A 45 yr old female having fibroid and adenomyosis..she is undergoing a lap. Hysterectomy and oophorectomy ..what is the procedure?
Reading File
Finding Sources
Finding Sources
Searching the Web
laparoscopic hysterectomy oophorectomy procedure steps fibroid adenomyosis
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is the complete breakdown:
Laparoscopic Hysterectomy + Bilateral Oophorectomy: Procedure Overview
Indication in this patient: Uterine fibroids + adenomyosis = definitive surgical management. Since she is 45 years old (peri-menopausal) and bilateral oophorectomy is planned, this will be a Total Laparoscopic Hysterectomy (TLH) + Bilateral Salpingo-Oophorectomy (BSO).
Pre-operative Preparation
- Full history, examination, and imaging (pelvic USG/MRI to map fibroid locations and assess uterine size)
- Bowel preparation is optional in most centers
- DVT prophylaxis (TED stockings, LMWH)
- Consent including risks: bladder/ureteral injury, bowel injury, haemorrhage, vault dehiscence, conversion to open
- Anaesthesia: General with endotracheal intubation (to allow steep Trendelenburg)
Theatre Setup and Patient Positioning
- Dorsal lithotomy position with legs in Allen/Yellowfin stirrups
- Arms tucked at sides (protected with padding) - no shoulder braces (risk of brachial plexus injury)
- Patient placed on beanbag/egg-crate mattress to prevent sliding in steep Trendelenburg
- Examination under anaesthesia (EUA) performed
- Foley catheter inserted to drain bladder
- Uterine manipulator inserted vaginally (e.g., Koh colpotomizer or VCare) - critical for uterine manipulation and colpotomy identification
- Oral/nasogastric tube placed to decompress stomach
Port Placement
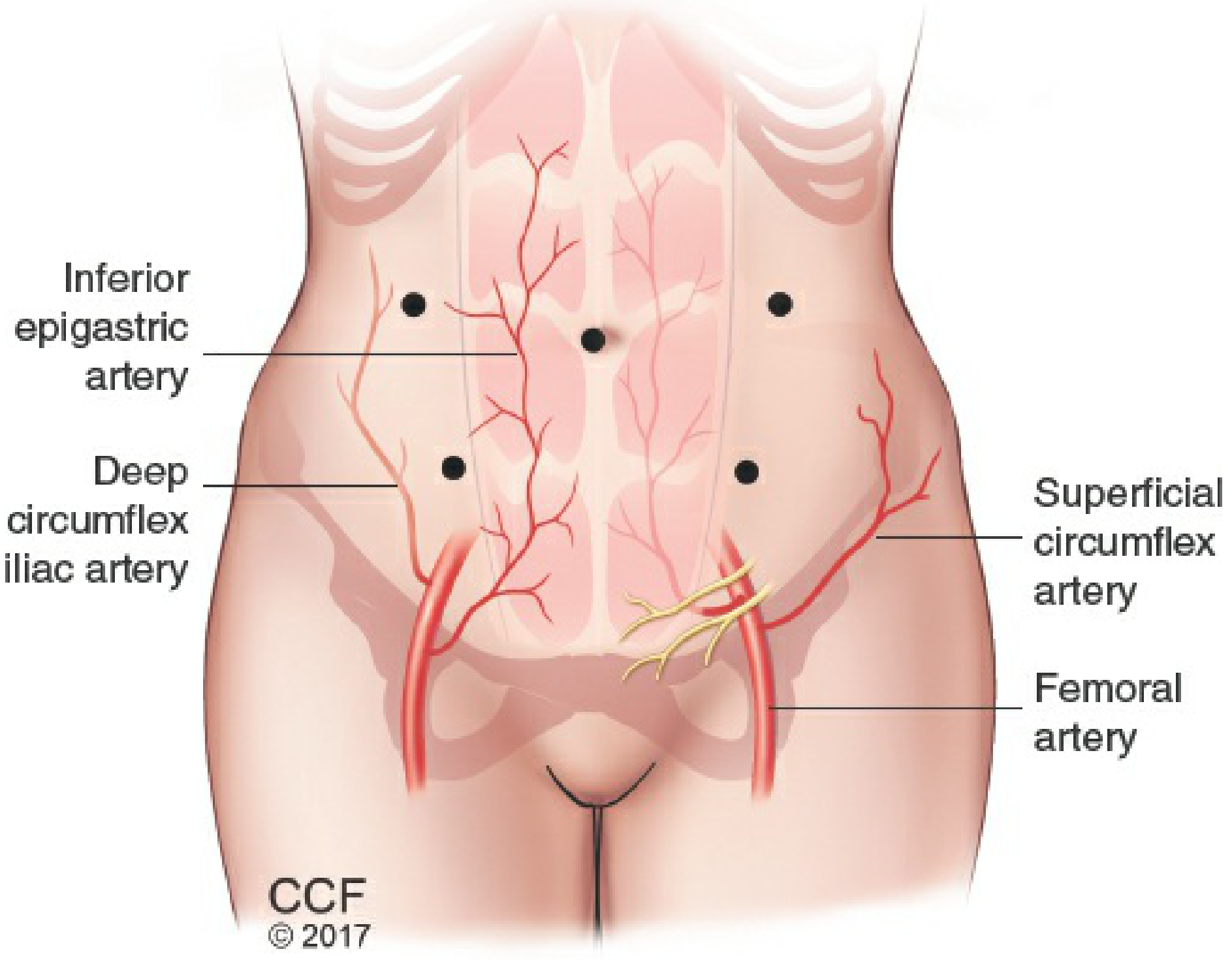
Port placement for laparoscopic hysterectomy - note the lateral ports placed medial to the inferior epigastric vessels (Berek & Novak's Gynecology)
| Port | Size | Location |
|---|---|---|
| Primary (camera) | 10-12 mm | Umbilicus |
| Right lateral | 5-10 mm | ~8 cm from midline, 8 cm above pubic symphysis |
| Left lateral | 5-10 mm | Mirror of right |
| Optional 4th | 5 mm | Additional left lateral for retraction |
- Key: Lateral ports must avoid the inferior epigastric vessels (branch of external iliac a/v); these lie medial to the round ligament insertion at the deep inguinal ring - they cannot be transilluminated and must be visualised directly.
