I now have comprehensive, authoritative content from multiple textbooks (Guyton, Tintinalli, Harrison's, Braunwald's, Morgan & Mikhail, and others) plus four key clinical images. Let me now compose the complete, exam-ready answer.
Ventricular Fibrillation (VF) - Complete MBBS/NEET PG Study Guide
Sources: Guyton & Hall Medical Physiology, Harrison's Principles (22e, 2025), Tintinalli's Emergency Medicine, Braunwald's Heart Disease, Morgan & Mikhail's Clinical Anesthesiology
1. Definition of Ventricular Fibrillation
Simple explanation first: Imagine your heart's ventricles - instead of squeezing together as a team, every small patch of muscle starts firing on its own, randomly, chaotically. No coordinated pump. No output. No life - unless fixed within minutes.
Formal definition (exam-ready):
Ventricular fibrillation is a life-threatening cardiac arrhythmia characterized by disorganized, chaotic electrical depolarization of the ventricular myocardium resulting in absent coordinated ventricular contraction, zero effective cardiac output, and cardiac arrest.
- Ventricular rate: 300-500 disorganized impulses per minute (no true "rate" - just chaos)
- There is no identifiable P wave, QRS complex, or T wave
- The result is the same as cardiac standstill: no blood is pumped
"The most serious of all cardiac arrhythmias is ventricular fibrillation, which is almost invariably fatal if not stopped within 1 to 3 minutes." - Guyton & Hall Medical Physiology
2. Normal Cardiac Electrical Conduction and How VF Develops
Normal conduction (the baseline you need to know):
SA Node (60-100 bpm)
↓
Atrial myocardium (P wave on ECG)
↓
AV Node (physiologic delay - allows atria to empty)
↓
Bundle of His
↓
Left Bundle Branch + Right Bundle Branch
↓
Purkinje Fibers (rapid spread - narrow QRS)
↓
Ventricular myocardium contracts uniformly (QRS complex)
↓
Repolarization (T wave)
↓
Refractoriness → impulse dies → waits for next SA node firing
Key concept - why does the impulse normally die? After propagation, the entire ventricular muscle enters refractoriness simultaneously. The impulse has "nowhere to go" - it extinguishes, and the heart waits for the next SA node beat.
How VF Develops - The Reentry Mechanism
VF arises primarily from reentry circuits (also called circus movements). Three conditions allow an electrical impulse to keep re-circulating instead of dying out:
- Long pathway - dilated cardiomyopathy, hypertrophied hearts - by the time the impulse completes the circuit, tissue ahead is no longer refractory
- Slow conduction velocity - ischemia, Purkinje system block, high K+ - the impulse arrives at tissue that has already recovered
- Shortened refractory period - sympathetic stimulation, drugs (epinephrine, certain anti-arrhythmics) - tissue recovers very quickly, the impulse re-enters too soon
What starts as one reentry circuit degenerates into multiple simultaneous wavefronts - this is the chain reaction mechanism of fibrillation. Once multiple small patches of ventricular muscle are contracting while equally many are relaxing, no net pumping occurs. The ventricles remain in a state of partial contraction - "intermediate" between systole and diastole.
3. Etiology and Risk Factors
Cardiac Causes (most common)
| Category | Examples |
|---|
| Ischemic heart disease | Acute STEMI, NSTEMI, chronic CAD - most common cause |
| Primary cardiomyopathies | Dilated CMP, Hypertrophic CMP (HCM), Arrhythmogenic RV CMP (ARVC) |
| Structural heart disease | Valvular disease (AS), congenital heart disease |
| Channelopathies | Long QT syndrome (congenital/acquired), Brugada syndrome, Short QT syndrome, Catecholaminergic polymorphic VT (CPVT) |
| Conduction system disease | WPW syndrome (especially with AF + rapid ventricular response) |
| Heart failure | Advanced HF with EF <35% |
| Primary electrical VF | Idiopathic VF (no structural cause identified) |
| Commotio cordis | Blunt chest trauma during T-wave upstroke (baseball, hockey puck) |
Non-Cardiac Causes
| Category | Examples |
|---|
| Electrolyte disturbances | Hypokalemia, hypomagnesemia, hypercalcemia, severe hyperkalemia |
| Drugs/toxins | Digoxin toxicity, tricyclic antidepressants, cocaine, organophosphate poisoning, aconitine poisoning |
| Metabolic | Severe acidosis, hypothermia |
| Respiratory | Severe hypoxia (any cause) |
| Procedures | Cardiac catheterization, central line placement (catheter irritation of myocardium) |
| Electrocution | 60-cycle AC current particularly dangerous |
| CNS events | Subarachnoid hemorrhage (can cause severe QT prolongation → VF) |
Clinical pearl (NEET PG high-yield): The most common cause of VF is ischemic heart disease. VF complicates approximately 5-10% of acute MIs. Primary VF (within first 48 hours of MI, without pump failure) has better prognosis than secondary VF (with cardiogenic shock).
4. Pathophysiology - Step by Step
Step 1 - The Trigger:
A premature ventricular contraction (PVC) or external stimulus (ischemia, shock) fires during the vulnerable period of the T-wave (relative refractory period). This is the "R-on-T phenomenon" - if a PVC falls on the T-wave when part of the ventricle is still refractory and part is recovering, it can initiate reentry.
Step 2 - Conditions for Reentry:
Ischemia does three things simultaneously that favor reentry:
- Creates areas of slow conduction (ischemic cells have low resting membrane potential)
- Creates non-uniform refractoriness (some areas recover faster than others)
- Shortens action potential duration in some cells, lengthens in others → dispersion of refractoriness
Step 3 - Spiral Wave Initiation:
A single reentry circuit ("spiral wave" or "rotor") forms. In a structurally normal heart, one rotor may be enough to produce a sustained VF.
Step 4 - Wavefront Multiplication (Chain Reaction):
As per Guyton's description, one reentry circuit degenerates into multiple daughter wavelets. Now 30-50 small patches of ventricular muscle are contracting simultaneously and independently. No coordinated systole occurs.
Step 5 - Loss of Cardiac Output:
Ventricles neither fully contract nor relax - they vibrate. Cardiac output = 0. Coronary perfusion stops. Brain ischemia begins.
