Explain pft full detail for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching Images
pulmonary function test flow volume loop obstructive restrictive spirometry
Finding Sources
Loading Image
Reading File
I now have all the comprehensive content needed for a full 15-mark MD exam answer. Let me compile the complete answer:
Pulmonary Function Tests (PFT) — Complete 15-Mark Answer
Definition & Overview
Pulmonary function tests (PFTs) are a group of non-invasive tests that measure how well the lungs work by assessing lung volumes, airflow rates, and gas exchange. They are essential for diagnosing, classifying, and monitoring respiratory diseases, and for preoperative risk assessment.
I. Lung Volumes and Capacities
Understanding lung volumes is the foundation of PFT interpretation.
Static Lung Volumes:
| Volume/Capacity | Definition | Normal (approx.) |
|---|---|---|
| Tidal Volume (TV) | Volume per normal quiet breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Extra volume inhaled beyond TV | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Extra volume exhaled beyond TV | ~1100 mL |
| Residual Volume (RV) | Volume remaining after maximal exhalation | ~1200 mL |
| Total Lung Capacity (TLC) | Volume at end of maximal inspiration | ~6000 mL |
| Vital Capacity (VC) | Maximum volume exhaled after maximal inhalation (TLC − RV) | ~4800 mL |
| Functional Residual Capacity (FRC) | Volume remaining at end of normal tidal exhalation (ERV + RV) | ~2200 mL |
| Inspiratory Capacity (IC) | TV + IRV | ~3500 mL |
Key Point: TV, VC, and IRV/ERV can be measured by spirometry alone. FRC, RV, and TLC require helium dilution, nitrogen washout, or body plethysmography. — Murray & Nadel's Textbook of Respiratory Medicine
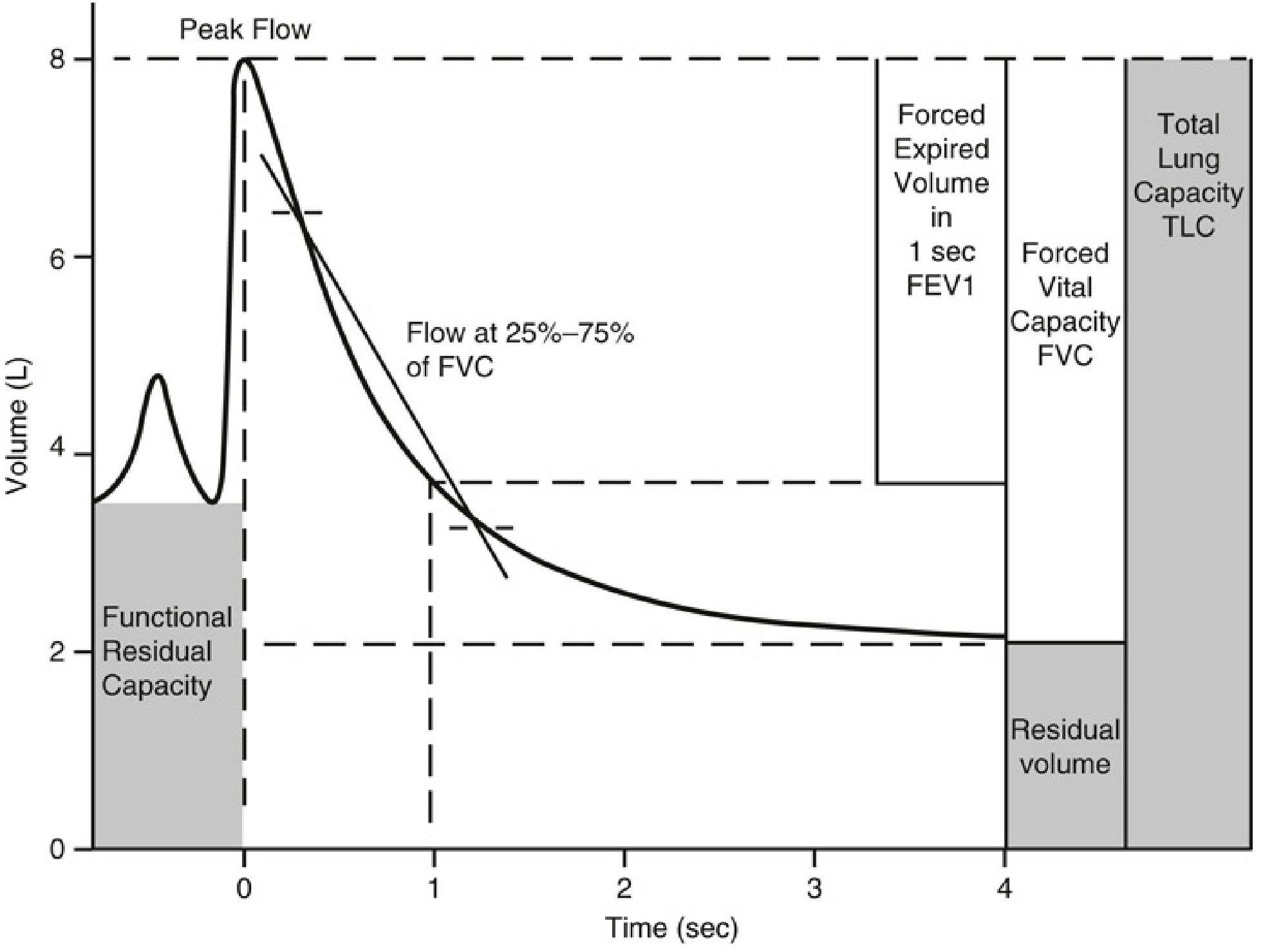
Spirometry tracing showing FEV1, FVC, FRC, RV, and TLC (Miller's Anesthesia, 10e)
II. Methods of Measuring Lung Volumes
1. Body Plethysmography (Gold Standard)
- Patient sits inside an airtight constant-volume chamber ("body box")
- Makes inspiratory efforts against a closed shutter
- Applies Boyle's Law (P₁V₁ = P₂V₂) to calculate FRC/RV
- Advantage: Measures all lung gas including trapped gas
- Disadvantage: May overestimate in severe obstruction (abdominal gas compression)
2. Helium Dilution
- Patient breathes known concentration of helium at FRC
- Helium mixes with lung gas and is diluted
- Formula: C₁ × V₁ = C₂ × (V₁ + FRC)
- Disadvantage: Underestimates in severe airway obstruction (trapped gas not measured)
3. Nitrogen Washout
