Barbiturate poisoning narayana Reddy forensic medicine in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a complete, detailed answer. Let me compile the full response from Narayana Reddy's textbook.
Barbiturate Poisoning
The Essentials of Forensic Medicine and Toxicology - K.S. Narayana Reddy (36th Edition, 2026)
Introduction
Barbituric acid was first detected by Adolf Baeyer in 1864, and Phenobarbitone was synthesized in 1912. Barbiturates are derivatives of Barbituric acid (2-4-6 trioxohexahydropyrimidine), used as sedative-hypnotics to this day.
Chemical Class: Sedative-hypnotics / CNS depressants
Uses
- Sedative-hypnotics
- Pre-anesthetic medication
- Seizure disorders (epilepsy)
Pharmacokinetics (Route of Absorption, Metabolism, and Excretion)
- Most sedative-hypnotics are administered orally; intravenous mode is reserved for seizure control or induction/maintenance of general anesthesia.
- Long-acting sedative-hypnotics have a plasma half-life of up to 80 hours.
- Most are metabolized to alcohols, phenols, and ketones, excreted in urine.
- Phenobarbitone is excreted ~25% unchanged in urine; the rest is metabolized slowly in the liver.
Adverse Effects (Therapeutic Use)
- Residual depression ("hangover" effect)
- Paradoxical excitement in the elderly
- Localized hypersensitivity - eyes, lips, subcutaneous tissues
- Synergy (Synergia) - with ethyl alcohol and antihistaminics (potentiation)