Step 6 - Time-Critical Deterioration:
- 0-4 seconds: Awareness lost
- 4-5 seconds: Unconsciousness
- 10-20 seconds: Seizure-like activity (agonal)
- 4-6 minutes: Irreversible brain damage begins
-
10 minutes without CPR: Near-zero survival
Step 7 - Electrical Deterioration:
VF itself worsens over time. Coarse VF (large amplitude) degenerates into fine VF (small amplitude) as myocardial energy stores (ATP) are depleted. Fine VF is harder to defibrillate. This is why CPR buys time - it maintains coronary flow, keeps the VF coarse, and improves defibrillation success.
5. ECG Features of VF with Detailed Interpretation
The ECG of VF (Guyton & Hall):
"The ECG is bizarre and ordinarily shows no tendency toward a regular rhythm of any type."
Classic ECG features:
| Feature | Description |
|---|
| P waves | Absent - no organized atrial activity |
| QRS complexes | Absent - no identifiable QRS |
| T waves | Absent |
| Baseline | Completely irregular, chaotic undulating waves |
| Rate | Indeterminate (appears 300-500/min but no true rate) |
| Rhythm | Completely irregular (no two deflections are alike) |
| Amplitude | Varies (see coarse vs fine below) |
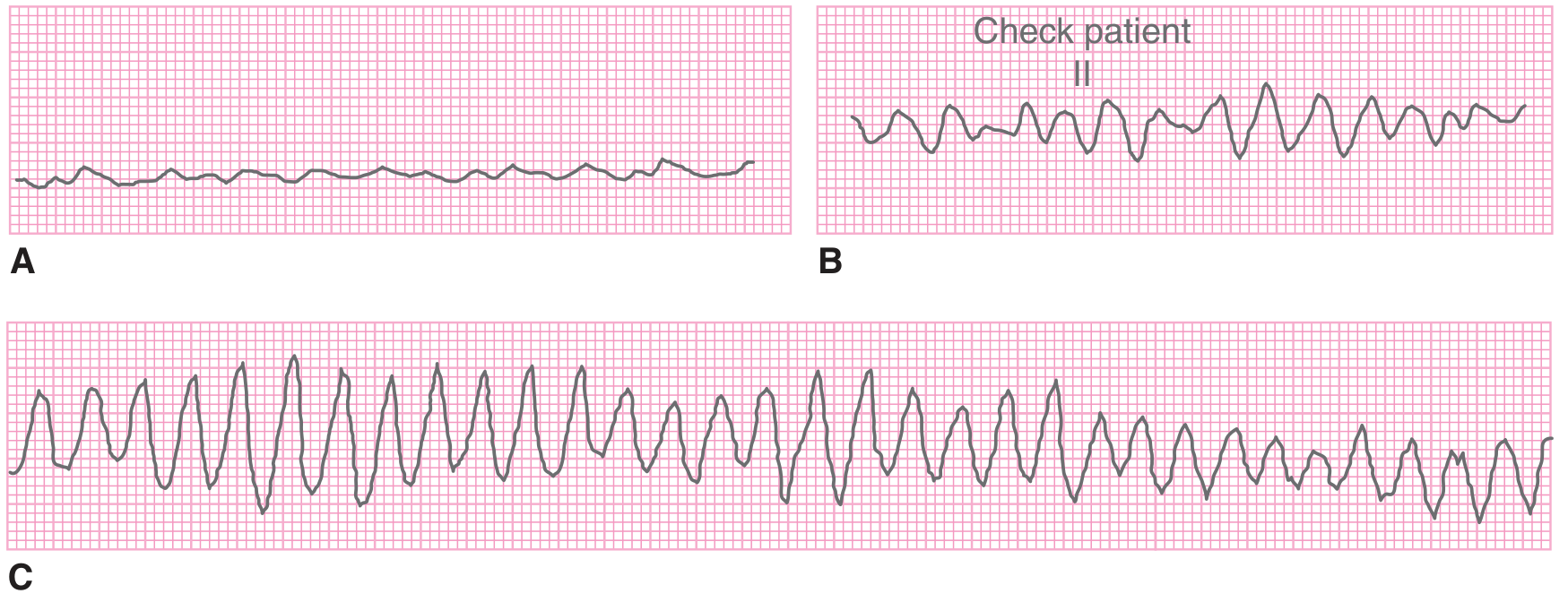
ECG images from Tintinalli's Emergency Medicine:
A = Fine VF (very small amplitude), B = Coarse VF (larger amplitude), C = Coarse VF mimicking polymorphic VT
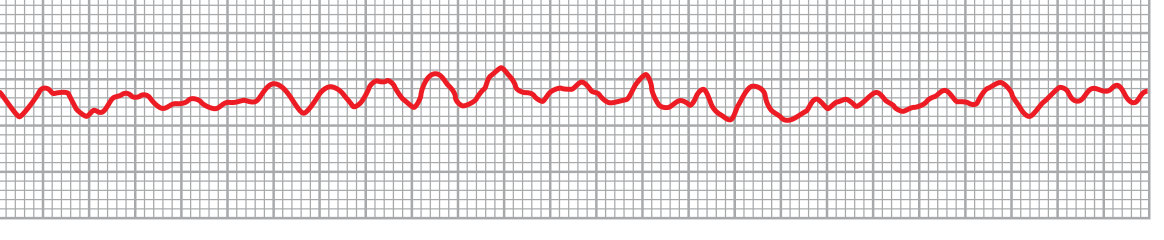
ECG from Guyton & Hall (Lead II):
Classic VF pattern - irregular undulating waveform without any identifiable P-QRS-T
ECG Interpretation Points for Exams:
- No identifiable QRS complex - this single feature is the most important
- No isoelectric baseline - the tracing never returns to a flat line
- Chaotic, random deflections - vary continuously in amplitude, frequency, and morphology
- During first few seconds: larger amplitude waves (coarse VF) as large masses contract
- After 20-30 seconds: amplitude decays to 0.2-0.3 mV
- After depletion: minute voltages of 0.1 mV or less can persist for 10+ minutes
6. Clinical Features and Presentation
VF presents as sudden cardiac arrest (SCA). The sequence is:
Pre-arrest (seconds before - if witnessed):
- Sudden collapse
- Patient may cry out as respiratory muscles contract
- Possible prodrome: chest pain (in ischemia-triggered VF), palpitations, presyncope
Arrest (immediate):
- Unresponsive - no verbal response, no purposeful movement
- Apneic or agonal breathing (gasping - do not mistake this for normal breathing)
- Pulseless - no carotid or femoral pulse
- No heart sounds on auscultation
- Skin: rapidly becomes pale, then cyanotic
Within minutes:
- Fixed and dilated pupils (brain hypoxia)
- Seizure-like movements (agonal)
- Loss of all brainstem reflexes
Exam pearl: On ECG monitor, you see chaotic deflections - but the patient is pulseless. Always confirm with the clinical examination. Never diagnose VF from ECG alone without checking for pulse/response.