- Patient placed in steep Trendelenburg to displace bowel out of the pelvis.
Surgical Steps (Step-by-Step)
Step 1 - Inspection and Assessment
- Survey the peritoneal cavity for adhesions (prior surgery, endometriosis)
- Assess uterine size, fibroid positions, ovarian/tubal status
Step 2 - Round Ligament Division
- Bilateral round ligaments identified, coagulated (bipolar energy or LigaSure), and divided
- This opens the broad ligament and provides access to the retroperitoneal space
Step 3 - Retroperitoneal Dissection and Ureter Identification
- The retroperitoneal space is opened along the medial leaf of the broad ligament
- The ureter is identified as it crosses the pelvic brim medial to the internal iliac artery - this is the most important safety step to prevent ureteral injury
Step 4 - Adnexal Pedicles (Oophorectomy portion)
- Since oophorectomy is planned: the infundibulopelvic (IP) ligament (containing the ovarian artery and vein) is skeletonised, coagulated, and divided bilaterally
- If only salpingectomy were planned, the utero-ovarian ligament would be divided instead
- The mesosalpinx is also coagulated and divided to free the fallopian tubes with the ovaries
Step 5 - Anterior Dissection / Bladder Flap
- The vesico-uterine peritoneum is incised (the bladder flap)
- Sharp dissection of loose cervicovesical areolar tissue pushes the bladder down off the lower uterine segment and cervix
- This protects the bladder during colpotomy and allows safe vault closure
Step 6 - Uterine Artery Ligation
- The uterus is torqued (anteverted/laterally displaced) away from the side being worked on
- The uterine artery is skeletonised by incising the posterior peritoneum down to the uterosacral ligament
- The uterine artery is then coagulated and transected at the level of the internal os bilaterally
- In fibroid/adenomyosis cases, the uterus is often bulky - adequate uterine manipulation is essential here
Step 7 - Cardinal and Uterosacral Ligaments
- The cardinal ligaments (lateral parametrium) and uterosacral ligaments are coagulated and divided bilaterally
- This fully mobilises the uterus down to the vaginal fornix
Step 8 - Colpotomy (Circumferential Vaginal Incision)
- The colpotomy ring of the uterine manipulator is used to identify and tent the vaginal fornix
- A circumferential incision is made around the cervix using monopolar or harmonic energy
- The uterus (with both ovaries and tubes attached) is now completely free
Step 9 - Specimen Removal
- The specimen is delivered transvaginally
- In cases of large uteruses (fibroids/adenomyosis can make the uterus very bulky - up to 1 kg+), morcellation may be required or the specimen is surgically debulked vaginally (morcellation is now restricted in many centres due to risk of disseminating occult malignancy)
- The vaginal vault is temporarily packed with a moist gauze roll to maintain pneumoperitoneum
Step 10 - Vault Closure
- The vaginal vault is closed either laparoscopically (intracorporeal suturing) or vaginally
- A running locked delayed-absorbable suture (e.g., 0-Vicryl or barbed suture) is used
- The ureters are re-checked after vault closure
Step 11 - Haemostasis Check and Closure
- The pelvis is irrigated and all pedicles inspected for haemostasis
- Port sites are closed: 10 mm or larger port fascial defects are closed with absorbable sutures (Veress or J-needle technique) to prevent port-site hernia
- Skin closed with subcuticular sutures or clips
Key Anatomical Dangers
| Structure at Risk | Step Where at Risk | Prevention |
|---|---|---|
| Ureter | Uterine artery ligation, colpotomy | Retroperitoneal identification before ligation |
| Bladder | Bladder flap, colpotomy | Sharp dissection, fill bladder if uncertain |
| Bowel | Port insertion, adhesiolysis | Proper Trendelenburg, careful dissection |
| Inferior epigastric vessels | Port placement | Direct visualisation, lateral port placement |
| Obturator nerve | Cardinal ligament dissection | Careful dissection within landmarks |
Special Considerations in This Patient
- Fibroids make the uterus bulky - larger manipulator may be needed, morcellation or vaginal debulking likely for specimen extraction; conversion to open must be considered if access to uterine vessels is impossible
