About metformin
Reading File
Searching the Web
metformin mechanism of action clinical uses 2025
Finding Sources
Searching PubMed
metformin type 2 diabetes
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough answer.
Metformin - Complete Overview
Drug Class & Background
Metformin is a biguanide oral antidiabetic drug and the most widely prescribed antidiabetic medication in the world. It has been used for over 30 years for type 2 diabetes mellitus (T2DM). - Goldman-Cecil Medicine, p. 985
Mechanism of Action
Metformin works through several interconnected pathways:
1. AMPK Activation (Primary Mechanism)
Metformin activates AMP-activated protein kinase (AMPK) by activating an upstream kinase, LKB1. Activated AMPK then:
-
Phosphorylates and inactivates acetyl-CoA carboxylase (reducing fatty acid synthesis and increasing fatty acid oxidation)
-
Inhibits HMG-CoA reductase (reducing cholesterol biosynthesis)
-
Enhances glucose uptake by skeletal muscle
-
Basic Medical Biochemistry - A Clinical Approach, 6e, p. 1226
2. Suppression of Hepatic Gluconeogenesis (Key Glucose-Lowering Effect)
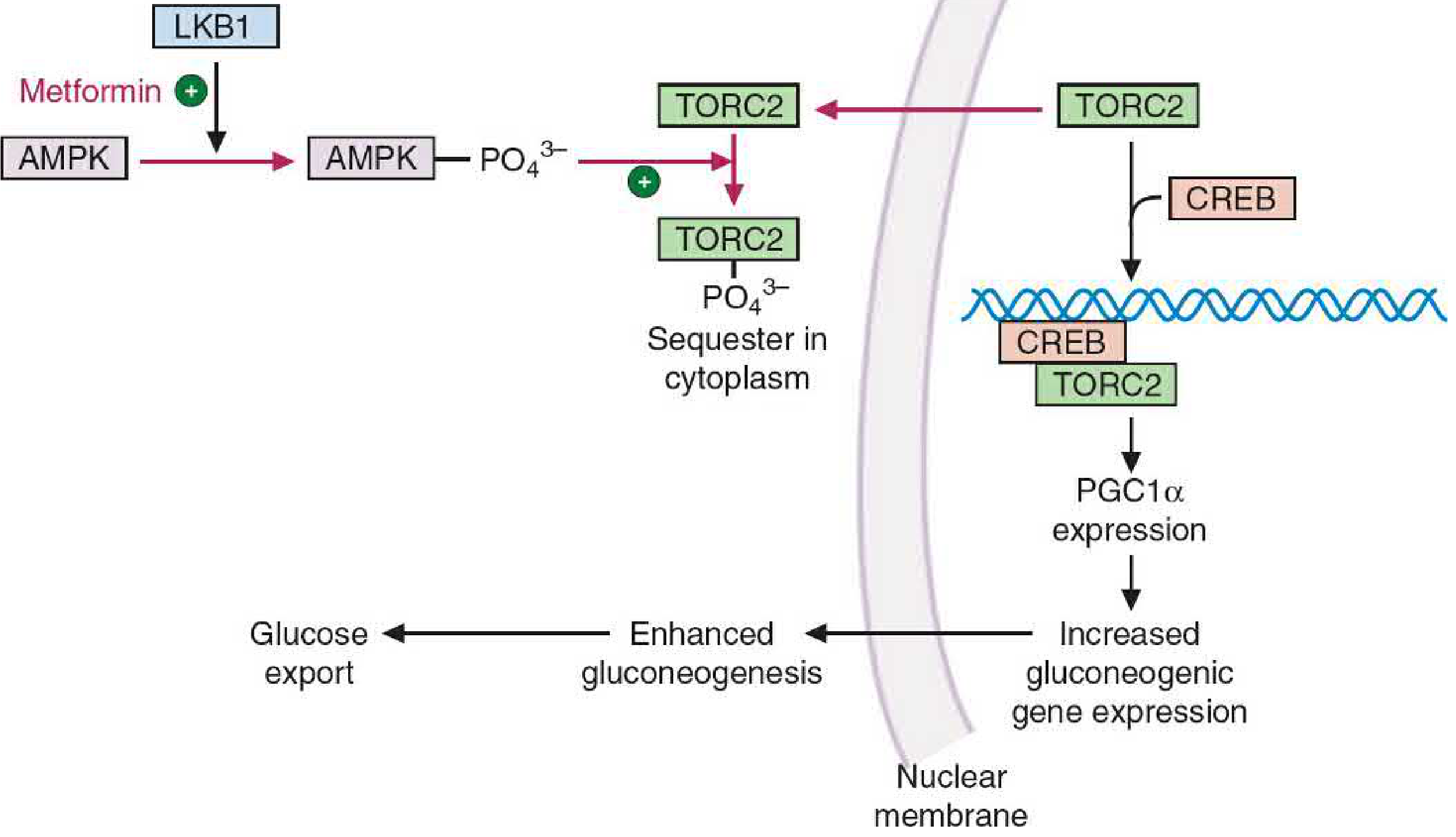
In insulin-resistant states, glucagon-driven cAMP elevates CREB transcription, which pairs with TORC2 to upregulate PGC1alpha - a coactivator that drives expression of gluconeogenic enzymes (glucose-6-phosphatase, PEPCK). Metformin-activated AMPK phosphorylates TORC2, sequestering it in the cytoplasm and blocking this transcriptional cascade, thereby suppressing hepatic glucose output. - Basic Medical Biochemistry - A Clinical Approach, 6e
3. Additional Mechanisms
- Inhibition of mitochondrial glycerol-3-phosphate dehydrogenase (reduces glycerol-to-glucose conversion - an AMPK-independent route) - Goodman & Gilman's
- Reduced intestinal glucose absorption
- Increased GLP-1 secretion from the GI tract
- Favorable changes to gut microbiota composition
Therapeutic Uses
| Indication | Notes |
|---|---|
| Type 2 Diabetes (first-line) | Preferred initial monotherapy per all major guidelines |
| Prediabetes / prevention | Reduces progression to T2DM |
| Polycystic ovary syndrome (PCOS) | Improves insulin sensitivity, restores ovulation |
| Weight management | Weight-neutral to mildly weight-reducing |
| Cardiovascular risk reduction | Reduces CV events and mortality in obese T2DM patients (UKPDS data) |
Efficacy
- Reduces HbA1c by 1.0-1.5% (11-16 mmol/mol)
- Does not cause hypoglycemia when used as monotherapy (no insulin secretagogue effect)
- Mild reduction in body weight
