Tb meningitis
Reading File
Finding Sources
Searching PubMed
"tuberculous meningitis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is a structured overview of tuberculous meningitis (TBM):
Tuberculous Meningitis (TBM)
Epidemiology
TBM parallels the prevalence of systemic tuberculosis. Incidence rose substantially from ~1985 in the United States, partly driven by HIV. In sub-Saharan Africa and other developing regions, TB is ~25× more frequent than in the US, again largely due to HIV. TBM was formerly more common in young children; now it predominantly affects adults in high-income countries. (Adams and Victor's Principles of Neurology, 12th Ed.)
Pathogen & Pathogenesis
Causative agent: Mycobacterium tuberculosis (rarely M. bovis, M. avium, M. kansasii, M. fortuitum post-neurosurgery).
Two-stage pathogenesis:
- Hematogenous seeding of the meninges/subpial regions → formation of tubercles (Rich focus)
- Rupture of one or more tubercles → discharge of bacilli into the subarachnoid space → intense inflammatory response
The process is a true meningoencephalitis — unlike pyogenic meningitis, it penetrates the pia and ependyma into underlying brain parenchyma. (Adams and Victor's)
Pathology
- Basal predominance: thick gelatinous exudate fills the pontine and interpeduncular cisterns, extending around the medulla, optic chiasm, and temporal lobes
- Microscopically: meningeal tubercles with central caseation, epithelioid and giant cells, lymphocytes, plasma cells
- Complications of exudate:
- Cranial nerve entrapment (especially CN III, VI, VII, VIII)
- Vasculitis → arterial occlusion → cerebral infarction (circle of Willis branches)
- Hydrocephalus (basal cistern obstruction — communicating; aqueduct blockage — obstructive)
- Spinal radiculopathy from circumferential cord exudate
Clinical Features
Onset: Subacute over 1–2 weeks (key distinguishing feature from acute bacterial meningitis)
| Feature | Detail |
|---|---|
| Fever (low-grade), malaise, headache | >50% of cases |
| Neck stiffness, Kernig/Brudzinski signs | ~75% of cases |
| Cranial nerve palsies (ocular > facial) | ~20% of cases at presentation |
| Papilledema | With raised ICP |
| Confusion, lethargy | Common |
| Focal neurologic deficit | From hemorrhagic infarction |
| Hyponatremia | SIADH or adrenal TB |
| Seizures | Especially in children |