7. Types of VF: Coarse vs Fine VF
Coarse VF
- Amplitude: > 0.2 mV (large, prominent undulations)
- Appearance: Large, irregular waves easily visible
- Significance: Occurs earlier in VF, myocardium still has some energy reserves (ATP)
- Prognosis: Better - more amenable to defibrillation
- Clinical implication: More likely to convert with first shock
Fine VF
- Amplitude: < 0.2 mV (small, barely perceptible waves)
- Appearance: Near-flat line with tiny irregular undulations
- Significance: Occurs later - energy-depleted myocardium
- Prognosis: Worse - difficult to defibrillate; can be mistaken for asystole
- Clinical implication: CPR first (to restore some perfusion) before defibrillation attempt
Exam Distinction:
| Coarse VF | Fine VF |
|---|
| Amplitude | >0.2 mV | <0.2 mV |
| Stage | Early | Late |
| ATP stores | Present | Depleted |
| Defibrillation | More effective | Less effective |
| Resembles | VT (sometimes) | Asystole |
Critical point: Fine VF can be mistaken for asystole. If you see what looks like asystole - check in 2 leads before declaring it. Fine VF needs a shock; asystole does NOT get shocked.
8. Diagnosis and Differential Diagnosis
Diagnosis:
- Clinical: Sudden unresponsiveness + pulselessness + apnea
- ECG: Chaotic, irregular undulations without QRS complexes
- Always confirm in two leads before treating
Differential Diagnosis of "No Pulse + Abnormal ECG":
| Condition | ECG | Pulse | Treatment |
|---|
| VF | Chaotic, no QRS | Absent | SHOCK |
| Pulseless VT | Wide, regular QRS | Absent | SHOCK |
| Asystole | Flat line (or fine VF) | Absent | CPR + drugs (NOT shock) |
| PEA | Organized rhythm | Absent | CPR + drugs (NOT shock) |
| Torsades de Pointes | Polymorphic, twisting QRS around baseline | May be present/absent | Mg2+, shock if pulseless |
Shockable rhythms = VF + Pulseless VT (the two rhythms that respond to defibrillation)
Non-shockable rhythms = Asystole + PEA (defibrillation is useless and harmful)
Differential for the ECG pattern of VF:
- Artifact (electrode displacement, patient movement) - can perfectly mimic VF; check the patient!
- Fine VF vs asystole - check in multiple leads; turn up gain
- Coarse VF vs polymorphic VT / Torsades - if patient is pulseless, it does not matter - shock both
9. ACLS Management (Latest Guidelines - AHA 2020/2023 Update)
Fundamental principle: Time = Survival. Every minute of VF without defibrillation = 7-10% decrease in survival odds.
Immediate Steps (First 2 Minutes):
C-A-B (not A-B-C in cardiac arrest):
- Confirm cardiac arrest: unresponsive, no normal breathing, no pulse (check <10 seconds)
- Call for help: activate emergency response, get AED/defibrillator
- Start CPR immediately - do not wait for equipment
- Attach monitor/defibrillator while CPR is ongoing
Defibrillation Energy Levels:
| Defibrillator Type | First Shock | Subsequent Shocks |
|---|
| Biphasic (preferred) | 120-200 J (or per manufacturer) | Escalate or same dose |
| Monophasic | 360 J | 360 J (same) |
| Pediatric | 2 J/kg first shock | 4 J/kg, then max 10 J/kg |
Key point from Morgan & Mikhail: "The first shock is usually associated with ~90% efficacy. Biphasic waveforms achieve same success with less energy and less myocardial injury than monophasic."
