Pain abdomen with hollow sounds in abdomen with massive vomiting, no fever, no nausea.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"small bowel obstruction" diagnosis management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I have comprehensive information. Let me now compile the full clinical answer.
Intestinal Obstruction - Clinical Analysis
The triad of colicky abdominal pain + high-pitched tinkling/hollow bowel sounds + massive vomiting (without fever) is the hallmark presentation of mechanical intestinal obstruction - most likely small bowel obstruction (SBO).
Pathophysiology
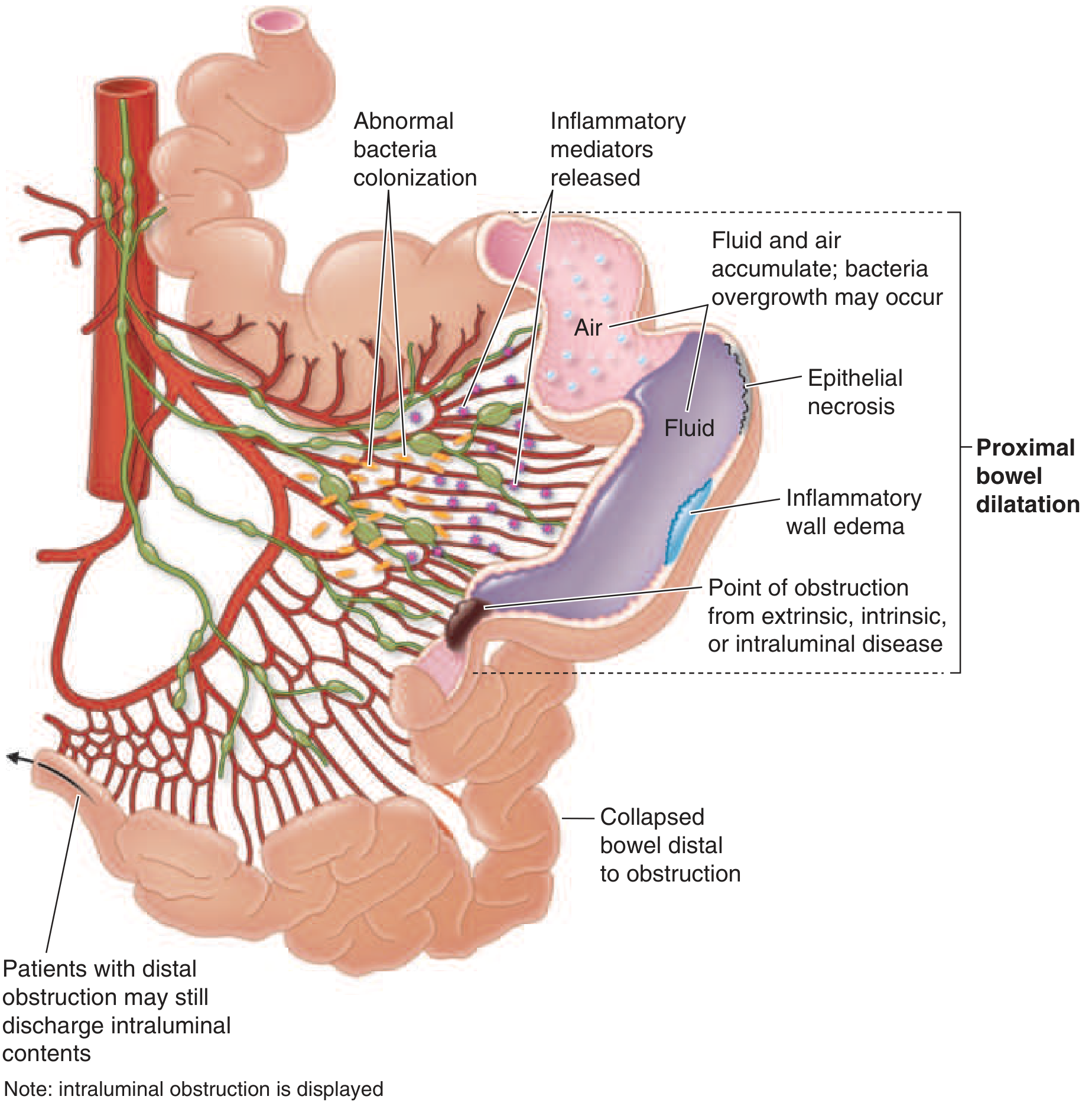
When the small bowel is obstructed, the intestine proximal to the block distends with fluid and gas. The small intestine normally secretes up to 6 litres of salt-rich fluid per day, and this cannot be reabsorbed once obstruction occurs. This leads to:
- Massive fluid accumulation in the bowel lumen
- Progressive distension and increased intraluminal pressure
- Abnormal bacterial colonization and inflammatory mediator release
- Epithelial necrosis and wall edema in severe/prolonged cases
(Harrison's Principles of Internal Medicine 22E, p. 2634; Pye's Surgical Handicraft 22nd Ed.)
Why These Specific Findings?
High-pitched Tinkling / Hollow Bowel Sounds
"A rush of high-pitched tinkling sounds may coincide with an episode of abdominal colic and precede vomiting. Thereafter no sounds may be audible for many minutes."