In infants/young children: apathy, hyperirritability, vomiting, seizures; neck stiffness may be absent.
Evidence of active TB elsewhere (usually lungs) is found in ~2/3 of patients. In adults, TBM is now seen predominantly in HIV patients, alcoholics, and immigrants from high-burden regions. (Adams and Victor's, p. 728)
MRI Appearance
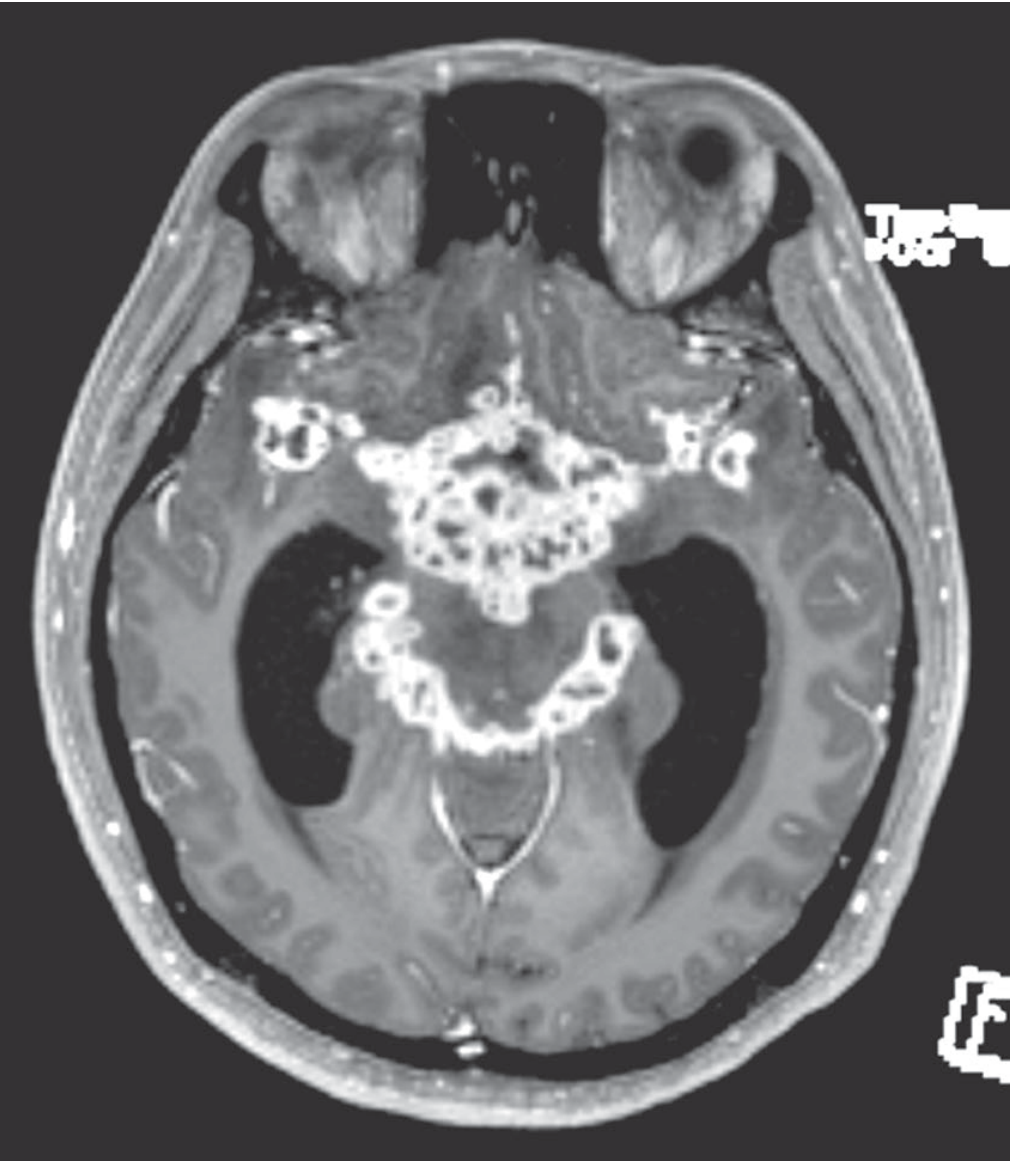
Gadolinium-enhanced MRI showing intense enhancement of the basal meninges (multiple abscesses) with hydrocephalus and cranial nerve palsies. — Adams and Victor's, Figure 31-3
Key MRI/CT findings:
- Basal meningeal enhancement (hallmark)
- Hydrocephalus
- Tuberculomas (ring-enhancing lesions)
- Deep cerebral infarcts (lenticulostriate/perforating artery territory)
- MR/CT angiography may show vasculitic arterial occlusions
CSF Analysis
| Parameter | Finding |
|---|---|
| Pressure | Elevated |
| Cell count | 50–500 WBC/mm³, lymphocyte predominance (early PMN possible) |
| Protein | 100–200 mg/dL (very high if spinal block) |
| Glucose | Low (<40 mg/dL); fall may be delayed several days |
| Chloride | Often reduced |
| Serum sodium | Often low (SIADH) |
Diagnostic tests on CSF:
| Test | Performance |
|---|---|
| Ziehl-Neelsen AFB smear | Sensitivity 10–50% (volume-dependent) |
| Culture (gold standard) | ~50% positive; takes 3–8 weeks |
| PCR/NAAT | Sensitivity ~80%, false-positive rate ~10%; multiplex PCR superior |
| ADA (adenosine deaminase) | Elevated in TBM; useful as rule-in test (levels >10 U/L) |
| Dot-ELISA (antigen/antibody) | ~86% sensitivity in suspected TBM |
| Tuberculin skin test | Positive in ~85% children, only 40–60% of adults |
| IGRA (interferon-gamma release assay) | Highly sensitive, ~90% specific; can be performed on CSF |
Key point: If TBM is strongly suspected and cryptococcosis/fungal/neoplastic meningitis have been reasonably excluded, do not wait for culture results — start treatment empirically. (Adams and Victor's, p. 729)
Staging (British Medical Research Council / MRC Grading)
| Stage | Features |
|---|---|
| Stage I (early) | Conscious, no focal deficit, no hydrocephalus |
| Stage II (moderate) | Altered consciousness (GCS 10–14), focal neurologic signs |
| Stage III (severe) | Coma (GCS ≤9), dense neurologic deficit |
Outcome strongly correlates with stage at initiation of therapy.