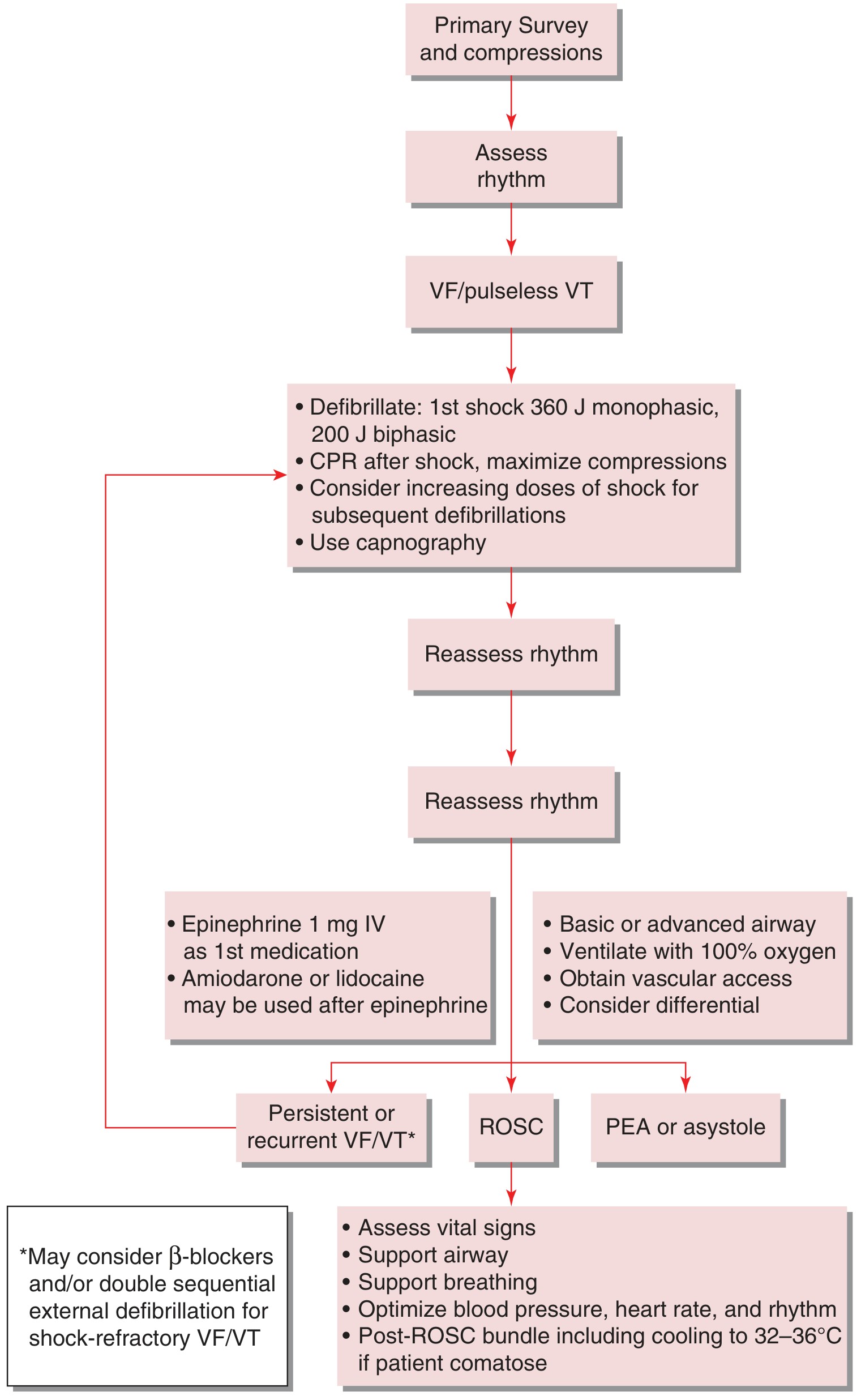
Management Algorithm (Tintinalli's):
CPR Sequence (High-Quality CPR Standards):
| Parameter | Standard |
|---|
| Rate | 100-120 compressions/min |
| Depth | At least 5 cm (2 inches), max 6 cm |
| Recoil | Full chest recoil between compressions |
| Interruptions | Minimize - pre-shock pause <10 seconds |
| Compression:ventilation ratio | 30:2 (before advanced airway); continuous compressions + 10 breaths/min after |
| Hand position | Lower half of sternum |
CPR-Shock-CPR Cycle:
- CPR (2 minutes)
- Stop CPR → check rhythm → if VF/pVT: shock
- Immediately resume CPR for 2 minutes (do not check pulse right after shock)
- After 2 min CPR: check rhythm again
- Give drugs in next cycle
Why CPR before checking pulse after shock? Even a successful shock causes a post-shock pause where myocardium is stunned - it needs CPR support to restore perfusion and allow recovery.
Drug Therapy:
1. Epinephrine (Adrenaline):
- Dose: 1 mg IV/IO every 3-5 minutes
- Route: IV or intraosseous (IO); if no IV access, can give via ETT (2-2.5 mg diluted)
- Timing: Give after 2nd shock (or after 1st shock if no IV yet)
- Mechanism: Alpha-1 agonist → vasoconstriction → increases aortic diastolic pressure → improves coronary perfusion pressure → increases likelihood of ROSC
- Note: Beta effects increase myocardial oxygen demand but also increase contractility
- AHA 2020 update: Epinephrine improves ROSC but long-term neurological survival benefit is less clear; still recommended
2. Amiodarone:
- First-line antiarrhythmic for shock-refractory VF
- Dose: 300 mg IV bolus (first dose), then 150 mg IV (second dose, if needed)
- Mechanism: Prolongs action potential and refractory period (Class III), also has Class I, II, IV effects
- Given: After 3rd shock (when VF persists despite CPR + 3 shocks + epinephrine)
3. Lidocaine:
- Alternative to amiodarone if amiodarone not available or contraindicated
- Dose: 1-1.5 mg/kg IV (first dose), then 0.5-0.75 mg/kg (repeat doses)
- Mechanism: Blocks fast Na+ channels → depresses ectopic pacemakers → Class IB
- Note: Amiodarone is preferred; lidocaine is the backup
4. Magnesium Sulfate:
- Indicated for: Torsades de Pointes + hypomagnesemia-associated VF
- Dose: 1-2 g IV over 5-20 minutes
- Not used routinely in VF
5. Sodium Bicarbonate:
- Not routine in VF
- Indicated in: pre-existing metabolic acidosis, hyperkalemia, TCA overdose
- Dose: 1 mEq/kg IV; risk is paradoxical intracellular acidosis
Drug sequence summary (memory trick: "Every Angry Lion Might Sleep"):
- Epinephrine - every 3-5 min (start after 2nd shock)
- Amiodarone - 300 mg after 3rd shock
- Lidocaine - if amiodarone unavailable
- Magnesium - for TdP/hypomagnesemia
- Sodium bicarbonate - only for specific indications
Post-Resuscitation Care (Post-ROSC Bundle):
Once spontaneous circulation returns (ROSC):
-
Targeted Temperature Management (TTM):
- Indicated for comatose patients after ROSC
- Target temperature: 32-36°C for at least 24 hours
- Prevents secondary neurological injury from reperfusion
- Evidence: TTM at 33°C vs 36°C shows similar outcomes; 36°C is now often preferred (more stable hemodynamics)
-
Hemodynamic stabilization:
- Target MAP >65 mmHg (vasopressors if needed)
- Avoid hypotension (SBP <90 mmHg worsens outcomes)
- Optimize heart rate and rhythm
-
Ventilation:
- Avoid hyperoxia: target SpO2 94-98% (hyperoxia causes reactive oxygen species injury)
- Avoid hypocapnia: target PaCO2 35-45 mmHg
- Normocapnia preferred
-
Identify and treat the cause:
- 12-lead ECG: look for STEMI (requires immediate PCI even if comatose)
- Echo: assess wall motion, structural disease
- Labs: electrolytes, ABG, troponin, toxicology screen
- Consider cardiac catheterization
-
Neuroprognostication:
- Do not declare neurological prognosis within first 72 hours post-ROSC (TTM and sedation confound exam)
- Use multimodal approach: clinical exam + EEG + SSEP + brain imaging
-
ICD implantation:
- Indicated if no reversible cause identified (reduces recurrence risk)
- Consider after 40+ days of surviving MI (EF <35%)
10. Complications and Prognosis
Complications of VF/Resuscitation:
| Complication | Mechanism |
|---|
| Hypoxic-ischemic encephalopathy | Cerebral hypoperfusion during arrest |
| Post-cardiac arrest syndrome | Systemic ischemia-reperfusion injury |
| Myocardial dysfunction | Post-arrest stunning (temporary), amiodarone toxicity |
| Rib fractures / sternal fractures | From CPR (expected) |
| Pneumothorax | CPR, intubation |
| Aspiration pneumonia | Loss of airway reflexes |
| Acute kidney injury | Hypoperfusion during arrest |
| Recurrent VF | Substrate still present |
Prognosis:
- In-hospital VF: survival to discharge approximately 20-35% (better than out-of-hospital)
- Out-of-hospital VF: survival to discharge approximately 5-10% overall; up to 40-50% if witnessed + bystander CPR + rapid defibrillation