- Contraindicated in acute/intermittent porphyria - since the end product of barbiturate metabolism (phenol derivatives) worsens porphyria
Toxic Effects / Clinical Signs of Acute Poisoning
(1) CNS
- Confusion, ataxia, slurred speech, lethargy, headache, nystagmus
- Initial pupil constriction → later dilatation (as coma deepens)
- CNS depression → coma, shock
(2) Respiratory System
- Primary cause of death - respiratory center depression
- Persons with COPD or chronic pulmonary disease are more susceptible
- Slow, shallow breathing → decreased minute volume → terminally Cheyne-Stokes breathing → respiratory arrest
(3) Cardiovascular System (CVS)
- Cardiovascular center depression
- Decreased cardiac output
- Patients with CCF are more susceptible
- Hypotension, cold clammy skin
(4) Hypothermia
- Hypothermia, hypotonia, hypotension, cold clammy skin
(5) Gastrointestinal Tract (GIT)
- Decreased peristalsis in deeply comatose cases - can endanger life
(6) Kidney
- Decreased renal perfusion due to hypotension
- Scanty urination, urinary incontinence
(7) Cutaneous Bullae - Barbiturate Bullae (Barb Bullae) [PATHOGNOMONIC]
- Subcutaneous erythematous or hemorrhagic bullae/blisters
- Commonly seen over: shin, knee, hands, or any pressure area
- Neonatal bullae may appear in newborns of mothers who abused sedative-hypnotics, up to 2 weeks after delivery
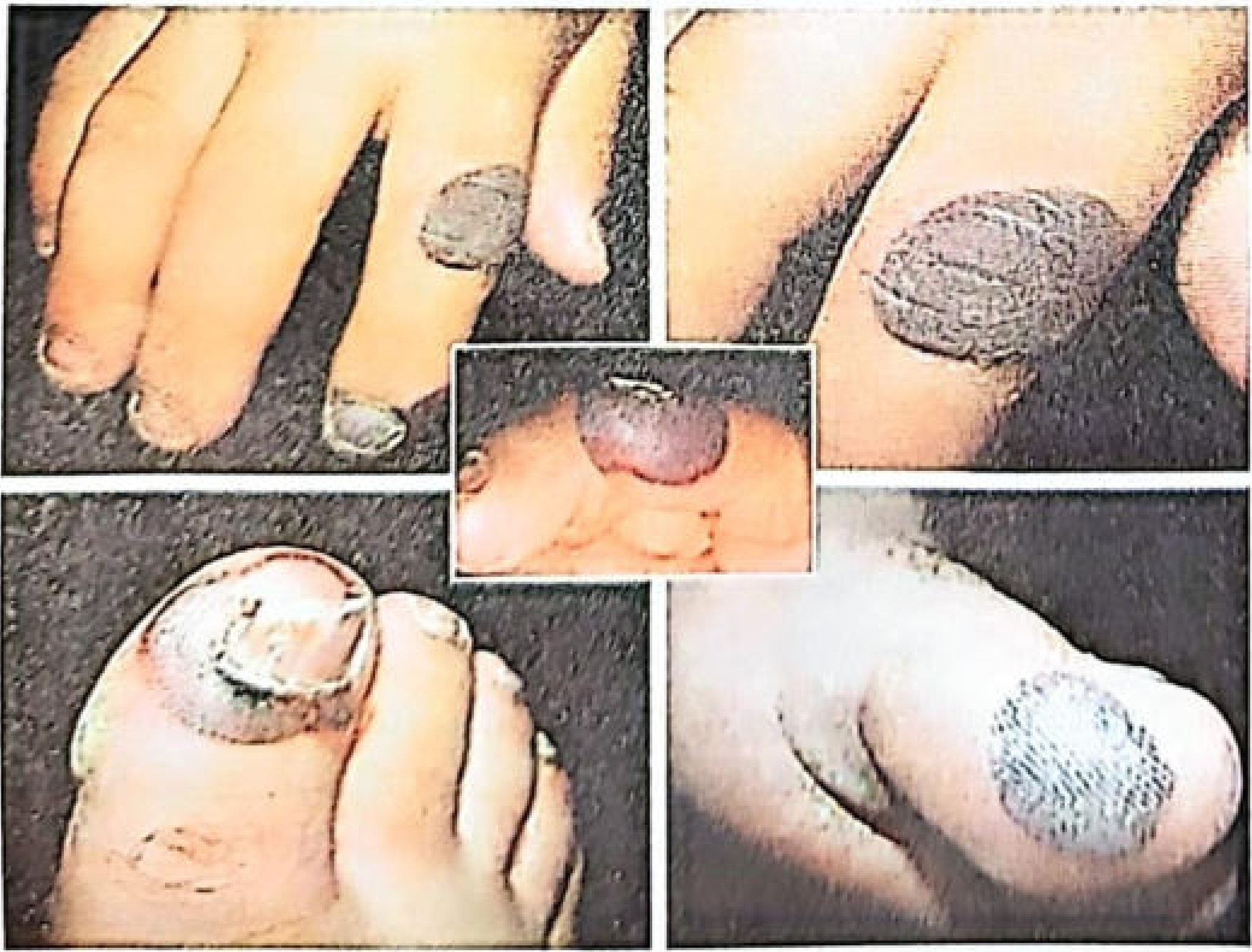
Fig. 31.2: Barbiturate bullae on fingers and toes.
