
IMG_20260621_103621_330@-1395505239.jpg
Explain diabetes mellitus
Reading File
Finding Sources
Searching PubMed
"diabetes mellitus" AND "pathogenesis"
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough, well-structured answer. Let me compile the comprehensive response.
Diabetes Mellitus
Definition
Diabetes mellitus (DM) is a group of metabolic disorders characterized by chronic hyperglycemia due to defects in insulin secretion, insulin action, or most commonly both. Long-standing hyperglycemia damages multiple organ systems - especially the kidneys, eyes, nerves, and blood vessels. In the United States, DM is the leading cause of end-stage renal disease, adult-onset blindness, and non-traumatic lower-extremity amputations.
- Robbins & Kumar Basic Pathology, p. 743
Epidemiology
- Over 37 million Americans (11% of the population) have diabetes; ~25% are undiagnosed.
- Approximately 1.4 million new cases are diagnosed yearly in the US.
- Type 2 DM accounts for the vast majority (~90-95%) of cases; Type 1 accounts for 5-10%.
- Rising rates of obesity and sedentary lifestyles have dramatically increased T2D globally.
Diagnosis
Blood glucose is normally maintained at 70-120 mg/dL. ADA/WHO diagnostic criteria (any one of the following, confirmed on repeat):
| Criterion | Threshold |
|---|---|
| Fasting plasma glucose | ≥ 126 mg/dL |
| Random plasma glucose (with symptoms) | ≥ 200 mg/dL |
| 2-hour glucose on 75g OGTT | ≥ 200 mg/dL |
| HbA1c | ≥ 6.5% |
Prediabetes is defined as:
- Fasting glucose 100-125 mg/dL ("impaired fasting glucose")
- 2-hr OGTT glucose 140-199 mg/dL
- HbA1c 5.7-6.4%
Up to one-fourth of individuals with prediabetes develop overt T2D within 5 years, especially those who are obese or have a positive family history.
- Robbins & Kumar Basic Pathology, p. 743-744
Classification
Type 1 Diabetes (T1D)
- Autoimmune destruction of pancreatic β-cells → absolute insulin deficiency
- 5-10% of cases; most common in those <20 years
- Previously called "insulin-dependent" or "juvenile-onset" diabetes
- Characterized by circulating islet autoantibodies
- Prone to diabetic ketoacidosis (DKA) without insulin
Type 2 Diabetes (T2D)
- Insulin resistance in peripheral tissues + relative insulin deficiency from impaired β-cell secretion
- ~90-95% of cases; typically in adults >40 years, but rising in youth
- Strongly associated with obesity (80% of patients)
- No islet autoantibodies; prone to nonketotic hyperosmolar coma
Comparison Table (from Robbins)
| Feature | Type 1 | Type 2 |
|---|---|---|
| Onset | Childhood/adolescence | Usually adulthood |
| Body habitus | Non-obese | Obese (80%) |
| Insulin levels | Progressively decrease | Increased early; normal/decreased late |
| Autoantibodies | Present | Absent |
