Antihypertensive drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive response. Here is the full guide on antihypertensive drugs:
Antihypertensive Drugs
Blood Pressure Physiology (Why Drugs Work)
Arterial blood pressure = Cardiac Output × Peripheral Vascular Resistance. Most antihypertensive drugs act by reducing one or both of these components.
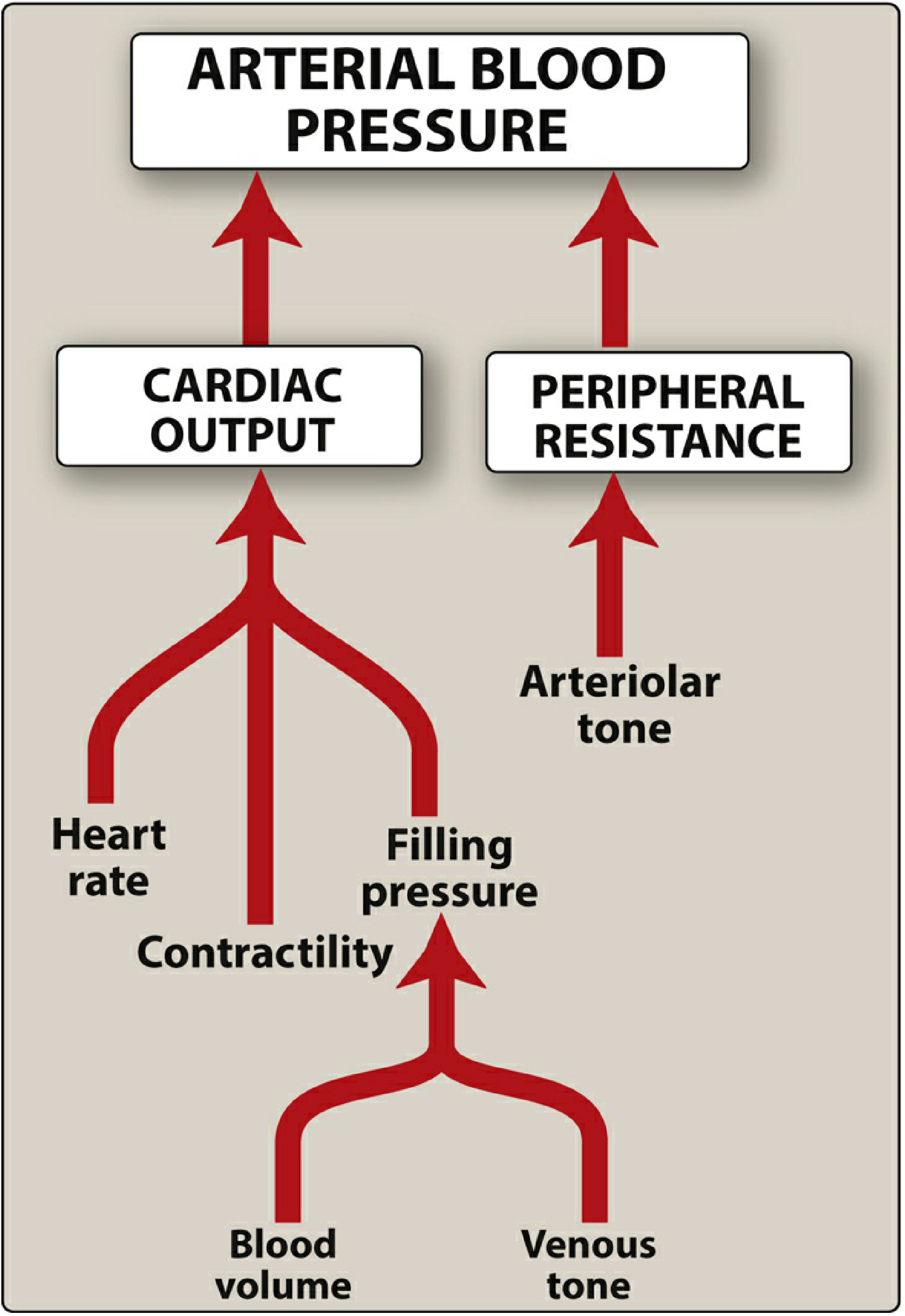
Two major regulatory systems control blood pressure:
- Sympathetic nervous system - via baroreflexes and adrenoceptors
- Renin-Angiotensin-Aldosterone System (RAAS) - controls sodium retention and vascular tone
Classification of Antihypertensive Drugs
BP Classification (ACC/AHA)
| Category | Systolic | Diastolic | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | or | <80 |
| Stage 1 Hypertension | 130-139 | or | 80-89 |
| Stage 2 Hypertension | ≥140 | or | ≥90 |
Drug Classes
1. DIURETICS
Mechanism: Lower blood pressure primarily by depleting body sodium stores. Initially reduce blood pressure by reducing blood volume and cardiac output. After 6-8 weeks, cardiac output returns toward normal while peripheral vascular resistance declines.
