Explain everything about keratokonus
Reading File
Finding Sources
Searching PubMed
keratoconus diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple textbooks. Let me compile the full detailed answer.
Keratoconus - A Complete Overview
Definition
Keratoconus (KC) is a progressive, non-inflammatory ectatic disorder of the cornea characterized by central or paracentral stromal thinning, apical protrusion in a cone configuration, and irregular astigmatism. The name derives from the Greek keras (horn/cornea) and konos (cone).
Epidemiology
- Prevalence: ~0.1-0.2% (approximately 55 cases per 100,000 in the US), though subclinical cases likely make this an underestimate
- Age of onset: Typically during the teens or twenties; rarely congenital
- Sex: Men are slightly more affected than women
- Laterality: Almost always bilateral, but commonly asymmetric at presentation. About 50% of normal fellow eyes will progress to KC within 16 years; virtually all cases become bilaterally affected on topographic imaging eventually
Etiology & Pathogenesis
The cause is multifactorial:
Genetic factors:
- Most patients have no family history; only ~10% of offspring develop KC
- Autosomal dominant transmission with incomplete penetrance has been proposed
- Associated with chromosomal loci on several chromosomes (VSX1, SOD1, and others)
Biochemical/structural abnormality:
- Degradation of stromal collagen fibrils and loss of lamellar organization
- Increased activity of proteolytic enzymes (matrix metalloproteinases) causes collagen breakdown
- Oxidative stress and free radical damage to stromal keratocytes play a role
- Result: focal stromal thinning, cornea loses its structural integrity and bulges forward under intraocular pressure
Mechanical factor:
- Chronic eye rubbing is a well-established risk factor and driver of progression - rubbing likely induces cytokine release (IL-1, TNF-alpha) causing keratocyte apoptosis
Risk Factors & Associations
Systemic associations:
- Down syndrome (trisomy 21) - most common
- Ehlers-Danlos syndrome
- Marfan syndrome
- Osteogenesis imperfecta
- Turner syndrome
- Sleep apnea / floppy eyelid syndrome
- Mitral valve prolapse
- Leber congenital amaurosis
- Retinitis pigmentosa
Ocular associations:
- Vernal keratoconjunctivitis (atopic disease)
- Allergy, asthma, eczema (the chronic rubbing from these drives KC)
- Blue sclera
- Aniridia
Behavioral:
- Chronic eye rubbing (from any cause)
Family history is also an independent risk factor.
Grading (by keratometry)
| Grade | Highest keratometry power |
|---|---|
| Mild | < 48 D |
| Moderate | 48 - 54 D |
| Severe | > 54 D |
Clinical Features
Symptoms
- Progressive decrease in vision - progressive myopia and irregular astigmatism
- Monocular diplopia, ghosting of images
- Starbursts and halos around lights
- Frequent changes in spectacle prescription
- In acute hydrops: sudden painful decrease in vision, red eye, photophobia, profuse tearing
Signs - Examination Findings
Direct ophthalmoscopy (at ~0.5 m):
The classic "oil droplet" reflex - a well-delineated bright reflex against the red background

Retinoscopy:
- Irregular "scissoring" or "water droplet" reflex due to irregular astigmatism
Slit-lamp biomicroscopy:
| Sign | Description |
|---|---|
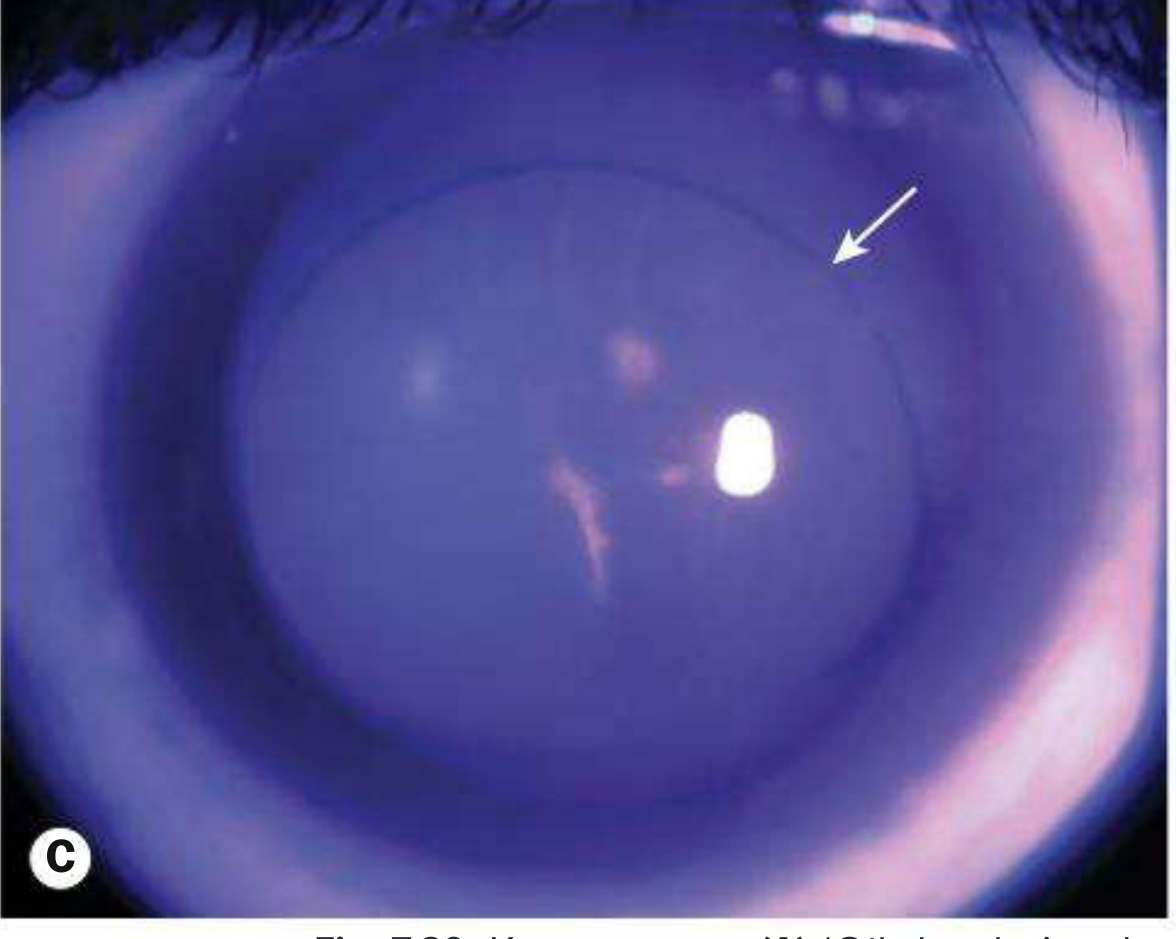
| Vogt striae | Very fine, vertical, deep stromal stress lines that disappear with pressure on the globe |
| Fleischer ring | Epithelial iron deposits (hemosiderin) surrounding the base of the cone - best seen with cobalt blue filter |
| Corneal thinning | Maximal thinning at the apex of the cone; usually inferocentral location |
| Superficial apical scarring | In advanced disease |
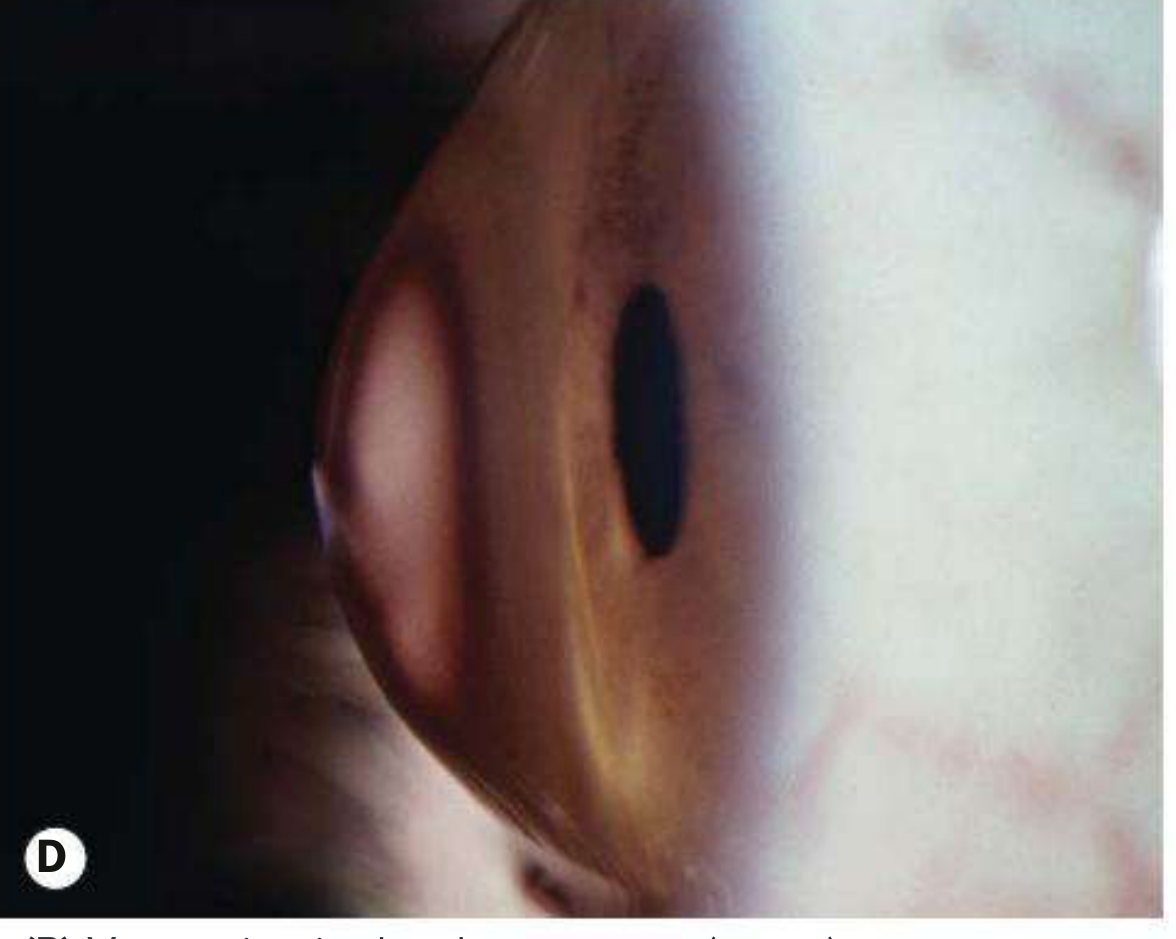
| Munson sign | Bulging of the lower eyelid in downgaze due to the protruding cone |
Keratometry:
- Steep irregular readings; egg-shaped ("mire") distortion
Corneal topography / tomography:
- Inferior steepening is characteristic
- Topographic progression: symmetrical bow-tie pattern → asymmetrical → inferotemporally displaced steep-sided cone (sometimes a central "nipple" cone)
- Tomography (Pentacam/Scheimpflug imaging) shows posterior corneal elevation, anterior thinning, and inferior displacement of the thinnest corneal point
Acute Corneal Hydrops
A complication of advanced KC:
- Mechanism: Stretching and rupture of Descemet membrane allows aqueous humor to suddenly flood the corneal stroma
- Symptoms: Acute severe decrease in vision, pain, red eye, photophobia, profuse tearing
