I have oral exam in surgery so explain me everything in the topic mentioned below refer all the surgery text book swarts everything i need detailed explanation and prepare me for oral exam i should answer every question please help Topic: Retroperitoneal Trauma
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material I need from multiple surgical textbooks (Maingot's, Fischer's Mastery of Surgery, Sabiston, Current Surgical Therapy, Mulholland & Greenfield's, and more) to write a comprehensive oral exam preparation guide. Let me compose the full answer now.
Retroperitoneal Trauma - Complete Oral Exam Guide
Sources: Maingot's Abdominal Operations | Fischer's Mastery of Surgery 8e | Sabiston Textbook of Surgery | Current Surgical Therapy 14e | Mulholland & Greenfield's Surgery 7e
1. ANATOMY OF THE RETROPERITONEUM
The retroperitoneum is the space posterior to the peritoneum, anterior to the posterior abdominal wall. It is an organ-rich, highly vascular region that is a major potential site for hemorrhage in both blunt and penetrating trauma.
Structures contained:
- Vascular: Abdominal aorta + all branches, IVC + tributaries, iliac vessels
- Solid organs: Kidneys, adrenal glands
- Hollow organs (secondary retroperitoneal): Duodenum (2nd, 3rd, 4th parts), ascending and descending colon, rectum, bladder (extraperitoneal portion)
- Other: Pancreas, ureters, lymphatics, sympathetic chains, lumbar plexus
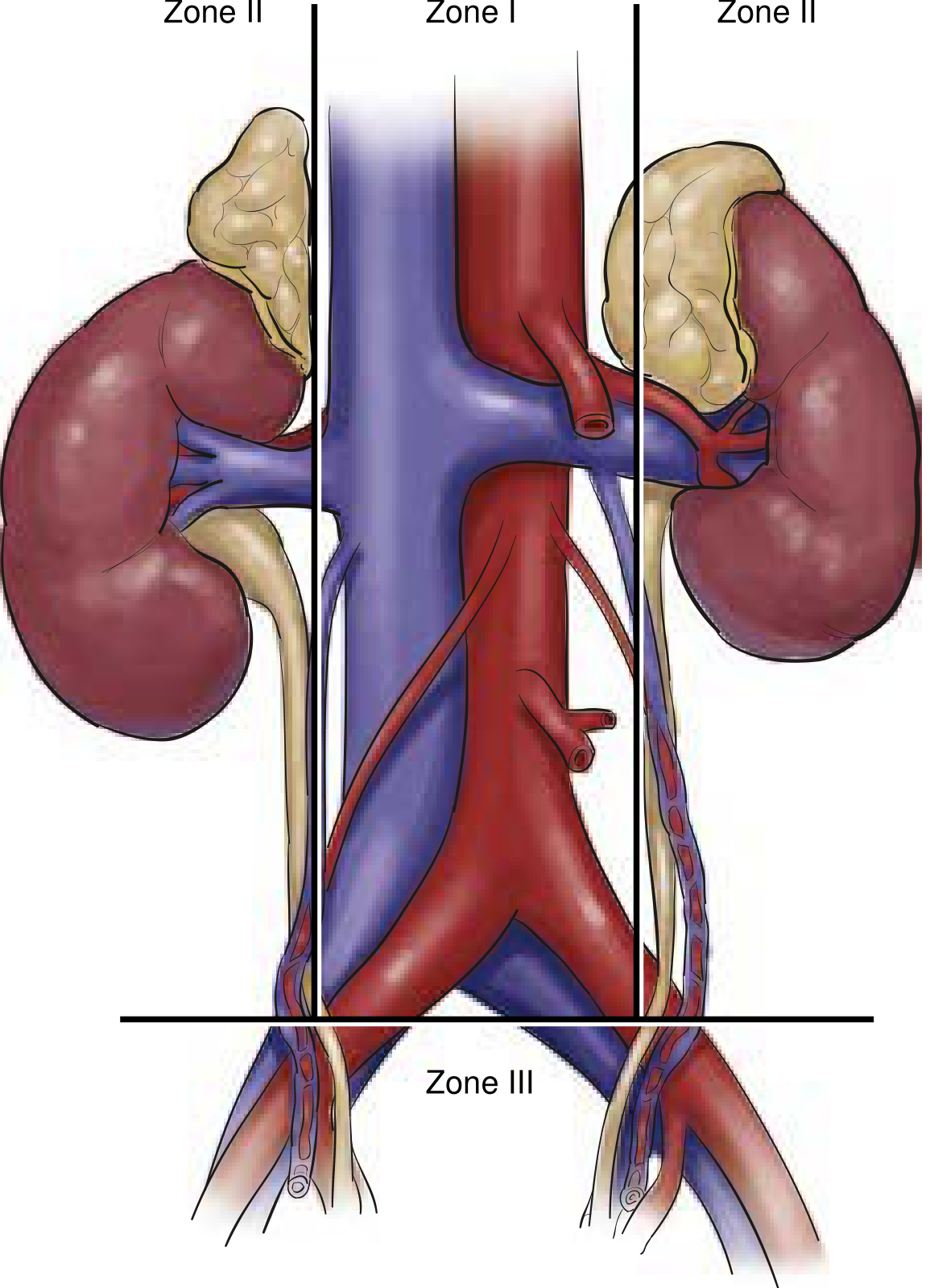
2. THE THREE ZONES OF THE RETROPERITONEUM
This is the single most important concept in retroperitoneal trauma. Every exam question on management is anchored to the zone system.
