endometriosis
Reading File
Finding Sources
Searching PubMed
endometriosis
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive material to write a complete, well-illustrated answer. Here it is:
Endometriosis
Definition
Endometriosis is defined by the presence of endometrial glands and stroma in extrauterine locations. It is a common, chronic inflammatory condition affecting an estimated 5-10% of women of reproductive age, and nearly half of women with infertility.
- Robbins & Kumar Basic Pathology, p. 689
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1602
Types
| Type | Description |
|---|---|
| Superficial peritoneal | Most common; implants on peritoneal surfaces |
| Ovarian endometriosis | Endometriomas ("chocolate cysts") filled with brown, tar-like fluid |
| Deep infiltrating endometriosis (DIE) | Tissue extending >5 mm below the peritoneum; involves uterosacral ligaments, vagina, bowel, bladder, ureters |
Risk of malignant transformation is mainly confined to deep infiltrating endometriosis.
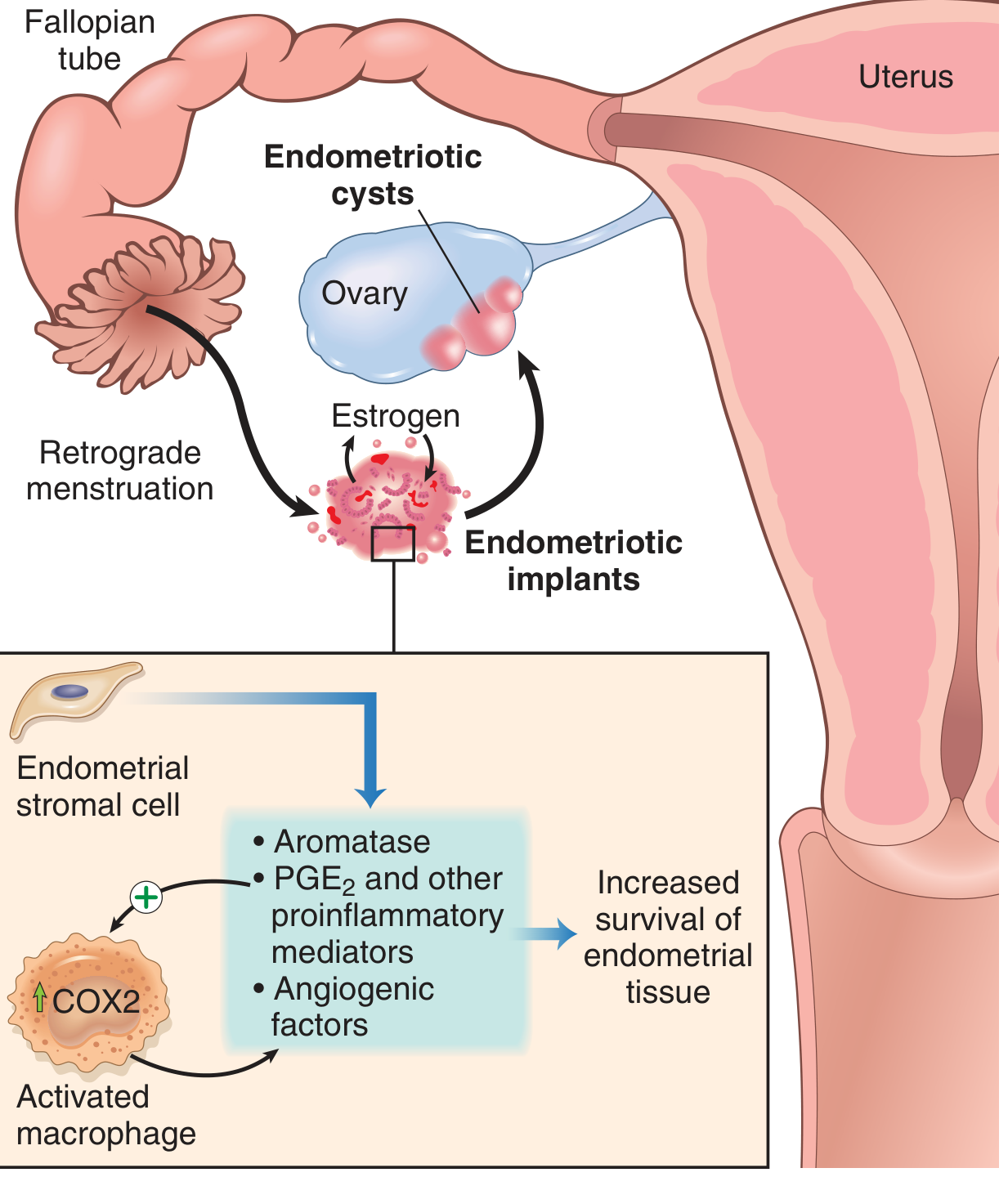
Pathogenesis
The mechanism remains incompletely understood. Four major theories exist:
- Regurgitation theory (Sampson's theory) - most widely accepted: menstrual tissue flows retrograde through the fallopian tubes and implants at ectopic sites.
