pt 35 female came with complaints of SOB from 3 days and fever consulted private clinic 2 days ago and given paracetamol and monocef but no relief due to persistent of symptoms pt consulted on examination spo2 96 temp 101 RR 28 remaining normal on auscultation I hear cresps sounds on bilateral lungs
"community-acquired pneumonia"[MeSH Terms] AND "treatment failure"[MeSH Terms]
"community-acquired pneumonia"[MeSH Terms] AND "antibiotic treatment"
Clinical Assessment: 35F - SOB + Fever + Bilateral Crepitations
Diagnosis: Community-Acquired Pneumonia (CAP) - Likely Atypical
Severity Assessment (CURB-65)
| Criterion | This Patient | Points |
|---|---|---|
| Confusion | Not mentioned | 0 |
| Urea >7 mmol/L | Unknown | 0 (pending) |
| Respiratory Rate ≥30 | RR 28 - borderline | 0 |
| Blood Pressure ≤90 systolic | Normal | 0 |
| Age ≥65 | 35 years | 0 |
- SpO2 96% (borderline - concerning if it dips further)
- RR 28 (elevated, one point below cutoff)
- Treatment failure with prior antibiotics
- Bilateral lung involvement
Workup to Order
Immediate
- Chest X-ray (bilateral PA view) - look for bilateral infiltrates, consolidation, interstitial pattern
- CBC - leukocytosis/lymphocytosis pattern
- CRP / ESR / Procalcitonin - bacterial vs. viral inflammation marker
- Blood cultures x2 - before starting new antibiotics
- LFT, RFT, electrolytes, blood glucose
- SpO2 monitoring and ABG if SpO2 drops
Specific Atypical Pathogen Workup
- Sputum Gram stain + culture + sensitivity (before antibiotics)
- Mycoplasma pneumoniae serology (IgM/IgG) or PCR
- Urinary Legionella antigen (especially if severe or cluster exposure)
- Urine pneumococcal antigen
- COVID-19 NAAT / RAT - must be ruled out given bilateral involvement
- Influenza A/B rapid antigen (seasonal)
Why Monocef (Ceftriaxone) Failed
Treatment Plan
Step 1: Escalate Antibiotic Coverage
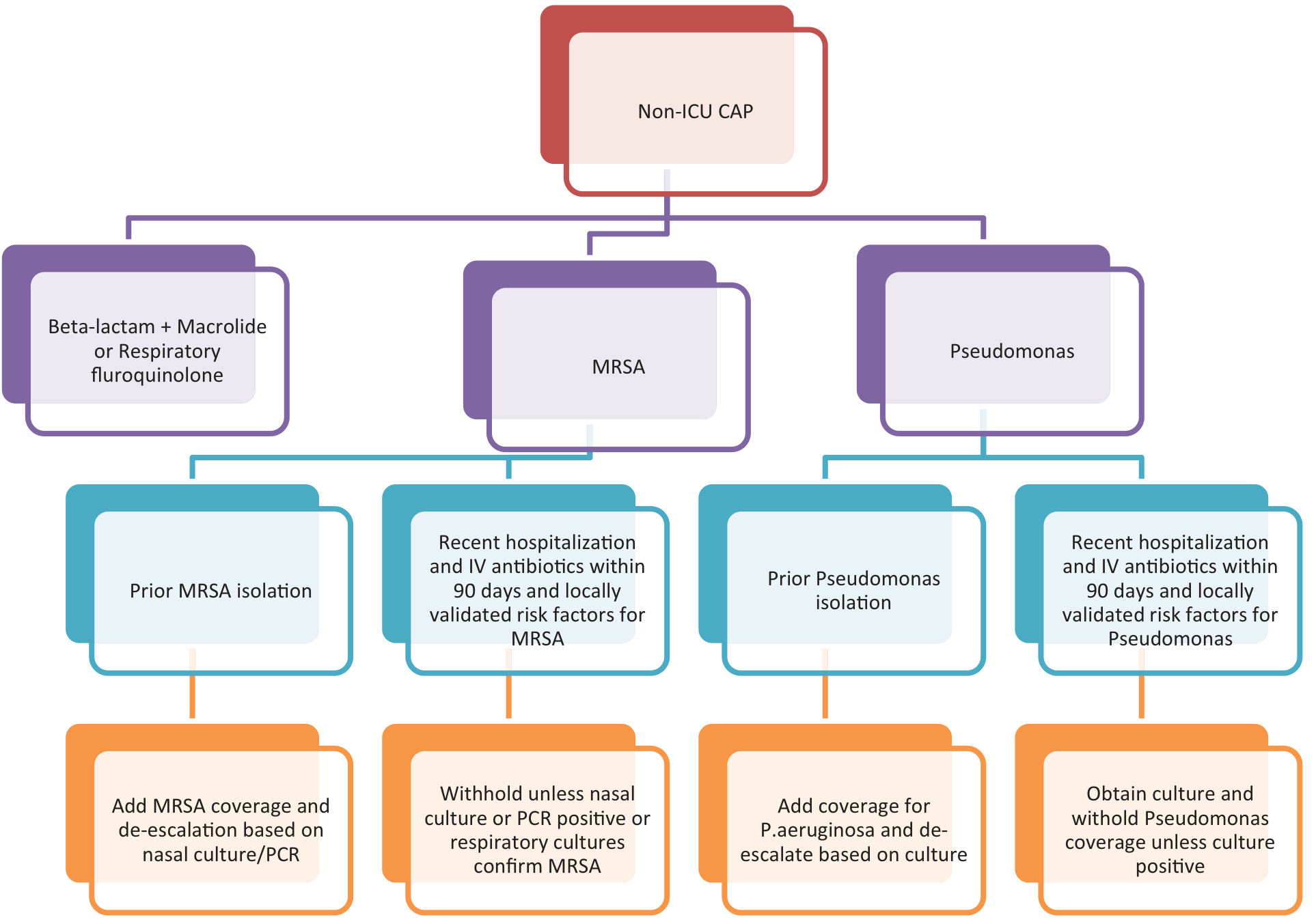
"Either a fluoroquinolone or a beta-lactam/macrolide combination regimen is therapeutically equivalent in non-severe CAP."