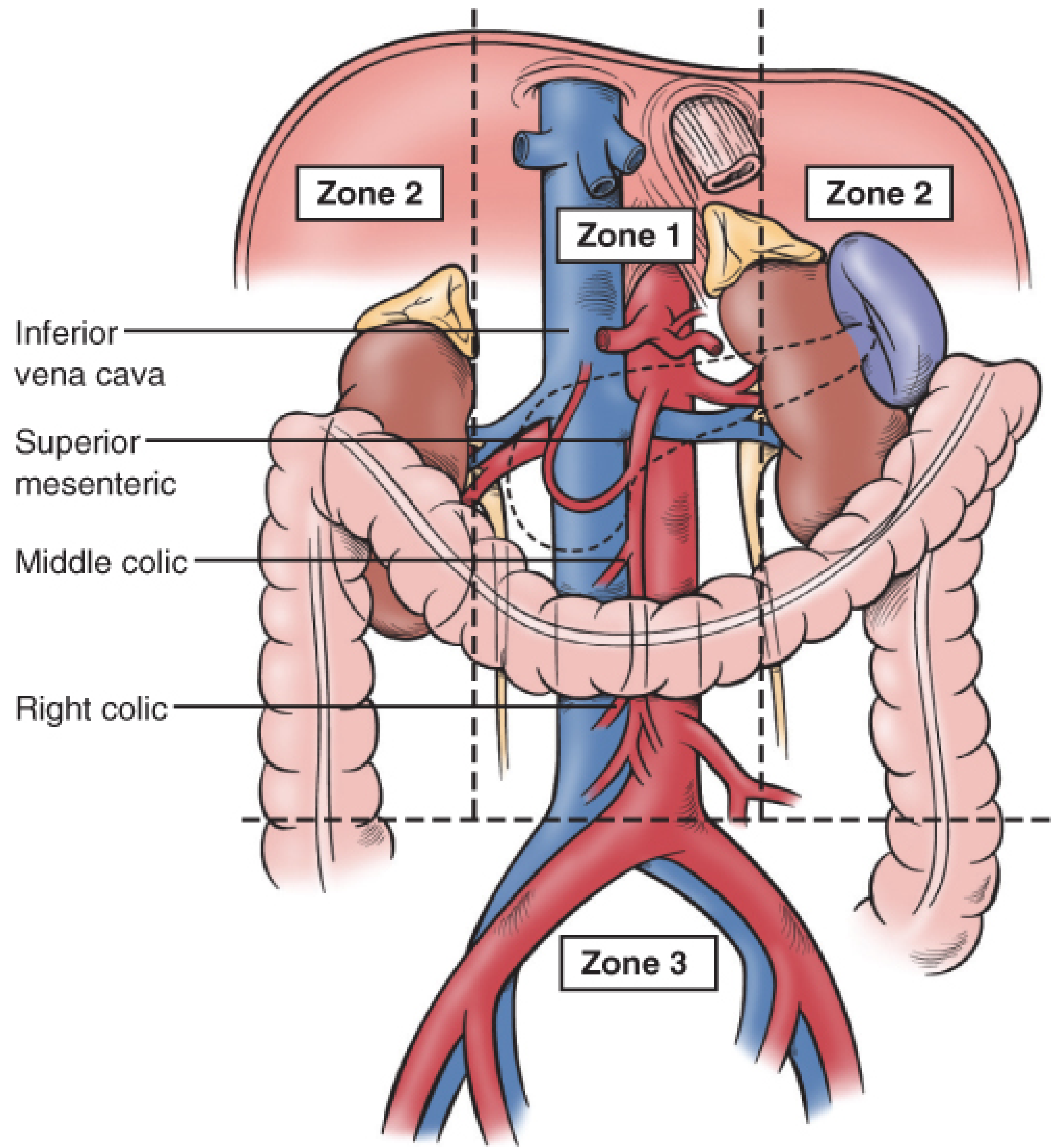
| Zone | Location | Structures |
|---|---|---|
| Zone I (Central) | Midline, from aortic hiatus to iliac bifurcation | Abdominal aorta, celiac axis, SMA origin, proximal renal vessels, IVC, proximal SMV |
| Zone II (Lateral) | Bilateral perirenal/flank regions | Kidneys, renal arteries and veins, adrenal glands, proximal ureters |
| Zone III (Pelvic) | Below iliac bifurcation | Common and external iliac arteries and veins, internal iliac vessels, pelvic venous plexus |
| Zone IV (some classifications) | Perihepatic | Retrohepatic IVC, hepatic veins |
Zone I is further divided by the transverse mesocolon:
- Supramesocolic Zone I: Suprarenal aorta, celiac axis, proximal SMA, suprarenal IVC, proximal SMV
- Inframesocolic Zone I: Infrarenal aorta, distal SMA, IMA, infrarenal IVC, distal SMV
3. THE GOLDEN RULE OF RETROPERITONEAL HEMATOMA MANAGEMENT
This is the most likely oral exam question. Memorize this table:
| Zone | Blunt Trauma | Penetrating Trauma |
|---|---|---|
| Zone I | ALWAYS explore | ALWAYS explore |
| Zone II | Selective (explore only if expanding/pulsatile) | ALWAYS explore |
| Zone III | Do NOT explore (unless exsanguinating) | ALWAYS explore |
| Zone IV (retrohepatic) | Do NOT explore | Do NOT explore |
The key principle: Obtain proximal (and where applicable, distal) control BEFORE opening any retroperitoneal hematoma.
Why not explore Zone III blunt hematomas?
Zone III blunt hematomas are almost always from pelvic fracture bleeding (venous plexus + cancellous bone). Opening the hematoma destroys the tamponade effect and can cause uncontrollable hemorrhage. These are better managed with pelvic binders, angioembolization, and pre-peritoneal packing.
Why always explore Zone I?
Zone I hematomas almost always involve the aorta, IVC, or proximal visceral vessels - injuries that are immediately life-threatening and cannot be controlled without direct surgical intervention.
4. MECHANISMS OF INJURY
Penetrating Trauma (Most Common Cause of Vascular Injuries)
- Gunshot wounds (GSWs): cause cavitating wounds due to high-velocity projectiles and associated shockwaves. These typically result in vessel thrombosis along with hemorrhage.
- Stab wounds: direct, lower-energy injury
- All penetrating retroperitoneal injuries require exploration regardless of zone (except Zone IV retrohepatic hematoma)
Blunt Trauma
- Motor vehicle accidents, falls, crush injuries
- Less commonly causes major vascular injury