- Benign metastasis theory: endometrial tissue spreads via blood vessels and lymphatics to distant sites (lung, brain, bone).
- Metaplastic theory: coelomic epithelium (from which the Mullerian ducts originate) undergoes metaplastic transformation into endometrial-like tissue.
- Extrauterine stem/progenitor cell theory: bone marrow-derived stem cells differentiate into endometrial tissue.
Once implanted, lesions are not passively inert. They produce elevated levels of aromatase (generating local estrogen from androgens), prostaglandin E2 (PGE2), VEGF, and matrix metalloproteinases (MMPs) - creating a self-sustaining, estrogen-driven, proinflammatory environment that promotes survival and growth of implants.
Sites of Involvement
Pelvic (most common):
- Ovaries, pouch of Douglas, uterosacral ligaments, fallopian tubes, pelvic peritoneum
Extrapelvic (less common):
- Gastrointestinal tract (sigmoid colon, rectum, small bowel - 12-37% of cases)
- Urinary tract (bladder, ureters)
- Lungs/diaphragm (can cause catamenial haemoptysis or pneumothorax)
- Umbilicus, laparotomy scars
Gross and Microscopic Appearance
Classic ("powder burn") lesions: black, dark brown, or bluish puckered nodules or small cysts on serosal surfaces - reflecting old haemorrhage surrounded by fibrosis.
Atypical/subtle lesions: red flame-like implants, vesicular lesions, clear serous vesicles, white plaques - these are easily missed.
Endometriomas: ovarian cysts 3-5 cm in diameter, filled with thick dark brown ("chocolate") fluid; densely adherent to the ovarian fossa. Reported in 17-44% of women with endometriosis.
Deep disease: fibrotic nodules and adhesion bands that can obliterate the pouch of Douglas, distort pelvic anatomy, and involve the bowel wall (mimicking cancer).