- Time dependency (Morgan & Mikhail): survival decreases 7-10% for every minute without defibrillation
- Best prognostic factor: Witnessed arrest + bystander CPR + early defibrillation (the "chain of survival")
- Primary VF (early VF in acute MI without pump failure): better prognosis, cardiac function usually preserved
- Secondary VF (with cardiogenic shock/heart failure): very poor prognosis
11. Shockable Rhythms: VF vs Pulseless VT
Shockable Rhythms (the two you must know):
Ventricular Fibrillation (VF):
- Mechanism: multiple simultaneous reentry circuits
- ECG: chaotic, no QRS
- Cause: ischemia, HCM, channelopathies, electrolyte disorders
- Treatment: unsynchronized shock (defibrillation)
Pulseless Ventricular Tachycardia (pVT):
- Mechanism: single or multiple reentry circuits; faster than VT that retains a pulse
- ECG: wide regular QRS complexes at 150-250/min
- Cause: similar to VF; often ischemia
- Treatment: unsynchronized shock (defibrillation - same as VF)
VF vs Pulseless VT Comparison (Exam Table):
| Feature | VF | Pulseless VT |
|---|
| ECG pattern | Chaotic, no QRS | Wide, regular QRS |
| Rate | Indeterminate | 150-250/min |
| QRS morphology | None | Uniform (monomorphic) or varying (polymorphic) |
| Pulse | Absent | Absent |
| Organized contraction | No | Technically yes, but ineffective |
| Treatment | Defibrillation (unsynchronized) | Defibrillation (unsynchronized) |
| Drug therapy | Same ACLS protocol | Same ACLS protocol |
Why unsynchronized for both? In VF, there is no QRS to synchronize to. In pVT, attempting synchronization risks discharge during a T-wave (relative refractory period), potentially worsening the arrhythmia. Both get an unsynchronized shock.
VT with pulse vs VF:
- VT with pulse: patient may be alert, hypotensive, or in extremis - may try synchronized cardioversion first
- VF: always pulseless - always needs defibrillation
Key differentiator from Torsades de Pointes (TdP):
- TdP: polymorphic VT with QRS amplitude that twists around the baseline ("turning of the points")
- Associated with prolonged QT interval on baseline ECG
- If pulseless TdP: defibrillate (same as VF/pVT)
- If with pulse: magnesium sulfate 1-2 g IV is first-line
12. High-Yield MBBS Viva Questions and Answers
Q1: What is the most common cause of VF?
A: Acute myocardial infarction (ischemic heart disease). VF is the most common cause of sudden cardiac death.
Q2: What is the most important determinant of survival in VF?
A: Time from collapse to defibrillation. Survival decreases 7-10% per minute without defibrillation.
Q3: What is the mechanism of VF?
A: Reentry circuits (circus movements) due to non-uniform refractoriness, slow conduction, and/or increased pathway length. Spiral wave reentry degenerates into multiple circulating wavefronts - the chain reaction of fibrillation.
Q4: How does defibrillation work?
A: A strong high-voltage electrical current simultaneously throws all ventricular muscle into a refractory state. All action potentials stop. After 3-5 seconds of silence, the SA node (or another pacemaker) restarts normal rhythm.
Q5: What is commotio cordis?
A: VF triggered by a blunt non-penetrating blow to the chest directly over the heart during the vulnerable period (upstroke of T-wave). Common in sports (baseball, hockey). Mechanism: stretch-activated ion channels cause premature depolarization.
Q6: What is the difference between cardioversion and defibrillation?
A: Cardioversion is synchronized to the R-wave (to avoid the vulnerable T-wave period) - used for tachyarrhythmias with a pulse. Defibrillation is unsynchronized - used for VF/pVT where there is no QRS to synchronize to (or where synchronization risks T-wave delivery).
Q7: What drug is first-line for shock-refractory VF?
A: Amiodarone 300 mg IV bolus. Lidocaine is the alternative.
Q8: Why is fine VF worse than coarse VF?
A: Fine VF indicates energy-depleted myocardium (ATP stores exhausted). It is harder to defibrillate. CPR temporarily restores coronary flow and converts fine VF to coarse VF, improving defibrillation success.
Q9: What is the energy for first shock with biphasic defibrillator?
A: 120-200 J (device-specific). For monophasic: 360 J.
Q10: What is post-cardiac arrest syndrome?
A: The systemic ischemia-reperfusion injury that follows successful resuscitation, involving brain injury, myocardial dysfunction, systemic inflammatory response, and persistent precipitating pathology. Managed with TTM, hemodynamic support, and targeted oxygen therapy.
Q11: Name 5 reversible causes of cardiac arrest (the H's and T's):
- H's: Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, Hypothermia
- T's: Tension pneumothorax, Tamponade (cardiac), Toxins, Thrombosis (pulmonary/coronary)
Q12: What is Primary vs Secondary VF in the context of MI?