- Patient breathes 100% oxygen; nitrogen "washes out"
- Expired nitrogen volume measured until concentration approaches zero
- Based on conservation of mass principle
III. Spirometry
Spirometry is the most commonly performed PFT. The patient inhales maximally to TLC, then exhales as forcefully and completely as possible.
Key Spirometric Measurements:
| Parameter | Definition | Normal |
|---|---|---|
| FVC (Forced Vital Capacity) | Total volume forcefully exhaled | ≥80% predicted |
| FEV₁ (Forced Expiratory Volume in 1 sec) | Volume exhaled in first second of FVC | ≥80% predicted |
| FEV₁/FVC ratio | Proportion of FVC exhaled in first second | ≥0.70 (LLN-based: >5th percentile) |
| FEF₂₅–₇₅% (Peak mid-expiratory flow) | Mean flow over 25–75% of FVC; reflects small airway function | Variable |
| PEFR (Peak Expiratory Flow Rate) | Maximum flow achieved during forced exhalation | Age/sex/height dependent |
| MVV (Maximal Voluntary Ventilation) | Maximum volume breathed per minute | ~170 L/min |
IV. Interpretation of Spirometry
Step-by-Step Approach (ATS/ERS):
- Visual inspection of flow-volume curve — quality check and large airway lesions
- FEV₁/FVC ratio → If low → obstructive pattern; if normal → normal or restrictive
- FVC → If low with normal ratio → may be restrictive (needs TLC confirmation)
- TLC → Low TLC confirms restriction; normal TLC + low FVC = nonspecific pattern
Patterns of Disease:
| Parameter | Obstructive | Restrictive | Mixed |
|---|---|---|---|
| FEV₁ | ↓ | ↓ (proportionate) | ↓↓ |
| FVC | Normal or ↓ | ↓ | ↓ |
| FEV₁/FVC | ↓ (<0.70) | Normal or ↑ | ↓ |
| TLC | Normal or ↑ | ↓ | ↓ |
| RV | ↑ | ↓ | Variable |
| DLCO | Normal (asthma/CB) or ↓ (emphysema) | ↓ (parenchymal) | Variable |
"The major diffuse obstructive disorders are emphysema, chronic bronchitis, bronchiectasis, and asthma. An FEV₁/FVC ratio of less than 0.7 generally indicates the presence of obstructive disease." — Robbins & Kumar Basic Pathology
"In diffuse restrictive diseases, FVC is reduced and the expiratory flow rate is normal or reduced proportionately. Hence, the ratio of FEV₁ to FVC is near normal." — Robbins Basic Pathology
Grading of Severity (ATS/ERS — based on FEV₁ % predicted):
| Severity | FEV₁ (% Predicted) |
|---|---|
| Mild | >70% |
| Moderate | 60–69% |
| Moderately severe | 50–59% |
| Severe | 35–49% |
| Very severe | <35% |
— Fishman's Pulmonary Diseases & Disorders
V. Flow-Volume Loop Analysis
The flow-volume loop plots expiratory flow (y-axis) against volume (x-axis), with the inspiratory loop below the baseline.