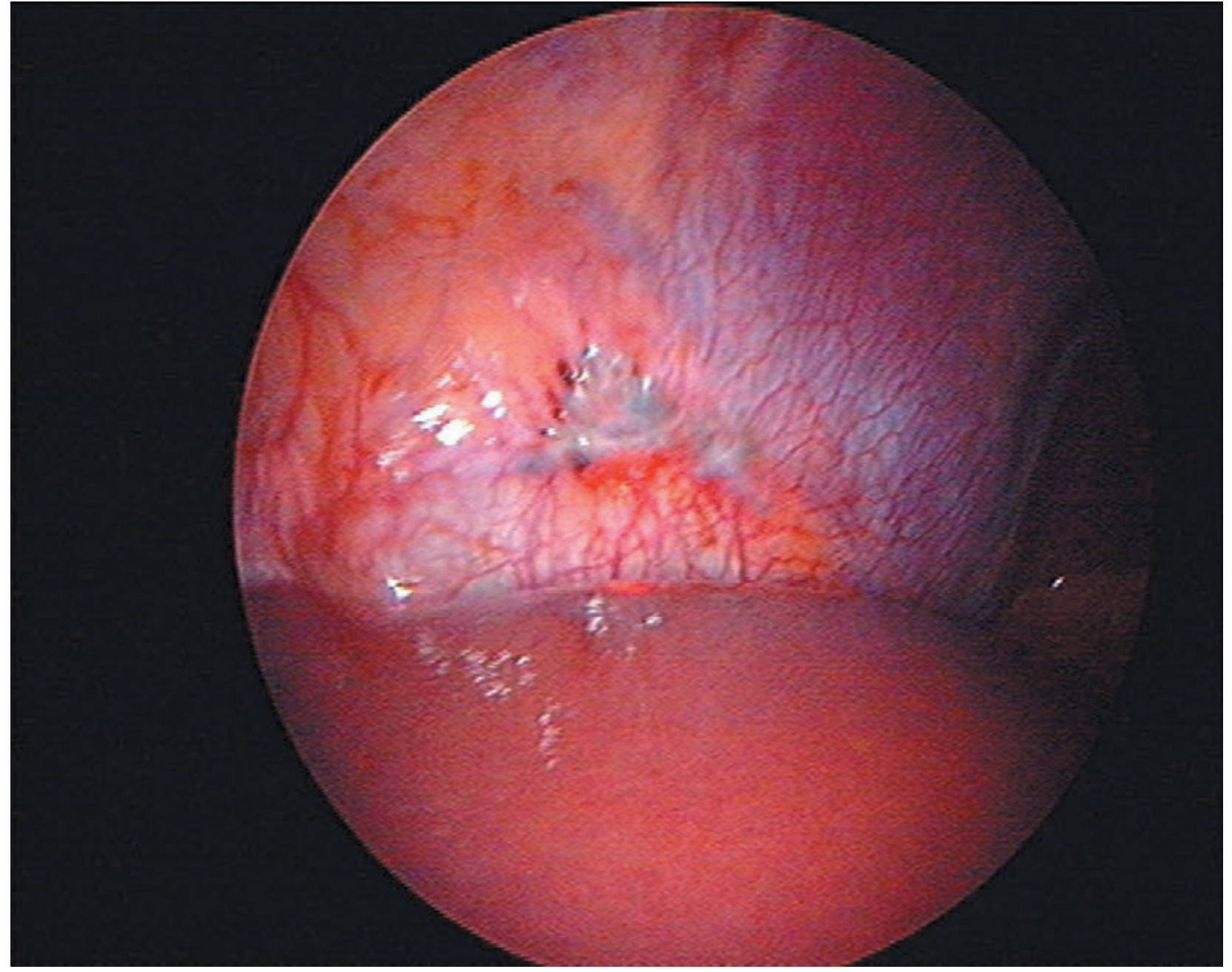
Laparoscopic views - endometriosis on the peritoneal surface of the diaphragm:
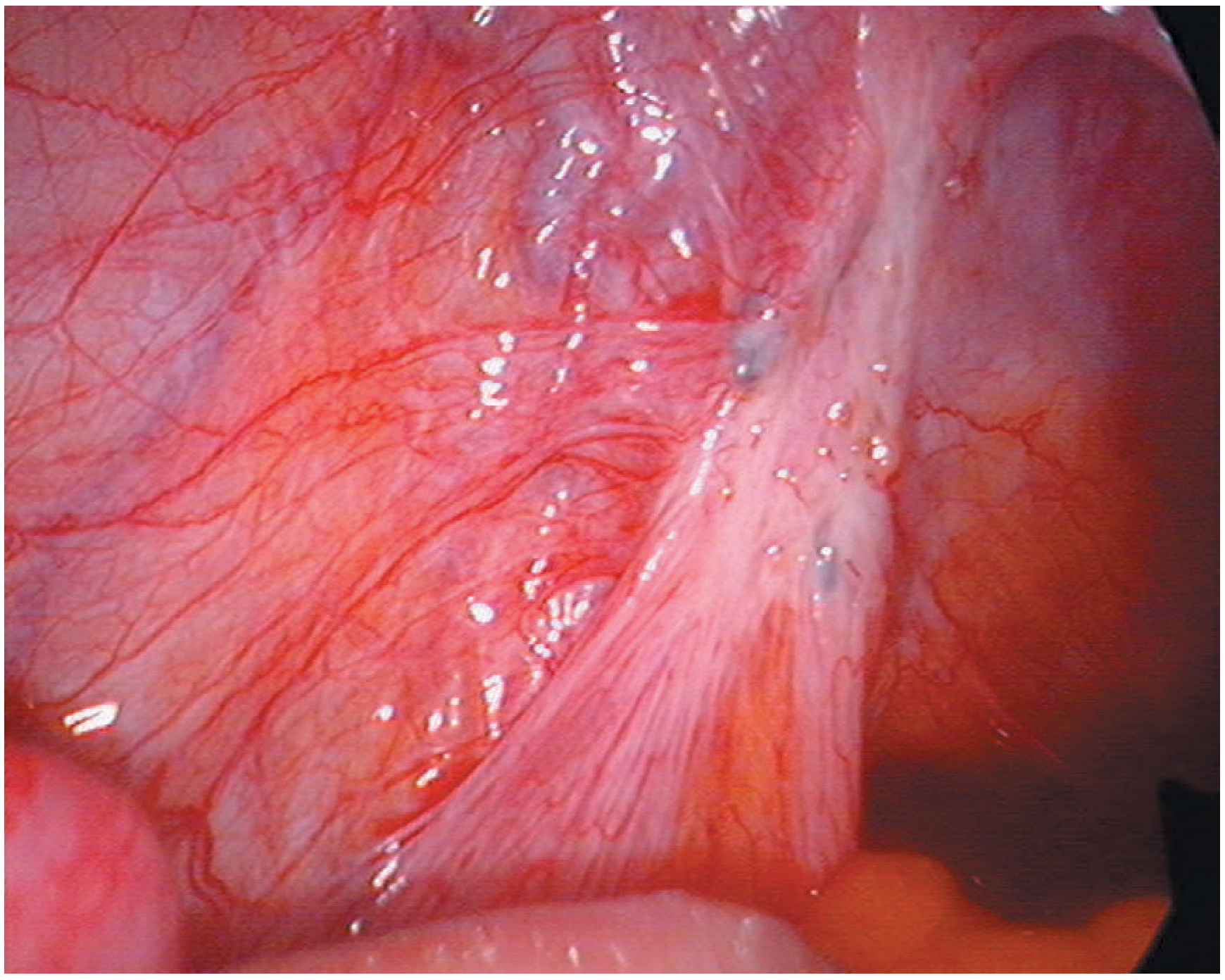
Uterosacral ligament involvement with dense fibrosis:
Symptoms
Endometriosis may be asymptomatic in a significant proportion of women. When symptomatic:
- Dysmenorrhoea (most common)
- Chronic pelvic pain (cyclical and non-cyclical)
- Deep dyspareunia (pain during intercourse)
- Dyschezia (pain on defaecation) - suggests bowel involvement
- Dysuria / haematuria - suggests bladder involvement
- Infertility
- Fatigue
- Catamenial haemoptysis or pneumothorax - with thoracic involvement
Note: there is poor correlation between disease extent/staging and symptom severity.
Diagnosis
Gold standard: laparoscopy with histological confirmation.
- Clinical examination may reveal pelvic tenderness, a fixed retroverted uterus, tender uterosacral ligaments, or enlarged ovaries. Deeply infiltrating nodules in the pouch of Douglas or visible vaginal lesions ("blue-domed" cysts in the posterior fornix) are strongly suggestive.