- Renal injuries are the most common retroperitoneal organ injury from blunt mechanism
- Zone III blunt hematomas are typically from pelvic fractures with dissection of blood superiorly
5. CLINICAL PRESENTATION & DIAGNOSIS
Clinical Signs
- Tachycardia, hypotension, narrowed pulse pressure (hallmarks of hemorrhagic shock)
- Abdominal tenderness, distension, peritonitis
- Grey Turner's sign: Flank ecchymosis (retroperitoneal hemorrhage tracking to flank) - delayed sign
- Cullen's sign: Periumbilical ecchymosis - delayed sign
- Unilateral loss of femoral pulse: Concerning for iliac artery or aortic injury
- Gross or microscopic hematuria: suggests renal or ureteric injury
- Pelvic instability on examination: suggests pelvic fracture with Zone III hematoma
- Seat belt sign
Investigations
In Hemodynamically Stable Patient:
- CT scan with IV contrast (triple-phase) is the investigation of choice
- Arterial phase: identifies arterial bleeding, pseudoaneurysm, occlusion, dissection, AV fistula
- Nephrogram phase: renal parenchymal injury
- Delayed/excretory (pyelogram) phase: pathognomonic - contrast extravasation identifies renal pelvis or ureteric injury
- Also identifies trajectory of GSW
In Hemodynamically Unstable Patient:
- FAST exam (Focused Assessment with Sonography in Trauma): identifies free fluid but has poor accuracy for diagnosing major vascular trauma
- Diagnostic Peritoneal Lavage (DPL): Rarely used now, but useful in unstable patient with equivocal FAST. Gross blood or succus = immediate laparotomy
- Plain X-ray: Radio-opaque markers (paper clips) to determine GSW trajectory; pelvic fractures
Labs:
- CBC, type and cross, basic chemistry, lactate, ABG/VBG
- Thromboelastography (TEG): Guides coagulation status and resuscitation
Single-shot IVP (Intravenous Pyelogram):
- Useful intraoperatively to confirm presence of contralateral kidney before nephrectomy
- No longer routinely used (hydration-dependent, less detail than CT)
- Still used in unstable patients going directly to OR
6. OPERATIVE MANAGEMENT
Initial Steps (Damage Control Approach)
- Standard midline laparotomy from xiphoid to pubic symphysis - gives access to all four quadrants
- Evacuate blood and pack all four quadrants
- Systematically survey for active bleeding
- Initial hemorrhage control: Packing + digital pressure, then more extensive exposure for proximal and distal vascular control
- For arteries: vascular clamps; for major veins: sponge sticks (preferred to avoid tearing thin venous walls)