Types:
- Thiazides (hydrochlorothiazide, chlorthalidone) - first-line, effective 10-15 mmHg reduction
- Loop diuretics (furosemide) - used in heart failure + hypertension
- Potassium-sparing (spironolactone, eplerenone) - mineralocorticoid receptor antagonists; useful in resistant hypertension
Key points:
- Thiazides are a reasonable first step, especially in elderly
- In severe hypertension, diuretics are used with sympathoplegics and vasodilators to control sodium retention
- ADRs: Hypokalemia, hyperglycemia, hyperuricemia (more relevant in elderly given higher rates of arrhythmias, DM, gout)
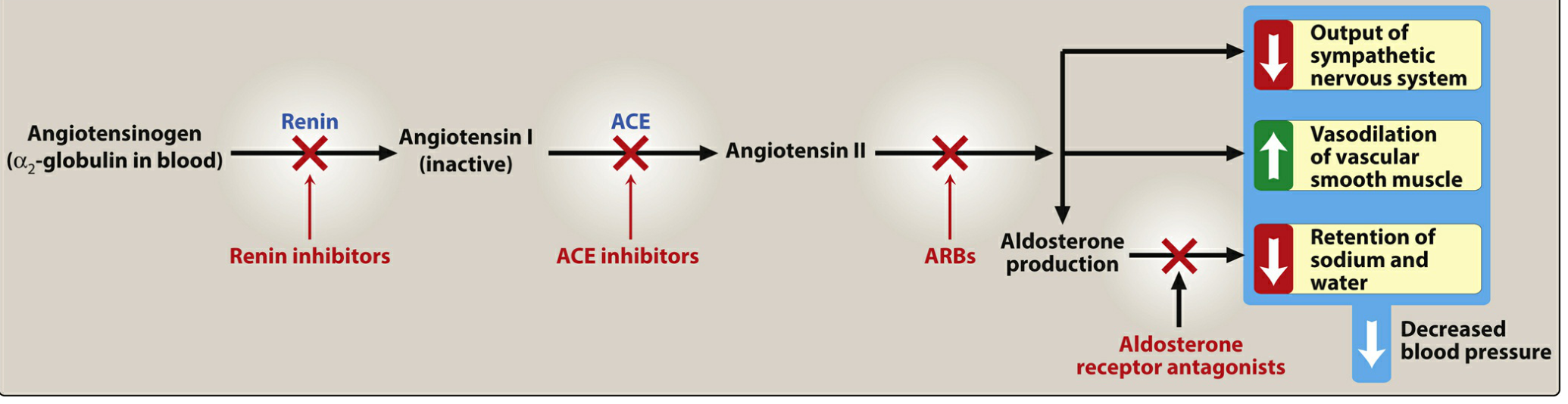
2. ACE INHIBITORS (ACEIs)
Examples: Captopril, enalapril, lisinopril, ramipril
Mechanism: Block ACE, which normally:
- Converts angiotensin I → angiotensin II (vasoconstrictor)
- Degrades bradykinin (a vasodilator that stimulates NO and prostacyclin)
Result: Decreased angiotensin II + increased bradykinin → vasodilation of arterioles AND veins, reduced aldosterone → less Na/water retention → decreased preload and afterload.