- Course: Descemet membrane usually heals within 6-10 weeks; edema clears, but variable stromal scarring may develop (which can paradoxically flatten the cone and sometimes improve vision)
Management of acute hydrops:
- Cycloplegic agent (e.g., cyclopentolate 1% TID) for pain relief if anterior chamber reaction present
- Aqueous suppressant (e.g., brimonidine 0.1% BID-TID)
- Sodium chloride 5% ointment BID-QID until resolved (typically weeks to months)
- Consider topical steroids to suppress corneal neovascularization
- Protective eyewear (shield)
- Intracameral gas (air, SF6, or C3F8) may speed resolution but carries risks (cataract, pupillary block glaucoma)
- Note: Acute hydrops is NOT an indication for emergency corneal transplantation
Workup & Diagnosis
- History: Rate of visual decline, frequency of prescription changes, eye rubbing, allergies, family history, previous refractive surgery
- Slit-lamp exam: Vogt striae, Fleischer ring, thinning, scarring
- Retinoscopy and refraction: Irregular astigmatism, scissors reflex
- Corneal topography: Shows central/inferior steepening
- Corneal tomography (Pentacam/Scheimpflug): Gold standard - shows posterior elevation, thinning map, and pachymetry; detects subclinical ("forme fruste") keratoconus
- Keratometry: Irregular mires and steep values
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Pellucid marginal degeneration | Inferior peripheral thinning (4-8 o'clock), 1-2 mm from limbus; protrusion above the thin band; "butterfly" topography; no Fleischer ring or Vogt striae; hydrops rare |
| Keratoglobus | Rare; globular (not conical) corneal ectasia; thinning limbus-to-limbus; associated with Ehlers-Danlos and blue sclera; non-progressive; higher risk of corneal rupture |
| Post-refractive surgery ectasia | History of LASIK/SMILE; iatrogenic, similar topographic appearance |
| Contact lens warpage | Topographic changes more arcuate; resolves with cessation of lens wear |
Treatment
Treatment follows a stepwise approach based on disease severity and progression:
Step 1 - Stop Eye Rubbing
All patients must be instructed to stop rubbing their eyes - this single behavioral modification can slow progression significantly.