- Transvaginal ultrasound (TVUS): reliably detects endometriomas and severe pelvic DIE; misses superficial implants.
- MRI: best non-invasive modality for mapping DIE; detects haemosiderin deposits and low-signal fibrotic plaques; can demonstrate obliteration of the pouch of Douglas and rectosigmoid involvement.
- Sigmoidoscopy: useful when bowel involvement is suspected to assess depth and distance from anal verge (important for surgical planning).
MRI showing deep endometriotic rectovaginal nodule with obliteration of the pouch of Douglas:
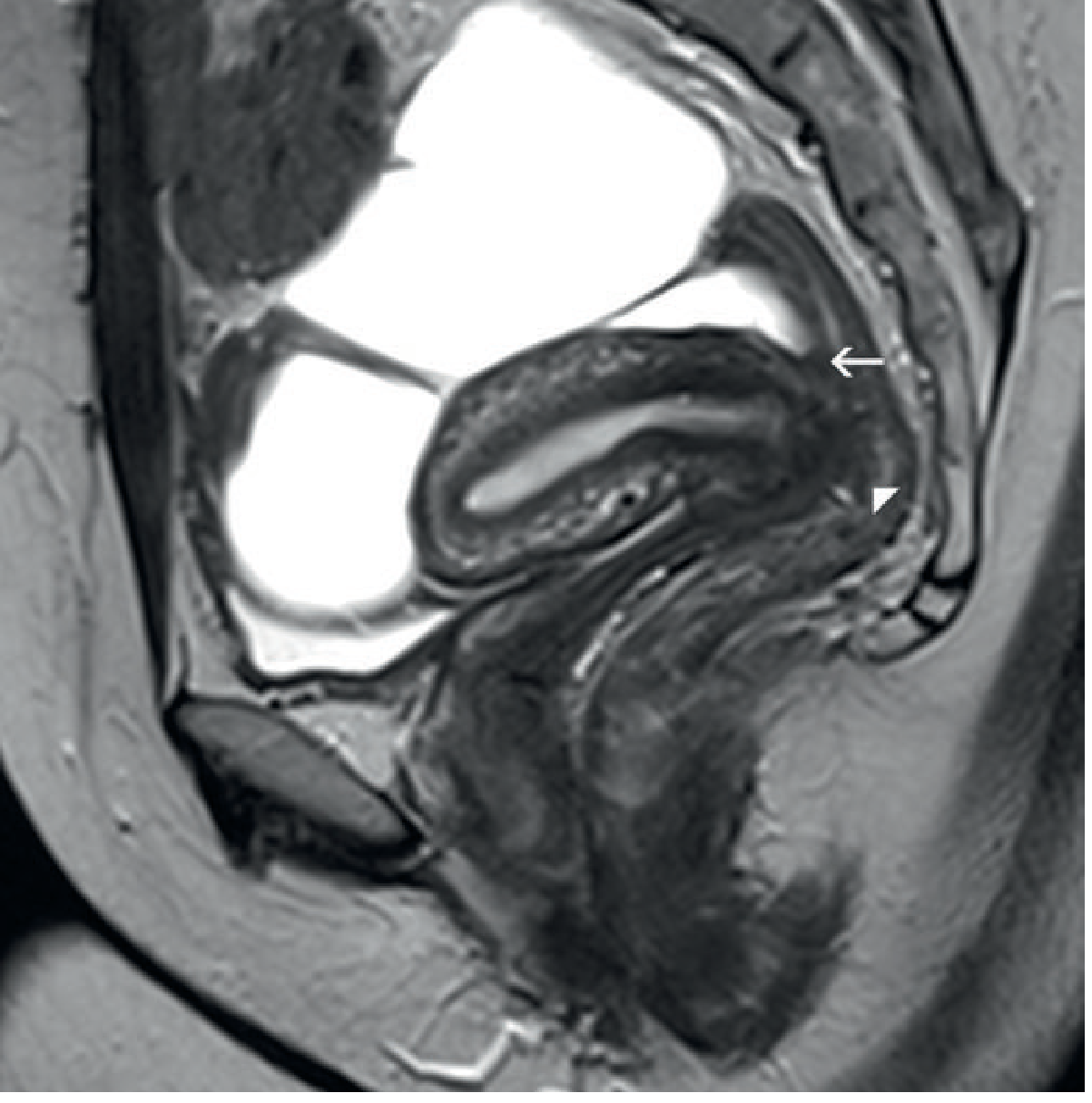 Sagittal T2-weighted pelvic MRI: low-signal nodularity obliterating the pouch of Douglas (arrow), with tethering and angulation of the rectal wall to a deep rectovaginal endometriotic nodule (arrowhead). (Grainger & Allison's Diagnostic Radiology)
Sagittal T2-weighted pelvic MRI: low-signal nodularity obliterating the pouch of Douglas (arrow), with tethering and angulation of the rectal wall to a deep rectovaginal endometriotic nodule (arrowhead). (Grainger & Allison's Diagnostic Radiology)
Treatment
Treatment options are influenced by the patient's desire for fertility, symptom severity, and disease extent.