- Pye's Surgical Handicraft 22nd Ed.
"Many patients with early small-bowel obstruction will have high-pitched, 'musical' tinkling bowel sounds and peristaltic 'rushes' known as borborygmi."
- Harrison's 22E, p. 2635
The gas-liquid interface in a distended, obstructed loop produces these characteristic sounds as peristaltic waves try to overcome the block. This contrasts with ileus (adynamic), where bowel sounds are absent or hypoactive from the outset.
Massive Vomiting Without Nausea
- Proximal SBO (jejunal) causes early, pronounced vomiting with less distension.
- Distal SBO causes late feculent vomiting with more pronounced distension.
- Vomiting is often projectile and forceful - reflecting peristaltic attempts to clear the obstruction.
No Fever
- Absence of fever is characteristic of simple (non-strangulated) obstruction.
- Fever developing later = red flag for strangulation, ischemia, or perforation - a surgical emergency.
Common Causes
| Cause | Key Notes |
|---|---|
| Adhesions (post-surgical) | Most common cause overall (50-70%) |
| Incarcerated hernia | Must always examine hernial orifices |
| Neoplasm | Intrinsic or extrinsic compression |
| Volvulus | Closed-loop obstruction - rapid deterioration |
| Intussusception | More common in children |
| Gallstone ileus | Gas in biliary tree on imaging |
| Crohn's disease | Strictures, inflammatory narrowing |
(Pye's Surgical Handicraft, p. 9003)
Investigations
Bloods
- CBC: Mild leukocytosis is common; marked neutrophilia/left shift = strangulation concern
- U&E: Hypokalemia, hypochloremia (from vomiting); elevated BUN:creatinine = dehydration
- ABG: Metabolic alkalosis from vomiting; metabolic acidosis = ischemia/sepsis alarm
- Serum amylase: May be moderately elevated (especially with strangulation)
- Lactate: Elevated = bowel ischemia
Imaging
| Modality | Findings |
|---|---|
| Erect AXR | "Staircase" pattern - multiple air-fluid levels; dilated small bowel loops >2.5 cm |
| Supine AXR | Valvulae conniventes crossing full width of bowel = small bowel; haustra = colon |
| CT abdomen (IV + oral contrast) | Sensitivity ~95% for high-grade obstruction; identifies transition point, strangulation, closed-loop obstruction |
| Ultrasound | Preferred in pregnancy; shows dilated loops with to-and-fro peristalsis |
"CT is the most frequently used imaging modality. Its sensitivity for detecting bowel obstruction is ~95% (78-100%) in patients with high-grade obstruction, with a specificity of 96%."
- Harrison's 22E, p. 2635
Management
1. Resuscitation First
- IV access, aggressive fluid resuscitation (IV crystalloids - NS or LR)
- Correct electrolyte imbalances (especially potassium)
- Urinary catheter to monitor urine output
2. Nasogastric Tube
- Decompress the stomach - reduces vomiting, aspiration risk, and abdominal pressure
- Insert NGT on free drainage
3. "Drip and Suck" Conservative Trial (for partial/simple SBO)
- IV fluids + NGT decompression
- Serial clinical and imaging reassessment
- Water-soluble contrast (e.g., Gastrografin/meglumine diatrizoate) administered via NGT:
- If contrast reaches the colon within 4-24 hours: very high likelihood of resolution without surgery
- Acts as a therapeutic agent as well (draws fluid into lumen, stimulates motility)
- Supported by recent meta-analyses (PMID: 40341790, BJS Open 2025)
4. Surgical Intervention - Indications
- Emergency surgery for: signs of strangulation (fever, peritonism, tachycardia, metabolic acidosis), closed-loop obstruction, irreversible ischemia, perforation, or failure to improve with conservative management
- Elective/semi-elective for: recurrent SBO, underlying tumor, failed conservative trial
Red Flags Requiring Urgent Surgery
| Sign | Significance |
|---|---|
| Fever (NEW) | Strangulation / peritonitis |
| Constant pain (not colicky) | Ischemia beginning |
| Peritonism / guarding | Perforation or ischemia |
| Metabolic acidosis | Bowel necrosis |
| Rising WBC with immature forms | Sepsis / strangulation |
| Cecum >10-12 cm on imaging | Risk of caecal perforation |
Differentiating from Ileus (Adynamic/Paralytic)
| Feature | Mechanical SBO | Paralytic Ileus |
|---|---|---|
| Pain character | Colicky | Vague, constant or absent |
| Bowel sounds | High-pitched, tinkling | Absent/silent |
| Vomiting | Prominent | Variable |
| Flatus passage | Absent (complete obstruction) | May persist early |
| Cause | Adhesions, hernia, tumor | Post-op, peritonitis, metabolic |
| X-ray | Air-fluid levels, no colonic gas | Diffuse dilatation of all bowel |
The absence of fever in this presentation also helps distinguish simple SBO from mesenteric ischemia (which typically presents with pain out of proportion, often with cardiovascular risk factors).
Key References:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 341, pp. 2634-2636
- Pye's Surgical Handicraft 22nd Ed., pp. 9003-9059
- Water-soluble contrast in SBO: BJS Open 2025 (PMID 40341790)
This is a shared conversation. Sign in to Orris to start your own chat.