A: Primary VF occurs suddenly within first 48 hours of MI without preceding hemodynamic deterioration - prognosis relatively good. Secondary VF occurs after LV failure/cardiogenic shock - very poor prognosis.
13. High-Yield NEET PG Concepts and Memory Tricks
High-Yield Facts for MCQs:
- VF = shockable rhythm (along with pVT). Asystole and PEA are NOT shockable.
- R-on-T phenomenon → triggers VF (PVC falling on T-wave)
- QT prolongation → predisposes to TdP → degenerates to VF
- Brugada syndrome: Right bundle branch block pattern + coved ST elevation in V1-V3 → VF risk (especially at night/with fever)
- Long QT syndrome: Congenital (KCNQ1/HERG mutations) or acquired (drugs: quinidine, sotalol, haloperidol, TCAs) → TdP → VF
- ICD is the definitive treatment to prevent recurrent VF (not drugs alone)
- Epinephrine in CPR: improves ROSC but not necessarily long-term neurological survival (AHA 2020)
- Amiodarone > Lidocaine for shock-refractory VF (multiple RCTs)
- Hypothermia/TTM post-ROSC: 32-36°C for 24 hours, comatose patients only
- Wolff-Parkinson-White + AF: rapid conduction via accessory pathway → rates >300/min → VF (avoid digoxin, verapamil - they speed up accessory conduction)
Memory Tricks:
Shockable rhythms: "VF and VT - Voltage kills, Voltage heals" (both start with V, both get shocked)
ACLS drug sequence for VF: "Every 3-5 minutes Epinephrine, After 3rd shock Amiodarone"
H's and T's (reversible causes):
"Hypoxia, Hypovolemia, H+, Hypo/K+, Hypothermia"
"Tension PTX, Tamponade, Toxins, Thrombosis"
Coarse vs Fine VF: "Coarse = current can cure; Fine = fading, fix with CPR first"
Energy for defibrillation: "Biphasic = Better (lower energy: 120-200J); Monophasic = More (360J)"
Commotio cordis: "Latin for agitation of the heart - ball hits chest at T-wave = game over"
Brugada mnemonic: "BRUGADA" = Beware (fever), Right BBB, Upsloping ST, GP misses it, Arrests at night, Diagnosed by flecainide challenge, Asian males most commonly
NEET PG Frequently Tested Points:
- Mechanism of VF: reentry (not automaticity)
- ECG of VF: no P, no QRS, no T - just chaos
- First drug in cardiac arrest (VF): epinephrine 1 mg IV every 3-5 min (after 2nd shock)
- Drug for shock-refractory VF: amiodarone 300 mg IV
- Magnesium sulfate is first-line for Torsades de Pointes (not routine VF)
- Post-ROSC TTM target: 32-36°C
- VF within 48h of acute MI with no heart failure = Primary VF = better prognosis
- Defibrillation mechanism: simultaneously makes all cells refractory → allows SA node to resume
14. Clinical Case Scenario with Explanation
Case:
A 58-year-old male with known hypertension and diabetes is admitted to the coronary care unit with crushing chest pain for 2 hours. His ECG shows ST elevation in leads II, III, aVF (inferior STEMI). He is given aspirin, heparin, and shifted for primary PCI. Suddenly, 30 minutes after admission, the monitor shows the following:
[ECG shows bizarre, chaotic, irregular undulations with no identifiable QRS complexes. Rate appears 400-500/min. No P waves. Patient slumps forward unresponsive.]
Nurse calls for help. Physician rushes in.
Step-by-Step Management:
Step 1 - Confirm arrest:
- "Mr. X, can you hear me?" - No response
- Check carotid pulse for <10 seconds - absent
- No normal breathing (agonal gasps noted)
- ECG = VF pattern
- Diagnosis: VF cardiac arrest in setting of acute inferior STEMI
Step 2 - Call and Start CPR:
- Call code blue / activate emergency team
- Begin chest compressions: 100-120/min, depth 5-6 cm, allow full recoil
- Attach defibrillator pads (already on monitor - check position)
Step 3 - First shock:
- Charge defibrillator: 200 J biphasic
- "Clear!" - ensure no one touching patient
- Deliver shock
- Immediately resume CPR for 2 minutes without checking pulse
Step 4 - After 2 minutes:
- Stop CPR for rhythm check (<10 seconds)
- VF persists on monitor
- Deliver 2nd shock (200-360 J biphasic)
- Resume CPR immediately
- Establish IV access, draw labs
- Intubate/advanced airway
Step 5 - Drugs (3rd cycle):
- Epinephrine 1 mg IV - push, followed by 20 mL NS flush
- Continue CPR cycle
- If VF persists after 3rd shock: Amiodarone 300 mg IV bolus
- Epinephrine every 3-5 minutes
Step 6 - ROSC achieved after 4th shock:
- Patient has palpable carotid pulse
- BP: 90/60 mmHg, HR: 70/min in sinus rhythm
- Patient remains comatose
Step 7 - Post-ROSC Care:
- 12-lead ECG: confirms inferior STEMI
- Emergent coronary angiography + PCI (even if comatose)
- Initiate TTM: target 33-36°C for 24 hours
- Mechanical ventilation: SpO2 94-98%, PaCO2 35-45 mmHg
- BP support with vasopressors to maintain MAP >65 mmHg
- ICU admission, continuous monitoring
- Consider ICD if recurrence risk high
What to tell the examiner:
This is a case of primary VF complicating an acute inferior STEMI, managed as per ACLS 2020 guidelines. The primary cause (STEMI) was treated with PCI. Post-ROSC care targeted temperature management and hemodynamic optimization. The prognosis depends on the duration of VF, quality of CPR, and neurological recovery, with ICD implantation to prevent recurrence.