1. Conservative (watchful waiting)
- Appropriate for asymptomatic or mildly symptomatic women.
2. Medical Management
| Agent | Mechanism |
|---|---|
| NSAIDs / simple analgesia | First-line for pain relief |
| Combined oral contraceptive pill | Suppresses ovarian cycling |
| Progestogens (e.g., norethisterone, medroxyprogesterone) | Decidualise and atrophy implants |
| Levonorgestrel IUS (Mirena) | Local progestogenic effect; reduces dysmenorrhoea |
| GnRH agonists (e.g., leuprorelin, goserelin) | Induce medical pseudomenopause; used with add-back HRT to reduce bone loss |
| Aromatase inhibitors | Suppress local and systemic estrogen; used in refractory cases |
Hormonal therapies suppress but do not eradicate disease, and symptoms often recur after stopping.
3. Surgical Management
- Laparoscopic ablation or excision of implants - preferred approach; restores anatomy.
- For endometriomas: drainage with directed ablation preferred over cystectomy to preserve ovarian reserve.
- For bowel DIE: shaving (superficial removal), disc excision, or segmental resection - depending on depth; low rectal lesions (5-8 cm from the anal verge) carry higher anastomotic leak risk.
- Definitive surgery: total hysterectomy + bilateral salpingo-oophorectomy + excision of all disease - reserved for women who have completed their family. Offers best chance of cure but does not guarantee it.
Surgical risks include bowel/bladder/ureteric injury (2 in 1,000), ureteric stricture leading to hydronephrosis, fistula formation (with repeated bowel shavings), and anastomotic leak.
Endometriosis and Infertility
Endometriosis is found in approximately 40-50% of infertile women. Proposed mechanisms include:
- Distortion of pelvic anatomy / adhesions impeding tubal pick-up
- Impaired folliculogenesis and oocyte quality
- Altered peritoneal fluid environment (inflammatory cytokines)
- Endometrial receptivity defects
Surgical treatment of endometriomas and adhesions can improve spontaneous conception rates. In vitro fertilisation (IVF) is recommended for those who fail to conceive after conservative surgery.
Recent Evidence (2024-2025)
- A 2024 systematic review (PMID 39067455) in Human Reproduction Update highlighted fibrosis as a key driver of endometriosis progression and pain, with emerging anti-fibrotic strategies under investigation.
- A 2025 meta-analysis (PMID 39946383) in PLoS One found physical activity and exercise significantly reduced pain intensity and improved quality of life in women with endometriosis, supporting it as a complementary management strategy.
Sources:
- Robbins & Kumar Basic Pathology, p. 689
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1602-1604
- Grainger & Allison's Diagnostic Radiology, p. 591
- PubMed: PMID 39067455, 39946383
This is a shared conversation. Sign in to Orris to start your own chat.