Rh isoimmunization
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching PubMed
Rh isoimmunization prevention anti-D immunoglobulin
Here is a thorough overview of Rh isoimmunization drawn from authoritative textbooks.
Rh Isoimmunization (Rh Alloimmunization)
Definition
Rh isoimmunization is a condition in which an Rh-negative individual develops IgG antibodies against Rh (D) antigens on red blood cells, most clinically significant when an Rh-negative mother is sensitized by an Rh-positive fetus. It is the primary cause of immune hydrops fetalis and hemolytic disease of the fetus and newborn (HDFN), also called erythroblastosis fetalis.
The Rh Blood Group System
- Encoded by two closely linked genes on chromosome 1p: RhD and RhCE
- The Rh system comprises multiple antigens: C, c, D, E, e - of these, only the D antigen is a major cause of clinically significant isoimmunization
- Prevalence of RhD negativity: ~15% of Caucasians, ~5% of Africans, <1% of Asians
- The most prevalent RhD-negative allele is a deletion of the RhD gene
(Tietz Textbook of Laboratory Medicine, 7th ed.)
Pathogenesis
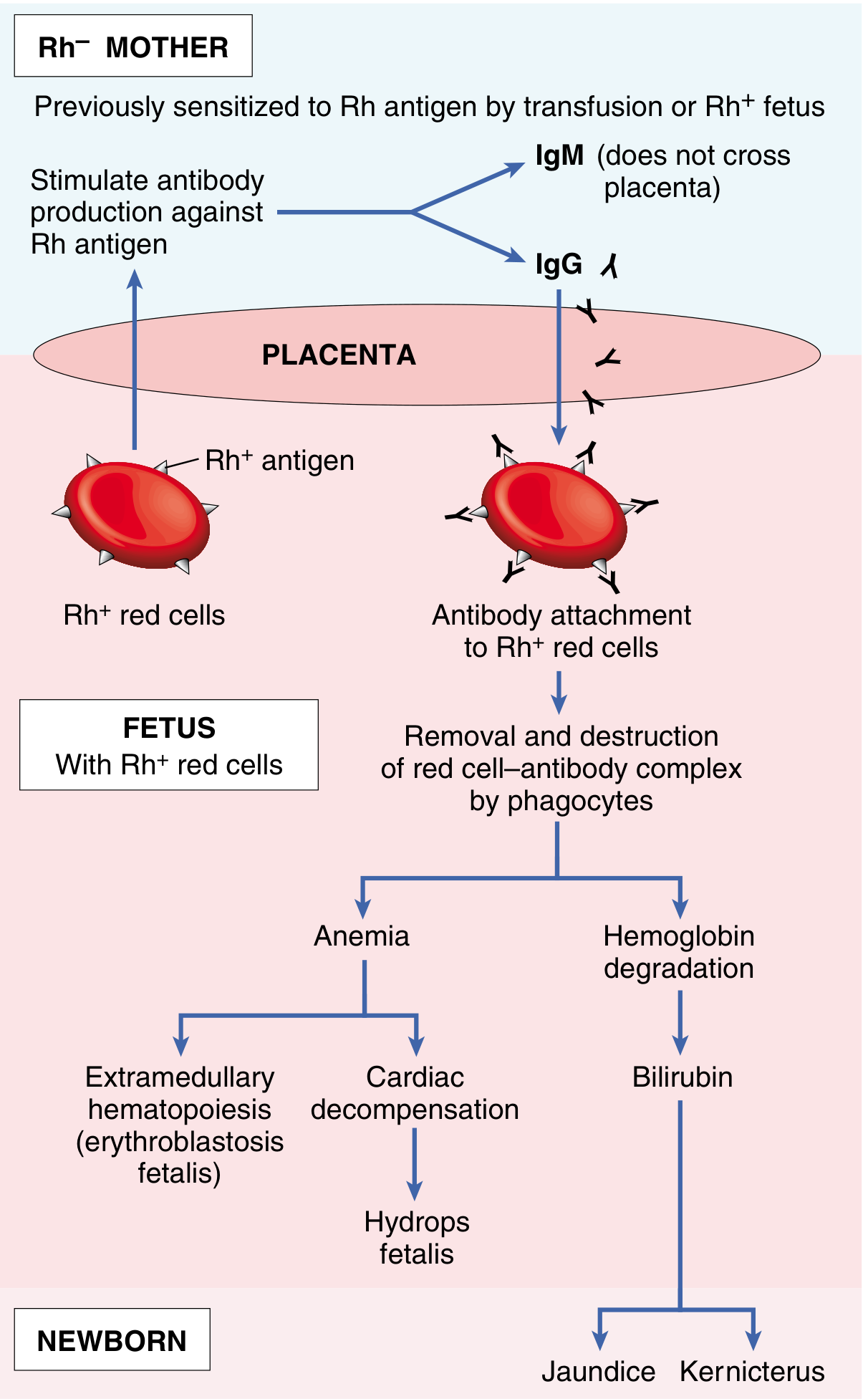
Pathogenesis of immune hydrops fetalis (Robbins & Cotran Pathologic Basis of Disease)
Step-by-step mechanism
- Sensitization (first pregnancy): Fetal Rh-positive RBCs cross the placenta (especially during the third trimester or at delivery) and enter the Rh-negative maternal circulation
- Initial immune response: The mother mounts a primary immune response producing IgM antibodies - these do NOT cross the placenta, so the first pregnancy is usually unaffected
- Subsequent pregnancies: Re-exposure to Rh-positive fetal RBCs triggers a brisk anamnestic (secondary) IgG response
- Placental transfer of IgG: Maternal IgG anti-D antibodies are actively transported across the placenta into the fetal circulation
- Fetal RBC destruction: Antibody-coated fetal RBCs are destroyed by phagocytes (extravascular hemolysis, primarily in the spleen)
Factors influencing sensitization
- Dose of antigen: Hemolytic disease typically requires >1 mL of Rh-positive fetal red cells reaching the maternal circulation
- ABO incompatibility is protective: If the fetus is also ABO-incompatible with the mother, fetal RBCs entering the maternal circulation are rapidly cleared by anti-A or anti-B IgM antibodies before the mother can mount an Rh immune response
- Antibody specificity, titer, transfer rate, and functional maturity of the fetal spleen all affect severity
(Robbins, Cotran & Kumar, Pathologic Basis of Disease)
Consequences of Fetal Hemolysis
| Consequence | Mechanism |
|---|---|
| Fetal anemia | Destruction of RBCs faster than replacement |
| Extramedullary hematopoiesis (erythroblastosis fetalis) | Liver & spleen attempt compensatory RBC production; hepatocytes destroyed |
| Hypoalbuminemia | Liver injury reduces albumin synthesis; reduced oncotic pressure |
| High-output cardiac failure | Heart compensates for anemia with increased output |
| Hydrops fetalis | Generalized edema from combined low oncotic pressure + cardiac failure; often fatal without intervention |
| Jaundice | Hemoglobin degradation → unconjugated bilirubin accumulation post-delivery |
| Kernicterus | Unconjugated bilirubin crosses the immature blood-brain barrier and deposits in basal ganglia, causing brain damage |
(Tietz Textbook of Laboratory Medicine, 7th ed.; Robbins & Cotran)
ABO vs. Rh Incompatibility - Key Differences
| Feature | ABO | Rh (D) |
|---|---|---|
| First pregnancy affected? | Yes (certain group O mothers have IgG anti-A/B) | Usually No |
| Antibody type | Mainly IgM (non-pathological) + some IgG | IgG (pathological) |