| Acute crisis | DKA | Hyperosmolar coma |
| HLA linkage | Yes (MHC class I & II) | No |
| Islet pathology | Insulitis, β-cell depletion | Amyloid deposition (late), mild β-cell loss |
Other Types
- Monogenic (MODY): Single-gene mutations affecting β-cell development/function; diagnosed before age 25
- Gestational diabetes: Occurs in ~5% of pregnancies due to pregnancy-induced insulin resistance; resolves post-delivery but raises 10-year T2D risk
- Secondary diabetes: Due to pancreatitis, cystic fibrosis, pancreatic adenocarcinoma, Cushing syndrome, acromegaly
Normal Insulin Physiology (Background)
Normal glucose homeostasis depends on three interrelated processes:
- Hepatic glucose production (gluconeogenesis + glycogenolysis)
- Peripheral glucose uptake (mainly skeletal muscle)
- The insulin/glucagon axis
Insulin's anabolic actions:
- Promotes glucose uptake into muscle and fat
- Stimulates glycogen synthesis, lipogenesis, protein synthesis
- Inhibits gluconeogenesis, lipolysis, and protein degradation
- The primary stimulus for insulin release is glucose; gut-derived incretin hormones (GLP-1, GIP) amplify this response
Pathogenesis
Type 1 DM
T1D results from a T-cell mediated autoimmune attack on β-cells in genetically susceptible individuals:
- Genetic susceptibility: Strong linkage to HLA region (MHC class I and II genes); also CTLA4 and PTPN22 polymorphisms
- Environmental triggers: Viral infections (e.g., enteroviruses) or other environmental factors may precipitate autoimmunity in susceptible individuals
- Autoimmune insulitis: CD4+ and CD8+ T lymphocytes infiltrate islets; CD8+ cells directly kill β-cells; autoantibodies against islet antigens (anti-GAD, anti-IA-2, anti-insulin) appear years before clinical disease
- Progressive β-cell loss: Eventually >90% of β-cells are destroyed → overt diabetes
Type 2 DM
T2D results from a vicious cycle of insulin resistance + β-cell dysfunction:
Insulin resistance (peripheral tissues fail to respond normally to insulin):
- Obesity-associated factors are central: excess non-esterified fatty acids (NEFAs), pro-inflammatory cytokines (TNF-α, IL-6), decreased adiponectin
- Adipokines and inflammatory mediators from visceral fat impair insulin receptor signaling (specifically IRS-1 and IRS-2 phosphorylation)
- Ectopic fat deposition in liver and muscle worsens resistance
β-cell dysfunction (inadequate compensatory insulin secretion):
- Glucotoxicity (chronic hyperglycemia) and lipotoxicity (excess NEFAs) damage β-cells
- Progressive reduction in β-cell mass and function
- Amyloid deposition (from islet amyloid polypeptide/IAPP) in islets occurs late in disease
Genetic factors: Variants in PPARG, KCNJ11, and >100 other susceptibility loci identified through genome-wide association studies