Compelling indications (first-line): Coronary artery disease, diabetes, heart failure, post-MI, chronic kidney disease, stroke history.
ADRs:
- Dry cough (bradykinin accumulation - most common reason to switch to ARB)
- Angioedema (rare but potentially life-threatening)
- Hyperkalemia (reduced aldosterone)
- Fetotoxicity - absolutely contraindicated in pregnancy
- First-dose hypotension (especially in volume-depleted patients)
3. ANGIOTENSIN RECEPTOR BLOCKERS (ARBs)
Examples: Losartan, valsartan, irbesartan, candesartan, telmisartan
Mechanism: Block AT₁ receptors directly, preventing angiotensin II from causing vasoconstriction and aldosterone secretion. Unlike ACEIs, they do NOT affect bradykinin degradation, so dry cough is absent.
Use: Same compelling indications as ACEIs; preferred when ACEIs cause cough or angioedema.
ADRs: Hyperkalemia, fetotoxicity. Do NOT combine with ACEIs (increased adverse effects, no added benefit).
4. CALCIUM CHANNEL BLOCKERS (CCBs)
Mechanism: Reduce calcium influx into vascular smooth muscle and cardiac cells → vasodilation, reduced peripheral resistance.
Two subclasses:
| Feature | Dihydropyridines (DHPs) | Non-DHPs |
|---|---|---|
| Examples | Nifedipine, amlodipine, felodipine, nicardipine | Verapamil, diltiazem |
| Primary effect | Vascular smooth muscle >> cardiac | Cardiac = vascular |
| Reflex tachycardia | Yes (especially short-acting nifedipine) | No |
| Use in angina | Vasospastic | Stable + vasospastic |
| Use in arrhythmias | No | Yes (rate control) |
| Negative inotropy | Minimal | Significant |
Key notes:
- Long-acting DHPs are preferred; short-acting nifedipine causes reflex tachycardia and is not recommended for chronic use
- Very effective in elderly and in patients with atherosclerotic angina
- IV nicardipine and clevidipine are used for acute/peri-operative hypertension
- ADRs (DHPs): Peripheral edema, flushing, headache, reflex tachycardia
- ADRs (non-DHPs): Bradycardia, AV block, constipation (verapamil), negative inotropy - avoid in heart failure with reduced EF
5. BETA-BLOCKERS (β-Blockers)
Examples: Metoprolol, atenolol, bisoprolol (selective β₁), propranolol, carvedilol (non-selective)
Mechanism: Block β-adrenoceptors → reduced heart rate, reduced contractility → reduced cardiac output. Also reduce renin secretion from juxtaglomerular cells.
Types:
- β₁-selective (cardioselective): Metoprolol, atenolol, bisoprolol - safer in asthma/COPD
- Non-selective: Propranolol (also blocks β₂ → bronchoconstriction)
- With α-blocking: Carvedilol, labetalol - also vasodilate
Compelling indications: Heart failure (bisoprolol, carvedilol, metoprolol succinate), post-MI, ischemic heart disease, certain arrhythmias.
ADRs:
- Bradycardia, heart block
- Bronchospasm (avoid in asthma; use with caution in COPD)
- Fatigue, cold extremities
- Masking hypoglycemia symptoms (use cautiously in diabetes)
- Insomnia, dizziness
- Rebound hypertension on abrupt withdrawal
Note: Less preferred than CCBs in elderly unless heart failure is present; considered less useful than ACEIs/ARBs in non-diabetic elderly patients.
6. ALPHA-BLOCKERS (α₁-Blockers)
Examples: Prazosin, doxazosin, terazosin
Mechanism: Block postsynaptic α₁-adrenoceptors → vasodilation of arterioles and veins → decreased peripheral resistance.
Use: Hypertension, especially in men with benign prostatic hyperplasia (dual benefit).
ADRs: First-dose phenomenon (severe orthostatic hypotension), reflex tachycardia, sodium/water retention (use with diuretic).