| Incidence | ~20-25% of pregnancies, hemolysis in 1/10 | Less common but more severe |
| Hydrops fetalis | Rare | Common (if untreated) |
| Prevention | No effective prophylaxis | RhIg (RhoGAM) highly effective |
(Robbins & Cotran Pathologic Basis of Disease)
Investigations / Monitoring
Maternal
- Indirect Coombs test (Indirect Antiglobulin Test, IAT): Screens maternal serum for anti-D antibodies; the primary test for alloimmunization
- Serial antibody titers: rising titers indicate ongoing sensitization
Fetal Surveillance (once mother is sensitized)
- Middle Cerebral Artery (MCA) Doppler velocimetry - Current gold standard for non-invasive fetal anemia monitoring
- Peak systolic velocity (PSV) >1.5 MoM (multiples of the median) for gestational age accurately detects moderate/severe anemia
- False-positive rates increase after 35 weeks
- Amniocentesis with spectrophotometry (ΔOD450) - Historically used (Liley curve/Queenan curve)
- Amniotic fluid bilirubin at 450 nm plotted on Liley's graph (zones 1-3: mild/moderate/severe)
- Largely replaced by MCA Doppler but still useful after 35 weeks
- Cordocentesis (fetal blood sampling): Indicated when MCA PSV >1.5 MoM - fetal hematocrit <30% is indication for intrauterine transfusion (IUT)
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
Management
Unsensitized Rh-negative mother (Prevention)
Anti-D Immunoglobulin (RhIg / RhoGAM) - the cornerstone of prevention:
- Antenatal: 300 mcg IM at 28 weeks gestation (prevents sensitization from undetected antepartum fetomaternal bleeding)
- Postpartum: 300 mcg IM within 72 hours of delivery of Rh-positive infant
- Also administered after: spontaneous or therapeutic abortion, amniocentesis, CVS, fetomaternal hemorrhage
- A 300 mcg dose covers up to 15 mL of Rh-positive fetal RBCs
- Kleihauer-Betke test (acid elution test) quantifies fetomaternal hemorrhage volume to determine if additional RhIg doses are needed
- Introduction of RhIg in 1968 (RhoGAM) has caused a dramatic reduction in HDN incidence worldwide
(Tietz Textbook of Laboratory Medicine, 7th ed.; Harriet Lane Handbook, 23rd ed.)
Sensitized mother / Affected fetus
| Gestational Age | Intervention |
|---|---|
| Fetal hematocrit <30% before 35 weeks | Intrauterine transfusion (IUT) via cordocentesis into umbilical vein |
| ≥35 weeks with rising ΔOD450 or anemia | Delivery (induction of labor) |
| Hydrops fetalis | Emergency IUT or early delivery depending on gestational age |
Newborn management
- Phototherapy for hyperbilirubinemia
- Exchange transfusion for severe hyperbilirubinemia or kernicterus risk
- Supportive care for hydrops (pleural drainage, respiratory support)
Recent Evidence
A 2026 systematic review (PMID 41406924) highlights that RhD alloimmunization and HDFN remain significant causes of perinatal mortality in Africa, where access to RhIg is limited. A 2026 systematic review (PMID 40728267) examined Rhesus testing and anti-D prophylaxis specifically in Rh-negative women undergoing first-trimester abortion, finding that evidence supports offering RhIg in this setting.
Summary
Rh isoimmunization is largely a preventable disease. Its pathogenesis hinges on the shift from non-pathological IgM (first pregnancy) to pathological transplacental IgG (subsequent pregnancies). The consequences range from mild neonatal jaundice to fatal hydrops fetalis. Prevention with anti-D immunoglobulin (RhoGAM) at 28 weeks and within 72 hours postpartum has dramatically reduced its incidence. In sensitized pregnancies, MCA Doppler monitoring and timely intrauterine transfusion or early delivery are the pillars of management.
This is a shared conversation. Sign in to Orris to start your own chat.