Clinical Features
Classic Triad (the "3 Polys")
| Symptom | Mechanism |
|---|---|
| Polyuria | Osmotic diuresis from glycosuria (glucose exceeds renal threshold ~180 mg/dL) |
| Polydipsia | Dehydration from water loss in urine |
| Polyphagia | Cellular starvation despite hyperglycemia |
Additional features:
- Weight loss (especially T1D) - catabolism of fat and muscle
- Blurred vision (osmotic swelling of lens)
- Recurrent infections (impaired leukocyte function)
- Fatigue
T1D typically presents acutely and dramatically; T2D is often asymptomatic for years and detected incidentally on routine blood tests.
Acute Complications
Diabetic Ketoacidosis (DKA) - primarily T1D
- Absolute insulin deficiency → unrestrained lipolysis and gluconeogenesis
- Free fatty acids → hepatic ketone body production (acetoacetate, β-hydroxybutyrate)
- Anion gap metabolic acidosis + hyperglycemia + ketonuria/ketonemia
- Triggers: infection, missed insulin doses
Hyperosmolar Hyperglycemic State (HHS) - primarily T2D
- Extreme hyperglycemia (>600 mg/dL) + severe dehydration without significant ketosis
- Residual insulin prevents ketogenesis but insufficient to prevent hyperglycemia
- High mortality; requires aggressive fluid resuscitation
Hypoglycemia
- Most common acute complication of insulin and sulfonylurea therapy
- Symptoms: sweating, tremor, tachycardia, confusion → seizures, coma
Chronic Complications
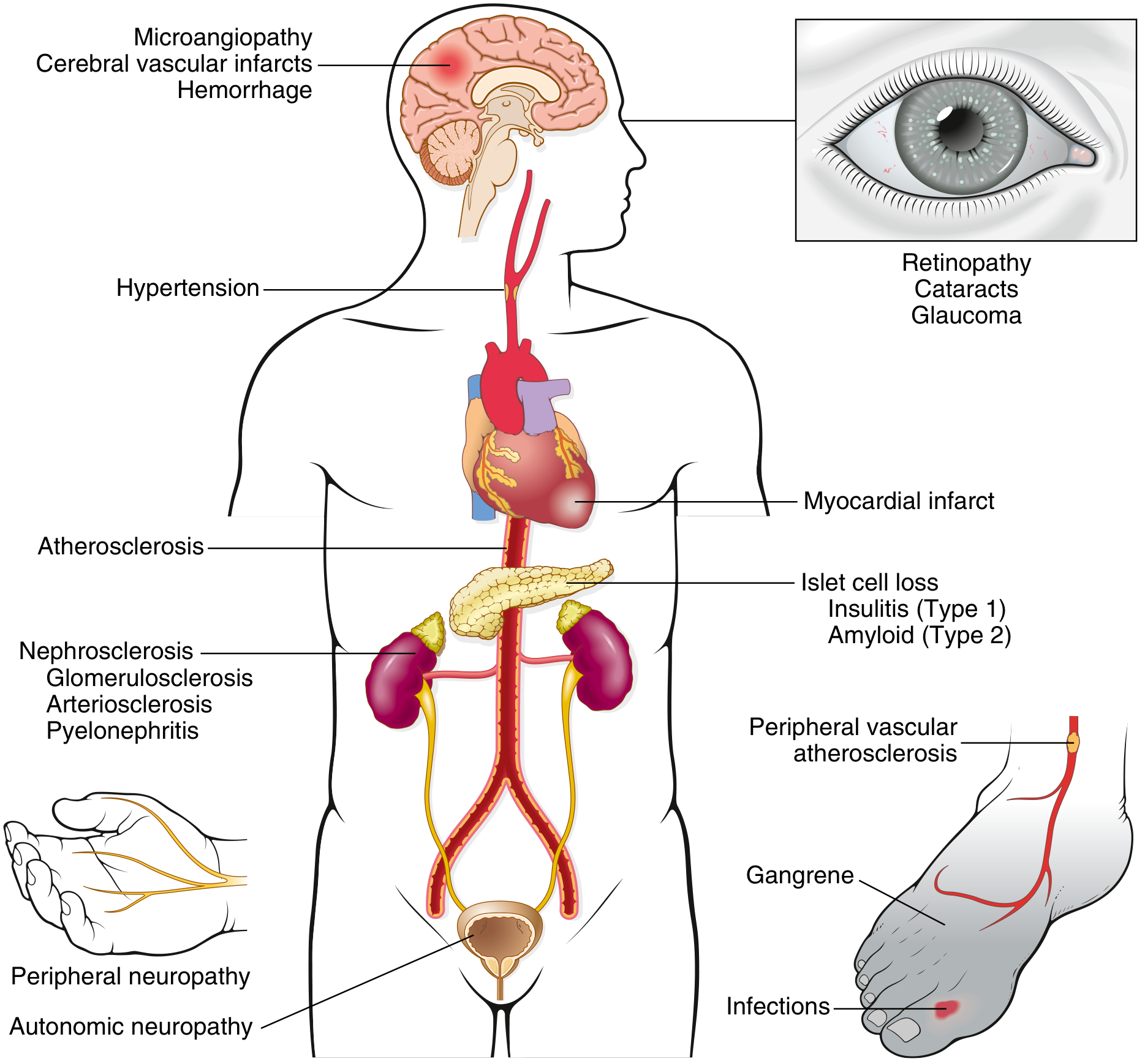
Fig. 18.22 - Long-term complications of diabetes (Robbins & Kumar)
Chronic complications arise from glucotoxicity acting through three main mechanisms:
1. Advanced Glycation End-Products (AGEs)
- Glucose reacts non-enzymatically with amino groups of proteins → AGEs
- AGEs bind receptor RAGE on endothelium, macrophages, smooth muscle
- Results in: release of TGF-β (excess basement membrane) and VEGF (retinal neovascularization), generation of reactive oxygen species (ROS), increased procoagulant activity, enhanced vascular smooth muscle proliferation
2. Protein Kinase C (PKC) Activation
- Hyperglycemia → de novo synthesis of diacylglycerol (DAG) → PKC activation
- Downstream: VEGF (neovascularization in retinopathy), TGF-β (fibrosis), ECM deposition
3. Polyol Pathway (Sorbitol Accumulation)
- In insulin-independent tissues (nerves, lens, kidneys, vessels): aldose reductase converts excess glucose → sorbitol → fructose
- Consumes NADPH (needed for glutathione regeneration → oxidative stress)
- Osmotic damage in nerves and lens (cataracts)
Macrovascular Disease
- Accelerated atherosclerosis of large and medium arteries
- Consequences: myocardial infarction (2-4x increased risk), ischemic stroke, peripheral arterial disease → gangrene
Microvascular Disease
| Complication | Manifestation |
|---|---|