15. Flowchart: Diagnosis and Management of VF
PATIENT COLLAPSES
|
↓
ASSESS: Responsive? Breathing? Pulse?
|
NO to all ↓
|
CALL FOR HELP + START CPR (100-120/min, 5-6 cm depth)
|
↓
ATTACH MONITOR/DEFIBRILLATOR
|
↓
ASSESS RHYTHM
|
┌──┴──┐
SHOCKABLE NON-SHOCKABLE
(VF or pVT) (Asystole/PEA)
| |
↓ ↓
DEFIBRILLATE CONTINUE CPR
Biphasic: 200J + Epinephrine
Monophasic: 360J every 3-5 min
| Treat H's and T's
↓
IMMEDIATELY RESUME CPR (2 min)
|
↓
CHECK RHYTHM (every 2 min)
|
↓
VF PERSISTS?
|
↓
2nd SHOCK + CPR
|
↓
VF PERSISTS?
|
↓
3rd SHOCK + EPINEPHRINE 1mg IV
|
↓
VF PERSISTS?
|
↓
AMIODARONE 300mg IV + continue CPR-Shock cycles
Repeat Epinephrine every 3-5 min
|
↓
ROSC? ──YES──→ POST-ROSC CARE
| - TTM 32-36°C
NO - Target MAP >65
| - 12-lead ECG
↓ - Treat cause
Consider: - ICU admission
- Double sequential
defibrillation (refractory VF)
- Treat reversible causes (H's and T's)
- Sodium bicarbonate if acidosis
The full ACLS management flowchart from Tintinalli's Emergency Medicine:
16. Common Mistakes Students Make in Exam Questions
Mistake 1: Saying "administer shock synchronized" for VF
VF has no QRS complex - synchronization is impossible and irrelevant. Always use unsynchronized (defibrillation) for VF and pulseless VT. Synchronized cardioversion is for rhythms with an organized QRS (e.g., atrial flutter, VT with pulse).
Mistake 2: Checking pulse immediately after each shock
ACLS guidelines state: after each shock, immediately resume CPR for 2 minutes BEFORE checking the rhythm or pulse. Students lose marks writing "check pulse after shock."
Mistake 3: Confusing VF with asystole in management
Asystole and PEA are NOT shockable. Giving a shock to asystole is wrong. Fine VF (small amplitude) can look like asystole - always check in 2 leads.
Mistake 4: Starting amiodarone too early
Amiodarone is given after the 3rd shock (not first or second), once the VF is confirmed as shock-refractory.
Mistake 5: Using magnesium sulfate as first-line for all VF
MgSO4 is first-line only for Torsades de Pointes or suspected hypomagnesemia. For standard VF, amiodarone/lidocaine are the antiarrhythmics.
Mistake 6: Not stating epinephrine dose correctly
Epinephrine in cardiac arrest = 1 mg IV every 3-5 minutes (not 0.1 mg, not 10 mg). The high-dose epinephrine strategy (0.1-0.2 mg/kg) showed no benefit and potential harm in trials.
Mistake 7: Forgetting post-ROSC care in long-answer questions
Post-resuscitation care (TTM, PCI if STEMI, oxygen targets, ICD consideration) is a high-scoring component that many students omit.
Mistake 8: Confusing primary and secondary VF prognosis
Primary VF (early MI, no heart failure) = good prognosis; Secondary VF (cardiogenic shock) = poor prognosis. Not vice versa.
Mistake 9: Writing "rate 400-500/min" for VF in MCQs
VF has no identifiable rate. The correct answer for "rate in VF" = indeterminate (not measurable). Do not assign a rate to VF.
Mistake 10: Forgetting to mention ICD in long answers on VF management
Implantable cardioverter-defibrillator is the definitive secondary prevention after VF in the absence of a reversible cause. Not mentioning this loses easy marks in university exams.
17. University Exam Model Answers
5-Mark Answer: "Define VF and describe its ECG features."
Ventricular fibrillation (VF) is a life-threatening arrhythmia characterized by chaotic, disorganized electrical activation of the ventricular myocardium resulting in absent coordinated ventricular contraction and zero cardiac output. It is the most common cause of sudden cardiac death.
ECG Features:
- No identifiable P waves (absent atrial activity)
- No QRS complexes (absent organized ventricular activation)
- No T waves
- Baseline shows continuously varying, chaotic, irregular undulations
- Rhythm is completely irregular with no pattern
- Amplitude varies: initially 0.5 mV (coarse VF), declining to 0.2-0.3 mV after 20-30 seconds (fine VF), with minute voltages persisting up to 10 minutes
- Coarse VF: larger deflections, early stage, better response to defibrillation
- Fine VF: small deflections, late stage, can mimic asystole
VF is fatal unless terminated within 1-3 minutes by electrical defibrillation.
10-Mark Answer: "Describe the pathophysiology, clinical features, and management of Ventricular Fibrillation."
Definition and Overview:
Ventricular fibrillation is disorganized depolarization and chaotic contraction of small areas of ventricular myocardium resulting in absent mechanical cardiac activity, zero cardiac output, and cardiac arrest. It is fatal without treatment within 1-3 minutes.
Pathophysiology:
The primary mechanism is reentry (circus movement). Under normal conditions, a cardiac impulse propagates through the ventricles, encounters refractory tissue, and extinguishes. VF develops when three conditions favor reentry:
- Prolonged conduction pathway (dilated heart)
- Decreased conduction velocity (ischemia, high K+)
- Shortened refractory period (catecholamines, drugs)
A trigger (R-on-T PVC, ischemia) initiates a single reentry circuit. This degenerates via a chain reaction into multiple simultaneous wavefronts (30-50 patches contracting independently), preventing coordinated contraction.
Clinical Features:
Sudden collapse with:
- Unconsciousness within 4-5 seconds
- Apnea (or agonal gasping)
- Absent pulse and heart sounds
- Fixed dilated pupils (if prolonged)
- Cyanosis
ECG: chaotic irregular deflections, no QRS, no P wave.