Treatment
Antituberculous Therapy
Intensive phase (first 2 months): Four-drug regimen
| Drug | Adult Dose | Key Toxicity |
|---|---|---|
| Isoniazid (INH) | 5 mg/kg/day (max 300 mg) | Hepatitis, peripheral neuropathy |
| Rifampin (RMP) | 10 mg/kg/day adult; 15–20 mg/kg child (max 600 mg) | Hepatitis, drug interactions |
| Pyrazinamide (PZA) | 20–35 mg/kg/day (weight-based dosing) | Hepatotoxicity, hyperuricemia |
| Ethambutol (EMB) | 15–25 mg/kg/day | Optic neuropathy (dose-dependent) |
- Add pyridoxine 50 mg/day with INH to prevent neuropathy
- Alternative intensive regimen: INH + PZA + high-dose RMP + moxifloxacin
Continuation phase: INH + RMP for the remaining duration
Total duration: 9–12 months for drug-sensitive TBM (standard 6-month pulmonary regimens are insufficient for CNS TB)
Corticosteroids
Adjunctive dexamethasone is standard of care — reduces inflammation, cerebral edema, and vasculitis, decreasing mortality and severe disability.
- Starting dose: 0.15 mg/kg IV dexamethasone, then taper over 6–8 weeks
- Benefit proven in both HIV-negative and (to a lesser degree) HIV-positive patients
HIV Co-infection
- Start ART within 2 weeks of antituberculous therapy
- Use caution regarding immune reconstitution inflammatory syndrome (IRIS)
- Drug interactions between rifampin and antiretrovirals require careful selection (prefer efavirenz-based regimens or dolutegravir with adjusted dosing)
Drug Resistance
- Rising rates of MDR-TB require testing and use of second-line agents (ethionamide, fluoroquinolones, linezolid, bedaquiline)
- From regions with high INH resistance: add ethionamide as fifth drug
Neurosurgical Interventions
- Hydrocephalus: ventriculoperitoneal (VP) shunt or external ventricular drainage
- In advanced disease, up to 25% of patients require neurosurgical procedures (ROSEN's Emergency Medicine)
- Tuberculomas: antituberculous therapy usually results in resolution (see MRI before/after)
Complications
- Cerebral infarction (stroke)
- Obstructive or communicating hydrocephalus
- Cranial nerve palsies
- Seizures / epilepsy
- Spinal cord involvement (tuberculous myeloradiculitis)
- Pott's disease (vertebral TB with cord compression)
- SIADH / hyponatremia
- Adrenal insufficiency
Prognosis
TBM leads to severe disability or death in roughly 50% of cases. Outcome depends on:
- Age and comorbidities
- MRC stage at presentation
- Time to diagnosis and treatment
- Drug resistance
- HIV status (ROSEN's Emergency Medicine, p. 2268)
Sources: Adams and Victor's Principles of Neurology 12th Ed. | ROSEN's Emergency Medicine | Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.