- Does not increase insulin secretion - Goldman-Cecil Medicine, p. 985
Dosing
- Start: 500 mg once or twice daily with meals (slow titration minimizes GI side effects)
- Maximum dose: 2,550 mg/day
- Available as immediate-release (IR) and extended-release (ER) formulations
- Renal dose adjustment required; withhold if eGFR < 30 mL/min
Adverse Effects
| Effect | Detail |
|---|---|
| GI symptoms | Nausea, bloating, diarrhea (most common; start low, titrate slowly) |
| Lactic acidosis | Rare (0.084 cases/1,000 patient-years) but mortality up to 50%; most common in patients with contraindications |
| Vitamin B12 deficiency | Long-term use impairs B12 absorption; periodic monitoring recommended |
| Peripheral neuropathy | May worsen due to B12 depletion |
- Campbell Walsh Wein Urology, p. 1469; Goldman-Cecil Medicine, p. 989
Contraindications & Precautions
- eGFR < 30 mL/min - drug accumulates, raising lactic acidosis risk
- Iodinated contrast agents - hold metformin before/during procedures (risk of transient renal impairment causing accumulation); restart 48 hours after if renal function is stable
- Hepatic failure - reduces lactate clearance, predisposing to lactic acidosis
- Heart failure with hemodynamic compromise, sepsis, severe hypoxia
Pharmacokinetics
- Absorption: Oral, absorbed from small intestine
- Distribution: Primarily cytosolic; < 10% enters mitochondria
- No hepatic metabolism - excreted unchanged by renal filtration
- Half-life: ~6 hours (plasma); ~17 hours (blood, due to erythrocyte accumulation)
Recent Evidence (2024-2025)
Recent systematic reviews highlight two emerging areas:
- Metformin + exercise combination shows superior glucose control vs. either alone in patients with abnormal glycaemia (Zhao T et al., Br J Sports Med, 2024 - PMID 39242178).
- Dementia risk: A 2025 meta-analysis in JAMA Neurology examined whether cardioprotective glucose-lowering agents (including metformin) reduce dementia risk - evidence remains under active investigation (Seminer A et al., JAMA Neurol, 2025 - PMID 40193122).
Summary Table
| Property | Detail |
|---|---|
| Class | Biguanide |
| Route | Oral |
| MOA | AMPK activation → suppress hepatic gluconeogenesis & lipogenesis; increase muscle glucose uptake |
| HbA1c reduction | 1.0-1.5% |
| Hypoglycemia risk | None (monotherapy) |
| Weight effect | Neutral to mild reduction |
| Key safety concern | Lactic acidosis (rare but serious) |
| Renal cutoff | Hold if eGFR < 30 mL/min |
| Long-term monitoring | Vitamin B12 levels |
This is a shared conversation. Sign in to Orris to start your own chat.