- Continue beta-lactam coverage (ceftriaxone 1-2g IV OD or ampicillin-sulbactam 1.5-3g IV q6h)
- ADD azithromycin 500 mg IV/oral OD (macrolide to cover atypicals)
- Levofloxacin 750 mg OD OR Moxifloxacin 400 mg OD
- These cover both typical AND atypical organisms in one drug
Note: If the patient received a macrolide in the past 3 months, prefer fluoroquinolone monotherapy. If she received a fluoroquinolone previously, go with beta-lactam + macrolide. "Antibiotic heterogeneity" reduces resistance pressure. - Fishman's Pulmonary Diseases and Disorders
Antibiotic Treatment Flowchart for Hospitalized Non-ICU CAP:
Step 2: Supportive Care
- O2 supplementation - target SpO2 ≥94% (nasal prongs/mask as needed)
- IV fluids if not tolerating orals
- Antipyretics - paracetamol 650mg q6h PRN (already being used)
- Bronchodilators (nebulization) if wheeze or bronchospasm present
- DVT prophylaxis (LMWH sc) if admitted and immobile
Red Flags to Watch For (Escalate to ICU if)
- RR ≥30 (currently 28 - monitor closely)
- SpO2 dropping below 92% or PaO2/FiO2 ≤250
- Multilobar infiltrates on CXR
- Confusion/disorientation
- BUN ≥20 mg/dL
- Leukopenia (WBC <4000)
- Hypotension requiring vasopressors
Pathogens to Consider by Pattern
| Organism | Clue | Treatment |
|---|---|---|
| Mycoplasma pneumoniae | Young adult, bilateral interstitial pattern, gradual onset, non-response to beta-lactam | Azithromycin or doxycycline |
| Chlamydophila pneumoniae | Similar to Mycoplasma, may have sore throat prodrome | Azithromycin or doxycycline |
| Legionella pneumophila | High fever, GI symptoms, hyponatremia, exposure to water systems | Azithromycin + rifampicin, or levofloxacin |
| S. pneumoniae | Lobar consolidation, rusty sputum, rapid onset | Ceftriaxone (already given, may be partially resistant DRSP) |
| COVID-19 / Viral | Bilateral ground-glass, lymphopenia | Supportive; consider antivirals per current protocols |
Summary Plan
- Admit the patient for inpatient management
- Investigations: CXR, CBC, CRP, procalcitonin, blood cultures, sputum C/S, Mycoplasma serology, urinary Legionella antigen, COVID-19 test
- Switch antibiotics: Add azithromycin 500mg IV OD to existing beta-lactam (or switch to levofloxacin 750mg OD monotherapy)
- O2 support to maintain SpO2 ≥94%
- Monitor RR, SpO2, vitals q4-6h; reassess severity daily
- Duration of therapy: Typically 5 days total for CAP responding to treatment (clinical stability criteria: afebrile, HR <100, RR <24, SpO2 ≥90%, tolerating orals)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Harrison's Principles of Internal Medicine 22E (2025)
- Goldman-Cecil Medicine International Edition
CBC Test Result Interpretation Hemoglobin 7.5 g/dL Severe anemia PCV 25.1% Low RBC Count 4.05 million/cumm Near normal Total WBC Count 19,400/cumm Significant leukocytosis Platelets 4.5 lakh/cumm Upper-normal Differential Count Parameter Result Interpretation Neutrophils 81% High (neutrophilia) Lymphocytes 12% Low (relative lymphopenia) Monocytes 4% Normal Eosinophils 3% Normal Basophils 0% Normal Peripheral Smear RBC morphology: Microcytic Hypochromic Anisocytosis This pattern is strongly suggestive of Iron Deficiency Anemia. WBC morphology: Neutrophilic leukocytosis with lymphopenia Usually seen with: Acute bacterial infection Significant inflammation Stress response CRP Test Result Normal CRP 102.6 mg/L < 6 mg/L Markedly elevated CRP. A CRP above 100 mg/L
CBC + CRP Interpretation & Updated Management
Lab Summary at a Glance
| Parameter | Value | Significance |
|---|---|---|
| Hb | 7.5 g/dL | Severe anemia |
| PCV | 25.1% | Markedly reduced |
| RBC | 4.05 million/cumm | Near normal (disproportionate - see below) |