- Control enteric injuries with oversewing or bowel clamps to prevent contamination
- Then proceed to definitive repair based on patient stability
Key Surgical Exposures (HIGH-YIELD for Oral Exam)
MATTOX MANEUVER (Left Medial Visceral Rotation)
- Indication: Supramesocolic Zone I hematoma; aorta and left-sided retroperitoneal structures
- Technique: Incise the white line of Toldt along the descending colon, curving around the spleen and gastroesophageal junction. Rotate left colon, distal pancreas, spleen, stomach fundus, and left kidney medially
- Exposes: Entire abdominal aorta, celiac axis, SMA, left renal artery, IMA, aortic bifurcation and iliac arteries
- Proximal control: Supraceliac aorta clamped at the diaphragmatic hiatus
CATTELL-BRAASCH MANEUVER (Right Medial Visceral Rotation)
- Indication: IVC injuries, right-sided Zone I hematoma, infrarenal vasculature, right renal hilum
- Technique: Take down white line of Toldt along ascending colon + wide Kocher maneuver (mobilize duodenum and pancreatic head medially) + incise small bowel mesentery along ileocecal junction toward ligament of Treitz
- Exposes: Infrarenal IVC, common iliac veins, infrarenal aorta, right renal hilum
KOCHER MANEUVER
- Mobilization of duodenum and pancreatic head to expose retroduodenal structures and right renal hilum
Inframesocolic Zone I Exposure
- Reflect small bowel to the right, transverse colon cephalad
- Take down ligament of Treitz
- Left renal vein is encountered, then infrarenal aorta can be exposed
7. ZONE-SPECIFIC MANAGEMENT IN DETAIL
Zone I Management
- ALWAYS requires exploration (blunt or penetrating)
- Proximal control first - supraceliac aorta clamped at the diaphragm
- If hematoma extends to aortic hiatus: may require surgical control of thoracic aorta or placement of REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta)
- Supramesocolic: Mattox maneuver
- IVC bleeding (supramesocolic): Right visceral rotation (Cattell-Braasch)
- Inframesocolic: Small bowel reflected right, transverse colon cephalad
Aortic injuries: Primary repair preferred; interposition graft for extensive injuries
IVC injuries: Primary repair if possible. If primary repair would cause >30% luminal narrowing, use patch angioplasty. Infrarenal IVC can be ligated as a last resort (risk of leg edema/DVT, not immediately fatal).
IVC injuries: Primary repair if possible. If primary repair would cause >30% luminal narrowing, use patch angioplasty. Infrarenal IVC can be ligated as a last resort (risk of leg edema/DVT, not immediately fatal).