- Adenomyosis increases uterine weight and vascularity - higher risk of haemorrhage, longer operative time, and increased difficulty with dissection (PMC evidence)
- Oophorectomy at 45 years induces surgical menopause - counsel patient pre-operatively about vasomotor symptoms, bone loss, and cardiovascular risk; hormone replacement therapy (HRT) discussion is essential
Post-operative Care
- Early mobilisation (same day or next morning)
- VTE prophylaxis continued for 28 days (major pelvic surgery)
- Foley catheter removed at 24 hours
- Pelvic rest for 6-8 weeks (no intercourse/tampons/heavy lifting)
- Warn about vault dehiscence (rare but serious complication of TLH)
Source: Berek & Novak's Gynecology, Chapter 27 - Laparoscopic Hysterectomy, pp. 1453-1458
So in this ptm general anaesthetic is used
Yes, General Anaesthesia (GA) with endotracheal intubation is the standard choice for laparoscopic hysterectomy. Here's why it is mandatory in this case:
Why General Anaesthesia is Used
1. Pneumoperitoneum Requirements
- CO₂ gas is insufflated into the peritoneal cavity to create a working space (pneumoperitoneum)
- Intra-abdominal pressure is raised to 12-15 mmHg
- This elevates the diaphragm, reduces tidal volume, and impairs spontaneous breathing
- Only a ventilated (intubated) patient can be safely managed under these conditions
2. Steep Trendelenburg Position
- The patient is placed in steep Trendelenburg (15-30° head-down)
- This further pushes abdominal contents against the diaphragm
- Leads to decreased lung compliance and functional residual capacity (FRC)
- Spontaneous ventilation is impossible to maintain safely - mechanical ventilation is essential
3. Airway Protection
- The combination of pneumoperitoneum + Trendelenburg significantly increases the risk of gastric regurgitation and aspiration
- Endotracheal intubation with a cuffed ETT protects the airway
4. Duration and Muscle Relaxation
- Laparoscopic hysterectomy + BSO is a long procedure (1.5 - 3+ hours)
- Adequate neuromuscular blockade is needed to:
- Allow proper abdominal wall relaxation for trocar insertion
- Facilitate working space within the abdomen
- Prevent patient movement during critical steps (uterine artery ligation, colpotomy)
5. CO₂ Absorption and Ventilation Control
- CO₂ is continuously absorbed from the peritoneum → causes hypercapnia and respiratory acidosis
- The anaesthetist compensates by increasing minute ventilation (respiratory rate + tidal volume)
- This is only possible with controlled mechanical ventilation
Anaesthetic Technique Summary
| Component | Detail |
|---|---|
| Induction | IV induction - Propofol + Fentanyl |
| Airway | Cuffed Endotracheal Tube (ETT) |
| Muscle relaxant | Rocuronium or Atracurium (reversed with Neostigmine/Sugammadex at end) |
| Maintenance | Inhalational agent (Sevoflurane/Desflurane) or TIVA (Propofol infusion) |
| Ventilation | Controlled mechanical ventilation; ETCO₂ monitored (target 35-40 mmHg) |
| Analgesia | Opioids intra-op + NSAIDs + local anaesthetic port-site infiltration |
| Position | Steep Trendelenburg - requires extra monitoring and padding |
Could Regional Anaesthesia Be Used?
No - not as a sole technique for this surgery. Spinal/epidural anaesthesia is contraindicated as the primary anaesthetic for laparoscopic procedures because:
- It cannot provide diaphragmatic protection
- It cannot manage the respiratory compromise of pneumoperitoneum + Trendelenburg
- It cannot provide adequate muscle relaxation at the abdominal level for prolonged laparoscopy
A combined technique (GA + epidural) is sometimes used in open hysterectomies for post-op pain but is less common for laparoscopic cases since the pain is far less.
Special Monitoring in This Patient
- Capnography (ETCO₂) - mandatory to detect CO₂ retention
- SpO₂ - continuous pulse oximetry
- Arterial line - if large uterus (fibroids/adenomyosis) suggests risk of haemorrhage
- Urinary output via Foley catheter
- Temperature monitoring - long procedures risk hypothermia
This is a shared conversation. Sign in to Orris to start your own chat.