| WBC | 19,400/cumm | Significant leukocytosis |
| Neutrophils | 81% | Neutrophilia |
| Lymphocytes | 12% | Relative lymphopenia |
| Platelets | 4.5 lakh | Upper-normal (may be reactive) |
| CRP | 102.6 mg/L | Markedly elevated (normal <6) |
| Smear | Microcytic, hypochromic, anisocytosis | Iron deficiency pattern |
Interpretation: Two Concurrent Diagnoses
1. Iron Deficiency Anemia (IDA) - Pre-existing, Severe
"In peripheral smears, red cells are microcytic and hypochromic. Characteristic findings include decreased hematocrit; hypochromic, microcytic red cell indices; low serum ferritin and iron levels; low transferrin saturation; increased total iron-binding capacity."
- Menorrhagia / heavy menstrual bleeding (most common in premenopausal women)
- Poor dietary intake / vegetarian diet
- Chronic GI blood loss (rare at this age but possible - check for H. pylori, celiac)
- Pregnancy (rule out - urine hCG if not done)
2. Acute Bacterial Infection (CAP) - Active, Severe
- WBC 19,400 - significant leukocytosis (normal 4,000-11,000)
- Neutrophils 81% - neutrophilia, hallmark of bacterial infection
- Relative lymphopenia (12%) - typical stress response / acute bacterial infection
- CRP 102.6 mg/L - a CRP >100 mg/L is a strong marker of serious bacterial infection and indicates the infection is not adequately controlled on current treatment
Note: CRP >100 combined with neutrophilic leukocytosis strongly argues against viral/atypical-only etiology and suggests a significant bacterial component - likely S. pneumoniae with possibly an atypical co-infection, or a resistant organism.
Critical Interaction: Anemia + Pneumonia
- Pulse oximetry measures oxygen saturation of hemoglobin - but if there is little hemoglobin to carry O2, tissue oxygen delivery is profoundly reduced even with a normal SpO2
- Oxygen content = Hb × 1.34 × SaO2 - at Hb 7.5, O2 content is roughly half of normal
- This patient's lungs are already compromised (bilateral crepitations, RR 28) - she cannot compensate with increased respiratory effort adequately
- Anemia + pneumonia = compound hypoxia risk - treat both simultaneously
Additional Investigations Needed
| Investigation | Why |
|---|---|
| Serum ferritin | Confirm IDA (will be low); also note: ferritin is an acute-phase reactant - may be falsely normal/elevated during active infection |
| Serum iron + TIBC | Iron low, TIBC high = IDA |
| Peripheral smear review | Already done - confirms IDA |
| Reticulocyte count | Assess bone marrow response |
| Urine hCG | Rule out pregnancy (35F) |
| Menstrual history | Detailed history - duration, flow, clots |
| LFT + RFT | Baseline before antibiotics; also assess anemia of chronic disease |
| Procalcitonin (PCT) | If >0.25 ng/mL confirms bacterial etiology; helps guide antibiotic duration |
| Sputum culture + sensitivity | Identify organism, guide de-escalation |
| Blood culture x2 | Before escalating antibiotics |
Updated Management Plan
A. For Active CAP (Priority - treat first)
- CRP 102.6 (treatment failure, ongoing bacterial infection)
- No response to Monocef (ceftriaxone) alone
- Bilateral disease, RR 28, SpO2 borderline
- Leukocytosis 19,400 with neutrophilia
- Beta-lactam + Macrolide combination:
- Inj. Ceftriaxone 2g IV OD (continue/maintain)
- ADD: Inj. Azithromycin 500mg IV OD (covers Mycoplasma, Legionella, Chlamydophila)
- OR switch entirely to Inj. Levofloxacin 750mg IV OD (monotherapy covering both typical + atypical)
If patient received azithromycin previously or has prolonged QTc on ECG, prefer levofloxacin monotherapy. Check 12-lead ECG before azithromycin (QTc prolongation risk, especially with anemia/electrolyte derangement).