7. CENTRALLY ACTING SYMPATHOPLEGICS
Examples: Clonidine, methyldopa
Mechanism: Stimulate central α₂-adrenoceptors → reduce sympathetic outflow from brainstem vasomotor centers. Baroreceptor reflexes remain intact, so orthostatic hypotension is less prominent than with peripheral sympathoplegics.
- Methyldopa: Converted to α-methylnorepinephrine (false transmitter). Drug of choice for hypertension in pregnancy. ADRs: sedation, positive Coombs test, hemolytic anemia (rare), hepatotoxicity.
- Clonidine: ADRs include sedation, dry mouth, rebound hypertension on abrupt withdrawal - must taper slowly.
8. DIRECT VASODILATORS
Examples: Hydralazine, minoxidil (oral); sodium nitroprusside, fenoldopam (parenteral)
Mechanism:
| Drug | Mechanism |
|---|---|
| Hydralazine | Releases NO → arteriolar dilation |
| Minoxidil | Opens K⁺ channels → membrane hyperpolarization → arteriolar dilation |
| Nitroprusside | Releases NO → arteriolar + venous dilation |
| Fenoldopam | Dopamine D₁ receptor agonist → arteriolar dilation |
Important: All vasodilators cause reflex tachycardia and sodium/water retention. Must be combined with a β-blocker (to counteract tachycardia) + diuretic (to counteract fluid retention). This is the rationale for triple therapy in severe hypertension.
Key ADRs:
- Hydralazine: Headache, tachycardia, nausea, lupus-like syndrome (at high doses, reversible). Approved for pregnancy-induced hypertension.
- Minoxidil: Hypertrichosis (hair growth - basis for topical use in male-pattern baldness), fluid retention, reflex tachycardia.
- Nitroprusside: Cyanide toxicity (releases CN⁻ as metabolite) - limit infusion duration.
9. RENIN INHIBITORS
Example: Aliskiren
Mechanism: Directly inhibits renin, the first step in the RAAS cascade, preventing conversion of angiotensinogen to angiotensin I. Do NOT combine with ACEIs or ARBs (increased risk of hyperkalemia, hypotension, renal impairment, especially in diabetics).
Compelling Indications: Drug Choice by Co-Morbidity
| Condition | Preferred Drug Class |
|---|---|
| Heart failure with reduced EF | ACEIs/ARBs + β-blockers (bisoprolol, carvedilol) + MRA |
| Post-MI | ACEIs/ARBs + β-blockers |
| Coronary artery disease / Angina | β-blockers, CCBs, ACEIs |
| Diabetes with CKD | ACEIs or ARBs (reduce proteinuria) |
| CKD (without diabetes) | ACEIs or ARBs |
| Isolated systolic hypertension (elderly) | Thiazides, long-acting CCBs |
| Pregnancy | Methyldopa, labetalol, hydralazine, nifedipine |
| BPH + hypertension | α₁-blockers (doxazosin) |
| Atrial fibrillation (rate control) | β-blockers, verapamil, diltiazem |
Resistant Hypertension & Polypharmacy
Up to 40% of hypertensive patients require 2 or more drugs. The standard triple therapy for resistant hypertension is:
ACEI or ARB + CCB + Thiazide diuretic
If still uncontrolled, add a mineralocorticoid receptor antagonist (spironolactone) - particularly effective in resistant hypertension.
Reasons for polypharmacy:
- Most drugs trigger compensatory mechanisms (e.g., vasodilators → reflex tachycardia + sodium retention)
- Some drugs have modest maximum efficacy but important long-term organ-protective effects (ACEIs)
- Combination allows lower doses → less toxicity from each drug
Drugs for Hypertensive Emergencies (Parenteral)
| Drug | Key Feature |
|---|---|
| Sodium nitroprusside | Very rapid onset; cyanide toxicity risk |
| Nicardipine (IV) | CCB; safe in most emergencies |
| Labetalol (IV) | α + β blocker; safe in pregnancy |
| Hydralazine (IV) | Preferred in eclampsia |
| Fenoldopam (IV) | Dopamine agonist; improves renal perfusion |
| Clevidipine (IV) | Ultra-short acting DHP-CCB; perioperative |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | Lippincott Illustrated Reviews Pharmacology | Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.