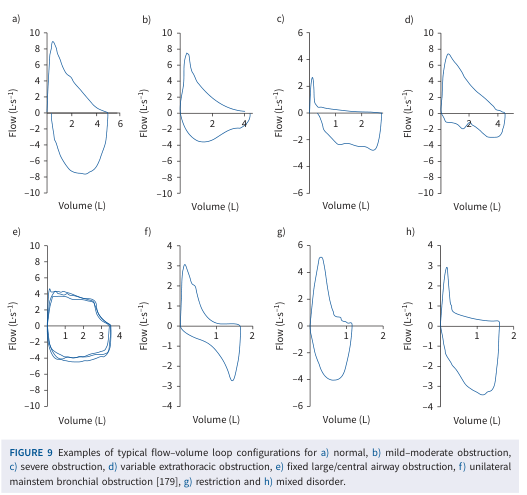
Flow-volume loop patterns: (a) Normal, (b) Mild-moderate obstruction, (c) Severe obstruction, (d) Variable extrathoracic obstruction, (e) Fixed large/central airway obstruction, (f) Unilateral mainstem bronchial obstruction, (g) Restriction, (h) Mixed disorder — Technical Standard on Interpretive Strategies for Lung Function Tests
Characteristic Patterns:
- Normal: High peak flow, smooth descending expiratory limb
- Obstructive (COPD/asthma): Reduced PEFR, scooped-out (concave) descending limb — hallmark of small airway collapse
- Restrictive: Narrow loop (reduced volumes), steep and tall but with normal shape proportionally
- Fixed large airway obstruction (e.g., tracheal stenosis, tracheal tumor): Plateaus on BOTH inspiratory and expiratory limbs (flow limited in both directions)
- Variable extrathoracic obstruction (e.g., vocal cord paralysis): Plateau only on inspiratory limb (negative intratracheal pressure during inspiration collapses the lesion)
- Variable intrathoracic obstruction (e.g., tracheomalacia): Plateau only on expiratory limb
VI. Diffusing Capacity for Carbon Monoxide (DLCO / Transfer Factor TLco)
Principle:
DLCO measures the functional capillary surface area available for gas exchange. CO is used because of its very high affinity for hemoglobin — so pulmonary blood flow does not limit CO transfer; only membrane thickness and area do.
Method (Single-breath technique):
- Patient exhales to RV
- Inhales mixture of 0.3% CO + 10% He (tracer) to TLC
- Holds breath 10 seconds
- Exhales; alveolar sample analyzed
- DLCO = CO uptake rate / driving pressure
Clinical Significance:
| Condition | DLCO |
|---|---|
| Emphysema | ↓↓ (destruction of alveolar-capillary surface) |
| Pulmonary fibrosis (IPF) | ↓ (membrane thickening, capillary loss) |
| Pulmonary hypertension | ↓ |
| Pulmonary embolism | ↓ |
| Asthma | Normal or ↑ |
| Polycythemia, left-to-right shunt | ↑ |
| Anemia | ↓ (corrected for Hb) |
| Normal spirometry | Normal DLCO helps exclude pulmonary vascular disease |
"DLCO is reduced in patients with interstitial lung diseases and emphysema. Values below 60% of predicted have been associated with increased risk of postoperative pulmonary complications." — Miller's Anesthesia, 10e
"In IPF, the decrease in DLCO results from both a loss of the pulmonary capillary volume and the presence of ventilation-perfusion abnormalities." — Murray & Nadel's Respiratory Medicine
VII. Bronchodilator Reversibility Testing
- Spirometry performed before and 15–20 minutes after short-acting bronchodilator (salbutamol 400 µg)
- Significant reversibility: ≥12% AND ≥200 mL increase in FEV₁ or FVC
- Positive in: Asthma (hallmark), partially reversible in COPD
- ATS/ERS recommendation: Post-bronchodilator values should be used for spirometry interpretation
VIII. Obstructive vs. Restrictive — Specific Disease Correlations
Obstructive Diseases:
- Asthma: ↓FEV₁/FVC, normal DLCO, reversible obstruction, air trapping (↑RV)
- COPD/Emphysema: ↓FEV₁/FVC, ↑TLC, ↑RV, ↓↓DLCO (emphysema), irreversible