Zone II Management
- Penetrating: Always explore - approach depends on side
- Blunt: Selective - explore only if expanding or pulsatile hematoma (signs of arterial injury)
- A rapidly expanding Zone II hematoma or pulsatile hematoma may indicate need for nephrectomy
- Signs that nephrectomy may be indicated: rapidly expanding Zone II hematoma or pulsatile hematoma
- First confirm presence of contralateral functioning kidney (single-shot IVP or CT)
Zone III Management
- Blunt: Do NOT explore - tamponade is protective; exploring destroys the effect and releases retroperitoneal pressure
- Management: pelvic binders, angioembolization (interventional radiology), pre-peritoneal pelvic packing (PPP)
- Penetrating: Always explore
- REBOA (Zone III) can provide temporary hemorrhage control
8. SPECIFIC ORGAN INJURIES
Renal Injuries (Most Common Retroperitoneal Solid Organ)
AAST Renal Injury Grading Scale:
| Grade | Description |
|---|---|
| I | Contusion or non-expanding subcapsular hematoma, no laceration |
| II | Non-expanding perirenal hematoma, cortical laceration <1 cm depth without urinary extravasation |
| III | Cortical laceration >1 cm depth without collecting system rupture |
| IV | Laceration through cortex, medulla, collecting system; or vascular injury with contained hemorrhage |
| V | Shattered kidney; or vascular avulsion |
Management:
- Grade I-III (blunt): Non-operative management (NOM) - bed rest, serial imaging
- Grade IV-V (penetrating): Typically require nephrectomy, especially with viable contralateral kidney
- Interventional radiology (angioembolization) has largely supplanted isolated nephrectomy for segmental arterial bleeding
- Unstable patients with active bleeding from kidney/renal hilum: operative intervention
- Renorrhaphy: For lacerations/superficial wounds - approximate disrupted capsule with pledgeted sutures or prosthetic (mesh) wrap, drain all repairs
- Partial nephrectomy: When injury pattern permits
Diagnosis of Renal Injury:
- CT with IV contrast (triple phase)
- Hematuria on UA: even children (<16 years) should undergo CT urogram if >50 RBC/HPF
- Renal vein injuries have lowest detection sensitivity on CT of all hilar structures - be vigilant
Ureteric Injuries
- Subtle, often missed
- Identified on the delayed phase of CT (contrast extravasation = pathognomonic of renal pelvis or ureteric injury)
- Gross hematuria, urinoma, or hydronephrosis may suggest ureteric injury
- Intraoperative: Cystoscopy + retrograde pyelogram when suspected and no pre-op imaging
- Primary repair: Interrupted absorbable suture over double-J stent; spatulate ends if complete transection; drain the repair
- If tension-free anastomosis not possible: Boari flap (bladder flap) + psoas hitch
- All ureteric repairs should be adequately drained
Duodenal and Pancreatic Injuries
- Located in Zone I retroperitoneum (2nd, 3rd, 4th portions of duodenum; body/head of pancreas)
- High-energy blunt trauma (handlebar injury, steering wheel) can cause deceleration injury
- Duodenal hematoma: Conservative management (NGT decompression, TPN); operative management if obstruction persists >2 weeks
- Duodenal perforation: Repair + drain; Pyloric exclusion for severe injuries
- Pancreatic injury: Distal pancreatectomy for body/tail; drainage for head injuries
Bladder Injuries
- Extraperitoneal: Most common in pelvic fractures; managed with urinary catheter + bladder decompression. May require operative repair if extensive or if anterior pelvic ring stabilization needed (risk of hardware contamination)
- Intraperitoneal: Classic repair in two-layer fashion with absorbable suture + catheter decompression
Adrenal Injuries
- Usually managed non-operatively
- Bilateral adrenal injuries may require steroid supplementation
9. DAMAGE CONTROL SURGERY IN RETROPERITONEAL TRAUMA
The "lethal triad" (hypothermia + acidosis + coagulopathy) drives the damage control approach.
Damage Control Stages:
- Phase 0 (Pre-hospital): Hemorrhage control, rapid transport
- Phase I (OR): Abbreviated surgery - control hemorrhage (pack/ligate/shunt), control contamination, close abdomen temporarily
- Phase II (ICU): Resuscitation - warm, correct coagulopathy with MTP (massive transfusion protocol), reverse acidosis
- Phase III (Planned re-op): Definitive repair (anastomoses, definitive vascular repair, remove packs)
Damage control options for vascular injuries:
- Ligation: For vessels that can be sacrificed (e.g., infrarenal IVC, internal iliac)
- Temporary Intravascular Shunt (TIVS): Maintains flow, buys time for resuscitation
- REBOA: Endovascular balloon occlusion at three zones:
- Zone I REBOA (descending thoracic aorta): For abdominal/pelvic hemorrhage
- Zone III REBOA (infrarenal aorta): For pelvic hemorrhage
10. PELVIC FRACTURE AND ZONE III HEMORRHAGE
This is a major subtopic for oral exams.