| Diabetic retinopathy | Non-proliferative (microaneurysms, hemorrhages, exudates) → proliferative (neovascularization) → blindness; cataracts; glaucoma |
| Diabetic nephropathy | Nodular glomerulosclerosis (Kimmelstiel-Wilson lesions), proteinuria, progressive CKD → ESRD |
| Diabetic neuropathy | Distal symmetric polyneuropathy (burning, tingling, loss of sensation); autonomic neuropathy (gastroparesis, erectile dysfunction, orthostatic hypotension) |
Increased Susceptibility to Infections
-
Impaired neutrophil chemotaxis and phagocytosis
-
Skin/soft tissue infections, UTIs, pneumonia, mucormycosis
-
Robbins & Kumar Basic Pathology, p. 749-754
Management Overview
Type 1 DM - Insulin is mandatory
- Basal-bolus regimen: long-acting insulin (glargine, degludec) + rapid-acting insulin (aspart, lispro) with meals
- Continuous subcutaneous insulin infusion (CSII) pumps + continuous glucose monitoring (CGM)
- Automated Insulin Delivery (AID) systems combine pump + CGM + algorithm
- Medical nutrition therapy (MNT): carbohydrate counting, avoiding excessive weight gain
- Exercise: 150 min/week moderate aerobic activity; monitor glucose around exercise
Type 2 DM - Stepwise approach
- Lifestyle: weight loss (5-10%), reduced caloric intake, physical activity
- Metformin: first-line pharmacotherapy (reduces hepatic glucose output)
- Additional agents based on comorbidities:
- GLP-1 receptor agonists (liraglutide, semaglutide) - weight loss benefit, CV protection
- SGLT-2 inhibitors (empagliflozin, dapagliflozin) - renal/CV protection
- DPP-4 inhibitors, sulfonylureas, thiazolidinediones, insulin
- Glycemic targets: HbA1c <7% for most patients (individualized)
- Cardiovascular risk factor management: BP, lipids, antiplatelet therapy
Key Monitoring Parameters
-
HbA1c every 3 months (reflects average glucose over ~3 months)
-
Self-monitoring of blood glucose (SMBG) or CGM
-
Annual dilated eye exam, urine albumin-to-creatinine ratio, lipid panel, foot exam, blood pressure
-
Harrison's Principles of Internal Medicine 22E, p. [insulin management section]
-
Robbins & Kumar Basic Pathology, p. 743-757
Summary
Diabetes mellitus is fundamentally a disorder of glucose homeostasis driven by insufficient insulin effect - either from autoimmune destruction of β-cells (T1D) or from the combination of insulin resistance and progressive β-cell failure (T2D). The clinical consequences span acute life-threatening emergencies (DKA, HHS) to chronic, insidious microvascular and macrovascular damage affecting virtually every organ system. Tight glycemic control, together with management of blood pressure and lipids, remains the cornerstone of preventing or delaying these devastating complications.
This is a shared conversation. Sign in to Orris to start your own chat.