Step 2 - Optical Correction
| Stage | Option |
|---|---|
| Mild (early) | Spectacles or soft contact lenses |
| Moderate | Rigid gas-permeable (RGP) contact lenses - provide a regular refracting surface over the irregular cone |
| Advanced | Scleral contact lenses (larger diameter, vault over the cone); hybrid lenses; piggyback systems |
Step 3 - Corneal Collagen Cross-Linking (CXL)
The only treatment that halts progression:
- Mechanism: Riboflavin (vitamin B2) photosensitizer is applied to the cornea, then ultraviolet-A (UVA) light is applied - this creates new covalent bonds between collagen fibrils, stiffening the cornea
- Standard (epi-off) protocol: 9 mm epithelial debridement → riboflavin drops for 30 min → UVA exposure for 30 min
- Epi-on (transepithelial): Less effective in older evidence, though recent meta-analyses (PMID: 40856685) continue comparing these approaches
- Efficacy: >90% success in halting progression; can sometimes reverse ectasia
- FDA approval: Ages 14 and older (off-label for younger children)
- Complication: Small risk of infection or corneal scarring (bandage contact lens used for ~3 days post-procedure; 1-2 weeks for stabilization)
- Indication: Documented progressive disease
Step 4 - Intracorneal Ring Segments (ICRS)
- Polymethylmethacrylate (PMMA) segments inserted into the corneal stroma via laser or mechanical channels (e.g., Intacs, Ferrara rings)
- Mechanically flattens the cone, reduces irregular astigmatism
- Facilitates contact lens tolerance in moderate-advanced cases
- Can be combined with CXL
- Does NOT halt progression on its own
Step 5 - Corneal Transplantation
Reserved for severe disease when contact lenses cannot be tolerated or no longer give satisfactory vision:
| Procedure | Details |
|---|---|
| Deep Anterior Lamellar Keratoplasty (DALK) | Partial thickness - replaces anterior stroma while preserving Descemet membrane and endothelium. Lower rejection risk. Contraindicated if prior hydrops (Descemet discontinuity) |
| Penetrating Keratoplasty (PK) | Full-thickness corneal replacement; used when DALK is not suitable or has failed |
- Outcomes may be compromised by residual astigmatism and anisometropia, often requiring contact lens correction even after transplant
- LASIK is absolutely contraindicated in keratoconus patients; pre-operative screening for KC is mandatory before any corneal refractive surgery
Prognosis
- Progression typically occurs over 5-10 years, then may stabilize
- Most patients with mild-moderate disease maintain functional vision with contact lenses
- Corneal transplant success rates are high (~90%), but residual optical correction is often still needed
- Quality of life is significantly impacted, particularly in advanced disease (PMID: 40877860)
Key Points Summary
- KC is a progressive non-inflammatory corneal ectasia - thinning + cone-shaped protrusion + irregular astigmatism
- Prevalence ~0.1-0.2%; bilateral but asymmetric; onset in teens/twenties
- Hallmark slit-lamp signs: Vogt striae, Fleischer ring, Munson sign, oil-droplet reflex
- Diagnosis confirmed with corneal topography/tomography (Pentacam)
- Stop eye rubbing is the most important behavioral intervention
- CXL halts progression and is first-line for progressive disease
- Contacts (RGP/scleral) are the backbone of vision rehabilitation
- Severe disease unresponsive to lenses → DALK or PK
- LASIK is absolutely contraindicated
- Acute hydrops = Descemet rupture → managed conservatively, not with emergency transplant
Sources: Kanski's Clinical Ophthalmology 10th ed.; Wills Eye Manual; Goldman-Cecil Medicine International Edition
Recent evidence note: A 2025 meta-analysis (PMID: 40856685) continues to compare epi-on vs. epi-off CXL - overall, epi-off remains more effective for halting progression. Deep learning tools are also emerging for earlier KC detection (PMID: 38300179).
This is a shared conversation. Sign in to Orris to start your own chat.