Types of pelvic fractures (by instability):
- Open book fracture (AP compression)
- Lateral compression
- Vertical shear (most unstable/deadly)
Source of bleeding in pelvic fractures:
- 80-85%: Venous plexus + cancellous bone (low pressure, self-tamponading)
- 15-20%: Arterial (superior gluteal artery most common)
- Both together in severe injuries
Management sequence of hemodynamically unstable pelvic fracture:
- Pelvic binder (immediate - circumferential compression, reduces volume, tamponades venous bleeding)
- Note: External fixation only provides anterior compression and can paradoxically open the posterior pelvis and worsen hemorrhage
- Massive Transfusion Protocol (1:1:1 ratio pRBC:FFP:platelets)
- CT angiography (if hemodynamically stable)
- Angioembolization (for arterial bleeding on CT) - primary tool for arterial Zone III hemorrhage
- Pre-peritoneal pelvic packing (PPP): If angioembolization unavailable/unsuccessful and patient remains unstable - pack anterior to peritoneum, tamponade pelvic space
- Definitive pelvic fixation: Ideally within 12-36 hours once stabilized - improves pulmonary hygiene, early mobilization, hemostasis
- REBOA (Zone III): As bridge to angioembolization
11. RESUSCITATIVE ENDOVASCULAR BALLOON OCCLUSION OF THE AORTA (REBOA)
- Introduced as adjunct for temporary hemorrhage control in Non-Compressible Torso Hemorrhage (NCTH)
- Used in trauma since the Korean War
- More widespread use in tertiary trauma centers
- Mechanism: Balloon inflated in aorta proximal to injury - redirects blood to heart/brain, reduces distal hemorrhage
- Three zones of deployment:
- Zone I (descending thoracic aorta, T4-T7): Abdominal and pelvic hemorrhage
- Zone II (NOT used - too close to renal vessels/visceral aorta)
- Zone III (infrarenal aorta, L1-L4): Pelvic/junctional hemorrhage
- Role remains controversial in prehospital and ED settings
12. ABDOMINAL VASCULAR INJURIES - HIGH-YIELD SUMMARY
| Vessel | Key Points |
|---|---|
| Suprarenal aorta | Highest mortality; requires supraceliac clamping; Mattox maneuver |
| Infrarenal aorta | Mattox or direct exposure; primary repair or interposition graft |
| Celiac axis | Can be ligated if necessary (rich collateral supply) |
| SMA | Must be repaired/reconstructed - ligation leads to bowel ischemia |
| IMA | Can be ligated (collateral supply via marginal artery) |
| IVC (suprarenal) | Highest operative mortality of all abdominal vessel injuries; difficult exposure |
| IVC (infrarenal) | Cattell-Braasch; primary repair if possible; can ligate if necessary |
| Renal artery | Revascularize if possible (warm ischemia limit ~4-6 hours); nephrectomy if reconstruction not feasible |
| Renal vein (left) | Can ligate close to IVC (adrenal and gonadal collaterals decompress) |
| Renal vein (right) | Cannot safely ligate (no adequate collaterals) - must repair |
| Iliac artery | External iliac must be repaired; internal iliac can be ligated |
| Iliac vein | Primary repair preferred; ligation as last resort |
13. LIKELY ORAL EXAM QUESTIONS AND MODEL ANSWERS
Q1: What are the three zones of the retroperitoneum and what do they contain?
Zone I is central (midline, aortic hiatus to iliac bifurcation) containing the aorta, IVC, and proximal visceral vessels. Zone II is lateral (bilateral perirenal) containing the kidneys, renal vessels, and adrenals. Zone III is pelvic (iliac bifurcation to pelvis) containing the iliac vessels. Some add Zone IV for the retrohepatic IVC.
Q2: What is the management of a retroperitoneal hematoma found at laparotomy?
Zone I - always explore regardless of mechanism. Zone II - always explore for penetrating injury; selective for blunt (explore only if expanding or pulsatile). Zone III - always explore for penetrating; do NOT explore for blunt (unless exsanguinating). Zone IV - do not explore. Always achieve proximal (and distal) control before opening any hematoma.