Fatal Dose and Lethal Blood Levels
| Parameter | Value |
|---|---|
| Fatal Dose | 6-10 grams (highly variable) |
| Lethal Blood Level (intermediate-acting) | 3-4 mg% |
| Lethal Blood Level (Phenobarbitone) | 8-15 mg% |
Treatment of Acute Barbiturate / Sedative-Hypnotic Poisoning
(1) Stomach Wash (Gastric Lavage)
- Indicated only in conscious patients
- Solution: KMnO4 4% (potassium permanganate) with activated charcoal or tannic acid - leave some quantity in the stomach, then suction
- Magnesium sulphate solution left in the stomach causes purgation and prevents further absorption
- Both are effective up to 24 hours of ingestion
(2) Emesis - CONTRAINDICATED
- Emesis (vomiting) is contraindicated as the gag reflex is depressed - risk of aspiration and asphyxia
(3) Specific Antidotes
- No specific antidote available
- Earlier literature mentioned analeptics (CNS stimulants) as antidotes - no longer recommended
(4) Supportive Treatment
- Maintain airway, cardiac output, adequate urinary excretion
- Antibiotics to prevent secondary infection
(5) Nursing Care
- Proper nursing to prevent bed sores
- Catheterization for urinary management
Autopsy Findings (Postmortem Appearances)
- Signs of asphyxia: Congestion, cyanosis, petechial hemorrhages
- Barbiturate bullae/blisters (characteristic finding)
- Blood: Dark-blue, deoxygenated, liquid blood
- Stomach (Fundus): Thickened, granular, and hemorrhagic
- Brain (in delayed death):
- Bilateral symmetrical necrosis of globus pallidus and corpus callosum
- Focal generalized necrosis of cerebral and cerebellar areas
Laboratory Diagnosis
| Test | Details |
|---|---|
| Dille-Koppanyi Test | Add 2 drops of 1% cobalt acetate in methanol + 1 drop of 5% isopropylamine in methanol to suspected material → Lavender color develops if barbiturates are present |
| Colorimetric methods | Spectrophotometric analysis |
| HPLC and GC-MS | Confirmatory gold-standard tests |
Chronic Barbiturate Poisoning
Usually due to prolonged medication (e.g., epilepsy) or use as a recreational substance.
Signs and Symptoms (Similar to Alcohol Intoxication):
-
Physical deterioration:
- Ataxia, cerebral dysfunction, dysarthria, hypertonia
- Parkinsonian tremors
-
Social deterioration:
- Mood, behavior, and intellectual dysfunction
-
Barbiturate Abstinence Syndrome (Withdrawal Syndrome):
- Physical and psychological dependence - abrupt cessation causes withdrawal
- Symptoms: visual disturbance, anxiety, dizziness, insomnia, nausea, vomiting, restlessness, tremors, convulsions
Medico-Legal Importance
-
Suicide: Barbiturates are a well-known drug of suicide, especially among patients on treatment, addicts, and medical professionals with drug knowledge.
-
Drug of Euthanasia: In Switzerland, barbiturates are legally used for oral suicidal consumption by an association called the "Exit Association".
-
Drugs of Abuse (Recreational Use):
- Amobarbital (Amytal)
- Pentobarbital (Nembutal)
- Secobarbital (Seconal)
- These are known by various street/nick names in the world of addicts.
-
Narcoanalysis (Truth Serum):
- Sodium Amytal and Sodium Pentothal (thiopental) are used as "truth serum" drugs
- Metered doses produce desired controlled narcosis
- This narcoanalysis is also called the "Amytal Interview"
-
Judicial Execution:
- The following sequential drug combination is used for the death sentence:
- Sodium thiopental (CNS depression)
- Pancuronium bromide (respiratory muscle paralysis)
- Potassium chloride (cardiac arrest)
- The following sequential drug combination is used for the death sentence:
Summary Table (Quick Revision)
| Feature | Details |
|---|---|
| Drug class | Barbituric acid derivatives |
| Mechanism of death | Respiratory center depression |
| Pathognomonic sign | Barbiturate bullae (Barb bullae) |
| Fatal dose | 6-10 g (variable) |
| Lethal blood level | 3-4 mg% (intermediate); 8-15 mg% (phenobarbitone) |
| Antidote | None specific |
| Gastric lavage | KMnO4 4% + activated charcoal; MgSO4 |
| Emesis | Contraindicated |
| Lab test (chemical) | Dille-Koppanyi test → Lavender color |
| PM brain finding | Bilateral necrosis of globus pallidus + corpus callosum |
| Medico-legal uses | Suicide, euthanasia, narcoanalysis, judicial execution |
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - K.S. Narayana Reddy, Chapter 31, pp. 548-549
This is a shared conversation. Sign in to Orris to start your own chat.