Management (ACLS):
- Confirm arrest; call for help; start high-quality CPR (100-120/min, 5-6 cm depth)
- Attach defibrillator; charge to 200 J (biphasic) or 360 J (monophasic)
- Defibrillate; immediately resume CPR for 2 minutes
- Reassess rhythm every 2 minutes; repeat shock if VF persists
- Establish IV/IO access; Epinephrine 1 mg IV every 3-5 minutes (after 2nd shock)
- After 3rd shock: Amiodarone 300 mg IV bolus (or lidocaine 1-1.5 mg/kg)
- Treat reversible causes (H's and T's)
Post-ROSC Care:
- Targeted temperature management (32-36°C, 24 hours, comatose patients)
- Hemodynamic stabilization (MAP >65 mmHg)
- Avoid hyperoxia (SpO2 94-98%) and hypocapnia
- Identify cause (12-lead ECG; PCI if STEMI)
- ICD implantation if no reversible cause
Prognosis:
Survival decreases 7-10% per minute without defibrillation. Out-of-hospital VF survival: ~5-10% overall; up to 40-50% with bystander CPR + rapid defibrillation.
15-Mark Answer: "Write in detail about Ventricular Fibrillation."
1. Definition (1 mark)
Ventricular fibrillation is a life-threatening cardiac arrhythmia characterized by disorganized, chaotic electrical depolarization of the ventricular myocardium with absent coordinated ventricular contraction, zero effective cardiac output, and clinical death unless treated within minutes.
2. Etiology (2 marks)
Cardiac causes:
- Ischemic heart disease (most common - acute MI, chronic CAD)
- Cardiomyopathies (HCM, DCM, ARVC)
- Channelopathies (Long QT syndrome, Brugada syndrome, CPVT)
- WPW syndrome with AF
- Commotio cordis (blunt chest trauma during T-wave upstroke)
Non-cardiac causes:
- Electrolyte disturbances (hypokalemia, hypomagnesemia)
- Drugs (digoxin toxicity, TCAs, cocaine)
- Severe hypoxia, hypothermia
- Electrocution
3. Pathophysiology (3 marks)
The mechanism is reentry (circus movement). Normal cardiac impulses die when they encounter refractory tissue. VF is initiated when ischemia or other triggers create:
- Non-uniform refractoriness (patchy recovery of myocardium)
- Slow conduction zones
- Areas of shortened action potential
A trigger (commonly R-on-T phenomenon - PVC landing on vulnerable T-wave) starts a reentry circuit. Via a chain reaction mechanism described by Guyton, multiple simultaneous small reentry wavefronts develop. Instead of uniform contraction, 30-50 patches contract independently and asynchronously. The ventricles remain in an "intermediate" state - neither in systole nor diastole. Cardiac output falls to zero.
Metabolic consequences progress rapidly:
- Unconsciousness: 4-5 seconds
- Irreversible brain injury: 4-6 minutes
- VF deteriorates from coarse to fine as myocardial ATP is depleted
4. ECG Features (2 marks)
- No P waves, no QRS complexes, no T waves
- Completely irregular, chaotic undulating waveform
- No isoelectric baseline
- Coarse VF: amplitude >0.2 mV, early stage, responds better to defibrillation
- Fine VF: amplitude <0.2 mV, late stage, mimics asystole
- Rate: indeterminate
5. Clinical Features (1 mark)
Sudden collapse with unconsciousness, absent pulse, absent heart sounds, apnea or agonal breathing, cyanosis. If witnessed, may be preceded by chest pain (in ischemic VF), palpitations, or presyncope.
6. Management - ACLS (4 marks)
Immediate:
- Confirm cardiac arrest (<10 seconds)
- Call for help, activate emergency response
- Start high-quality CPR: 100-120/min, 5-6 cm depth, full recoil, minimize interruptions
Defibrillation:
- Biphasic: 120-200 J (or 200 J); Monophasic: 360 J
- Pediatric: 2 J/kg (first), 4 J/kg (subsequent)
- Immediately resume CPR for 2 minutes after each shock
- Reassess rhythm every 2 minutes
Drugs:
- Epinephrine 1 mg IV every 3-5 minutes (after 2nd shock): increases coronary perfusion pressure
- Amiodarone 300 mg IV after 3rd shock (if VF persists): prolongs refractory period
- Lidocaine 1-1.5 mg/kg IV: alternative to amiodarone
- Magnesium sulfate 1-2 g IV: for Torsades de Pointes
- Treat reversible causes: H's and T's
Post-ROSC Care:
- Targeted temperature management (32-36°C, 24 hours)
- Hemodynamic support (MAP >65 mmHg)
- Controlled ventilation (SpO2 94-98%, normocapnia)
- 12-lead ECG; emergent PCI if STEMI
- ICD implantation if no reversible cause
7. Prognosis (1 mark)
Survival decreases 7-10% per minute without defibrillation. Out-of-hospital VF survival ranges from 5-10% overall to 40-50% with rapid bystander CPR and defibrillation. Primary VF (without heart failure) has better prognosis than secondary VF (with cardiogenic shock). Long-term outcomes depend on neurological recovery and underlying cardiac disease.
8. Complications (1 mark)
- Hypoxic-ischemic encephalopathy (most serious)
- Post-cardiac arrest syndrome (ischemia-reperfusion injury)
- Recurrent VF (if underlying cause untreated)
- CPR-related: rib fractures, pneumothorax, aspiration
Quick Reference Summary Card
| Key Point |
|---|
| Definition | Chaotic ventricular depolarization, no cardiac output |
| Mechanism | Reentry circuits → multiple wavefronts |
| Most common cause | Ischemic heart disease (acute MI) |
| ECG | No P/QRS/T; chaotic irregular waveform |
| Treatment | Defibrillation (unsynchronized) + CPR |
| Biphasic energy | 120-200 J |
| Monophasic energy | 360 J |
| First drug | Epinephrine 1 mg IV every 3-5 min |
| Antiarrhythmic | Amiodarone 300 mg IV (after 3rd shock) |
| Post-ROSC temp target | 32-36°C (TTM) |
| Survival loss per minute | 7-10% without defibrillation |
| Shockable rhythms | VF + Pulseless VT |
| Non-shockable rhythms | Asystole + PEA |
| Key difference VF vs TdP | TdP: twisting QRS + prolonged QT; treat with MgSO4 first |
References: Guyton and Hall Textbook of Medical Physiology (11e/14e) | Harrison's Principles of Internal Medicine (22e, 2025) | Tintinalli's Emergency Medicine (9e) | Braunwald's Heart Disease (12e) | Morgan & Mikhail's Clinical Anesthesiology (7e) | AHA ACLS Guidelines 2020