Q3: A patient is brought in after an RTA with hypotension, tachycardia, and pelvic instability. FAST is negative. What is your management?
Pelvic fracture with Zone III retroperitoneal hematoma causing hemorrhagic shock. Immediately apply pelvic binder, start MTP (1:1:1), obtain CXR and pelvic X-ray. If stable enough - CT angiography to identify arterial bleeding, then angioembolization. If unstable despite initial measures - pre-peritoneal pelvic packing, consider REBOA Zone III. Do NOT perform exploratory laparotomy and open the Zone III hematoma in blunt trauma (destroys tamponade).
Q4: What is the Mattox maneuver? When do you use it?
Left medial visceral rotation. Performed by incising the white line of Toldt from the descending colon curving around the spleen and GEJ, rotating the left colon, distal pancreas, spleen, stomach, and left kidney medially. Used to expose the entire abdominal aorta, celiac axis, SMA, left renal artery for supramesocolic Zone I hematomas and aortic injuries.
Q5: What is the Cattell-Braasch maneuver?
Right medial visceral rotation. Involves taking down the white line of Toldt along the ascending colon, wide Kocher maneuver, and incising the small bowel mesentery at the ileocecal junction toward the ligament of Treitz. Exposes the IVC, common iliac veins, infrarenal aorta, and right renal hilum.
Q6: How do you diagnose ureteric injury?
Delayed/excretory phase of CT urogram - contrast extravasation is pathognomonic. Signs include gross hematuria, urinoma, and hydronephrosis. Intraoperatively, cystoscopy + retrograde pyelogram if no pre-op imaging. Single-shot IVP identifies contralateral kidney but has limitations.
Q7: Why can the left renal vein be ligated near the IVC but not the right?
The left renal vein has collateral drainage via the left adrenal vein and left gonadal vein, which allow venous decompression. The right renal vein is short with no significant collaterals, so ligation causes renal venous hypertension and infarction.
Q8: What is Grey Turner's sign?
Flank ecchymosis indicating retroperitoneal hemorrhage tracking to the flanks. It is a delayed sign (may appear 24-48 hours after injury). Associated sign: Cullen's sign (periumbilical ecchymosis).
Q9: What is REBOA and in what zones is it deployed?
Resuscitative Endovascular Balloon Occlusion of the Aorta - a balloon catheter placed endovascularly to temporarily occlude the aorta, redirecting blood to the heart and brain while reducing distal hemorrhage. Zone I (descending thoracic aorta) for abdominal hemorrhage; Zone III (infrarenal aorta) for pelvic hemorrhage. Zone II is not used.
Q10: What determines whether to ligate or repair the SMA vs IMA in trauma?
SMA must be repaired or reconstructed - ligation causes massive small bowel ischemia and infarction (no adequate collaterals). The IMA can be ligated because of rich collateral supply via the marginal artery of Drummond and middle colic artery from the SMA. Similarly, the celiac axis can be ligated due to collaterals via the gastroduodenal artery.
14. COMPLICATIONS
- Delayed hemorrhage: Pseudoaneurysm, AV fistula (especially after NOM of renal injuries)
- Urinoma: Post-traumatic urine collection from unrecognized ureteric injury
- Post-traumatic ileus / paralytic ileus: Classic complication of retroperitoneal irritation (blood/urine in retroperitoneum)
- Abdominal compartment syndrome: After massive resuscitation and temporary abdominal closure
- OPSS (Overwhelming Post-Splenectomy Sepsis): If splenectomy performed - vaccinate against pneumococcus, Hib, meningococcus
- Pelvic sepsis: From missed rectal injuries in Zone III penetrating trauma
- DVT/PE: Common after pelvic fractures; anti-coagulation is challenging given ongoing hemorrhage risk
Quick Memory Aid for Zones:
"Zone 1 = Always open (pipes are broken) | Zone 2 = Penetrating always, Blunt only if expanding | Zone 3 blunt = NEVER open (the tamponade is your friend)"
- Maingot's Abdominal Operations, p. 1272
- Fischer's Mastery of Surgery 8e, p. 7069-7076
- Sabiston Textbook of Surgery, p. 988-996
- Current Surgical Therapy 14e, p. 1369
- Mulholland & Greenfield's Surgery 7e, p. 1380
This is a shared conversation. Sign in to Orris to start your own chat.