthymic portion | Requires generator delivering ≥25 W into 100 Ω; if fragment cannot be confirmed, coagulation may be incomplete |
Pomeroy and partial salpingectomy: failure rates of 1-4 per 1,000 cases. Irving and Uchida: failure rates are exceedingly rare.
Anesthesia for Postpartum Sterilization
A key concern is the persistent risk of pulmonary aspiration in the immediate postpartum period. Gastric volume and pH normalize within 24 hours of delivery, but most clinicians treat these patients as "full stomach" cases until that time.
If Epidural was Used for Labor
- The epidural catheter can be left in place for up to 48 hours
- Allow an elective fasting period before proceeding
- A T4-T5 sensory level is usually needed for a pain-free experience; lower levels (T10) may fail to prevent visceral traction pain
If No Prior Anesthesia (Vaginal Delivery without Block)
Regional anesthesia is preferred for minilaparotomy (over general), given aspiration risk:
- Spinal is often preferred over epidural for speed, density, and reliability
- Bupivacaine 8-12 mg or lidocaine 60-75 mg
- Postdural puncture headache risk is ~1% with 25-gauge pencil-point needle
- Epidural: lidocaine 1.5-2% or chloroprocaine 3%, 15-30 mL
- Note: regional anesthetic dose requirements return to normal within 24-36 hours after delivery
General anesthesia is required for laparoscopic fulguration (not recommended in the immediate postpartum period anyway):
- Rapid-sequence induction + endotracheal intubation
- Premedication: H2 blocker (ranitidine), sodium citrate, or metoclopramide
- Extubate only when awake with intact airway reflexes
- Succinylcholine duration is modestly prolonged (reduced plasma cholinesterase persists postpartum)
- Rocuronium duration is also prolonged; atracurium/cisatracurium are not affected
- Avoid excessive volatile agents (risk of uterine relaxation and postpartum hemorrhage)
- Breastfeeding can resume immediately postanesthesia (the old "pump and dump" advice is outdated)
Complications and Failure
- Complication rate for postpartum minilaparotomy: approaches that of interval sterilization, generally < 3%
- Average tubal sterilization failure rate: ~1 in 250 at 1 year
- Postpartum and postabortion sterilization is slightly less effective than interval sterilization
- Ectopic pregnancy risk: postpartum partial salpingectomy and unipolar coagulation have the lowest rates of ectopic pregnancy after sterilization failure (Berek & Novak)
Reversal and Regret
- 1-2% of women seek reversal after sterilization
- Of these, only 30-70% are candidates for reversal surgery (range depends on original method)
- Pregnancy occurs in approximately 50% of those who undergo reversal
- Reversal is most successful when < 3 cm of tube was damaged or removed, and when the isthmic portion was preserved (non-electrocautery techniques are most reversible)
Risk Factors for Regret (Counsel Before Proceeding)
- Marital disharmony at the time of sterilization (remarriage is the reason in 90% of reversal requests)
- Age < 30 years at time of sterilization
- Sterilization chosen due to financial, health, or emotional difficulties
- Regret may be slightly more prevalent after postpartum sterilization specifically
vs. Interval Sterilization
| Feature | Postpartum (PTL) | Interval (6+ weeks later) |
|---|---|---|
| Technical ease | Easier (enlarged uterus) | Standard difficulty |
| Access | Infraumbilical minilaparotomy | Suprapubic minilaparotomy or laparoscopy |
| Anesthesia risk | Slightly higher (aspiration) | Lower |
| Efficacy | Slightly lower | Slightly higher |
| Laparoscopy safety | Less safe (engorged vasculature) | Preferred route |
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. - Chapter 152
- Berek & Novak's Gynecology - Chapter 14
- Morgan and Mikhail's Clinical Anesthesiology, 7th ed. - Chapter on Obstetric Anesthesia
Create a summary document on postpartum sterilization for patient counseling
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Running Command
The document is valid and ready. Here's your file:
Postpartum Sterilization Patient Counseling
Word Document · DOCX
The document is formatted as a professional patient counseling guide (~17 KB) and includes:
Structure and Content:
| Section | What's Inside |
|---|---|
| Title block | Document title, subtitle, and introductory note |
| What is Postpartum Sterilization? | Plain-language definition and permanence warning |
| When Can it Be Done? | Three timing options (C-section, within 48h, 6-week interval) |
| When It Cannot Be Done | Contraindications in bullet form |
| How is it Performed? | Step-by-step overview + techniques table (Pomeroy, Parkland, Irving, Uchida, clips) |
| Effectiveness | Failure rates; ectopic pregnancy callout |
| Anesthesia Options | Epidural/spinal/general with plain-language explanation |
| Risks & Complications | Formatted table with frequency and details |
| Permanence & Regret | Reversal success rates, risk factors for regret |
| Alternatives | IUD, implant, injectable, vasectomy comparison table |
| Recovery | Post-procedure care instructions |
| Questions to Ask | Checklist of key questions for the patient |
| Consent Warning | Right to withdraw consent callout |
| Acknowledgment / Signature Block | Patient name, DOB, date, signature, witness, doctor fields |
Design: Teal/orange colour scheme, shaded callout boxes for warnings, alternating-row tables, header/footer with page numbers, and clinical-but-accessible language throughout.
This is a shared conversation. Sign in to Orris to start your own chat.