- Chronic Bronchitis: ↓FEV₁/FVC, normal DLCO
- Bronchiectasis: ↓FEV₁/FVC, variable DLCO
Restrictive Diseases:
- Pulmonary fibrosis (IPF): ↓TLC, ↓FVC, normal FEV₁/FVC, ↓↓DLCO
- Sarcoidosis, asbestosis: Restrictive ± mixed, ↓DLCO
- Neuromuscular disease (GBS, MG): ↓TLC, ↓MIP/MEP, normal DLCO
- Chest wall disorders (kyphoscoliosis, obesity): ↓TLC, normal DLCO
- ARDS: Classic acute restrictive pattern
Mixed Pattern:
Occurs in: eosinophilic granulomatosis, ABPA, hypersensitivity pneumonitis, COP, COPD + fibrosis, endobronchial sarcoidosis — Goldman-Cecil Medicine
IX. Arterial Blood Gas (ABG) Correlation
PFTs are complemented by ABG analysis:
- Type 1 Respiratory Failure (PaO₂ <60 mmHg, normal PaCO₂): V/Q mismatch — IPF, PE
- Type 2 Respiratory Failure (PaO₂ <60 + PaCO₂ >45 mmHg): Ventilatory pump failure — COPD, neuromuscular disease
- Respiratory Alkalosis + Hypoxemia: Early IPF (hyperventilation to compensate)
X. Exercise Testing (CPET — Cardiopulmonary Exercise Test)
Used for unexplained dyspnea, pre-surgical assessment, transplant evaluation:
- Measures VO₂ max — gold standard for cardiopulmonary reserve
- Identifies cardiovascular vs. ventilatory vs. peripheral limitation
- 6-Minute Walk Test (6MWT): Simpler; correlates with DLCO and VO₂ max in IPF; strong predictor of mortality
XI. Preoperative Assessment (Pulmonary Risk)
| PFT finding | Implications |
|---|---|
| FEV₁ <60% predicted | Increased postoperative pulmonary complications |
| DLCO <60% predicted | Increased risk, consider CPET |
| FEV₁ <1.5 L (lobectomy) / <2 L (pneumonectomy) | High operative risk for lung resection |
| Predicted postoperative FEV₁ <40% | Very high risk for lung resection |
Summary Algorithm (ATS/ERS):
Spirometry
│
├── FEV₁/FVC < LLN → OBSTRUCTIVE
│ │
│ ├── DLCO normal → Asthma / Chronic Bronchitis
│ └── DLCO ↓ → Emphysema
│
└── FEV₁/FVC ≥ LLN
│
├── FVC normal → NORMAL (no restriction)
└── FVC ↓ → Measure TLC
│
├── TLC ↓ → RESTRICTIVE
│ ├── DLCO ↓ → Parenchymal (IPF, fibrosis)
│ └── DLCO normal → Chest wall / NM disease
├── TLC normal → Nonspecific pattern
└── TLC ↑ + RV ↑ → Air trapping (pseudo-restriction)
Key Exam Points to Remember
- FEV₁/FVC <0.70 = obstructive; TLC <80% = restrictive (gold standard for restriction)
- DLCO ↓ in emphysema (structural loss) but normal in asthma and chronic bronchitis
- Helium dilution underestimates in severe obstruction (trapped gas); body plethysmography is gold standard
- Flow-volume loop: Scooped expiratory = obstructive; plateaus on both limbs = fixed large airway obstruction; narrow loop = restrictive
- Bronchodilator reversibility ≥12% + ≥200 mL = significant (asthma vs. COPD distinction)
- Post-bronchodilator spirometry is used for definitive classification
- FVC ↓ with preserved FEV₁/FVC ratio in IPF — the restrictive signature
- DLCO corrected for Hb — reduce by 7% per g/dL Hb below 14.6 g/dL (anemia artificially lowers DLCO)
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases & Disorders; Miller's Anesthesia 10e; Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.