- O2 supplementation - nasal prongs/mask to target SpO2 ≥94-96%
- Antipyretics (paracetamol 650mg q6h PRN)
- IV fluids - assess hydration status
- Monitor vitals q4h; recheck CRP at 48-72h to assess treatment response
B. For Severe IDA (Hb 7.5 g/dL)
- Restrictive threshold: transfuse at Hb <7 g/dL in otherwise stable patients
- This patient has Hb 7.5 g/dL - borderline, but with active pneumonia + tachypnea + reduced O2 carrying capacity, the threshold should be liberalized
- Clinical decision: Transfuse 1-2 units PRBC given respiratory compromise
"A transfusion threshold of a hemoglobin level of 7 g/dL is equivalent to a threshold of 9 to 10 g/dL in terms of the need for life support, or death" - but this is for stable, non-hypoxic patients.
- Oral ferrous sulfate 200mg TDS (take on empty stomach with Vit C for absorption)
- OR IV iron sucrose if oral not tolerated or urgency
- Duration: Continue oral iron for 3-6 months after Hb normalizes (to replete stores)
- Investigate source of blood loss - detailed menstrual history, stool for occult blood, gynecological evaluation
Summary Action List
| Priority | Action |
|---|---|
| Immediate | Add azithromycin IV or switch to levofloxacin IV |
| Immediate | O2 supplementation (titrate to SpO2 ≥95%) |
| Urgent | Consider PRBC transfusion (Hb 7.5 + pneumonia = indication) |
| Today | Serum ferritin, iron, TIBC, reticulocyte count |
| Today | Blood cultures x2 before escalating abx |
| Today | Sputum C/S, urine Legionella antigen, Mycoplasma serology |
| Today | ECG before azithromycin (QTc check) |
| Today | Urine hCG, detailed menstrual history |
| 48-72h | Recheck CRP, WBC - should decline with correct treatment |
| After stabilization | GI evaluation for blood loss if no menstrual cause found |
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Goldman-Cecil Medicine International Edition
- Tintinalli's Emergency Medicine
- Fishman's Pulmonary Diseases and Disorders
see now tell me step by step treatment and management and also pt can't afford all tests
Step-by-Step Treatment & Management
35F | CAP (treatment failure) + Severe IDA | Resource-Limited Setting
STEP 1 - ADMIT THE PATIENT (Day 0, Right Now)
- Treatment failure on antibiotics x2 days
- RR 28 (near threshold), SpO2 96% with bilateral disease
- Hb 7.5 - severe anemia compromising O2 delivery
- CRP 102.6 - uncontrolled infection
STEP 2 - MINIMUM ESSENTIAL TESTS (Affordable, Already Mostly Done)
| Test | Why it matters | Cost |
|---|---|---|
| Chest X-Ray (PA view) | Confirms pneumonia, rules out effusion/empyema, guides severity | Low |
| Random Blood Sugar | Uncontrolled DM worsens pneumonia, affects antibiotic choice | Very low |
| Serum ferritin OR just clinical + smear | If ferritin is unaffordable, the smear already confirms IDA - can treat empirically | Optional |
- Blood culture - skip if unaffordable, start empiric treatment
- Sputum culture - skip if unaffordable
- Legionella antigen, Mycoplasma serology - skip
- ABG - skip unless SpO2 drops below 92%
- LFT/RFT - defer unless signs of organ dysfunction
Clinical diagnosis is sufficient to start treatment. The CBC + CRP + smear + clinical picture give you enough to act.
STEP 3 - ANTIBIOTICS (Most Important Step)
Option A - Preferred (Two cheap drugs, proven regimen):
Inj. Ceftriaxone 2g IV OD [continue or start fresh]
+
Tab. Azithromycin 500mg OD x 5 days
Option B - If you suspect Legionella or want monotherapy (slightly more expensive):
Tab./Inj. Levofloxacin 750mg OD x 5 days
Per Fishman's Pulmonary Diseases: "Either a fluoroquinolone or a beta-lactam/macrolide combination regimen is therapeutically equivalent in non-severe CAP... all patients should receive empiric therapy that provides coverage for atypical pathogens."
Duration:
- Total 5 days of antibiotics if clinical response is good
- Clinical stability = afebrile + RR <24 + SpO2 stable + tolerating orals → switch to oral and plan discharge
STEP 4 - OXYGEN SUPPORT
- Start nasal prongs O2 at 2-4 L/min
- Target SpO2 94-96%
- Do NOT wait for SpO2 to drop - start now given bilateral disease + anemia
- Recheck SpO2 after 30 minutes on O2
STEP 5 - MANAGE THE FEVER AND SYMPTOMS
Tab. Paracetamol 650mg every 6 hours (when temp >38.5°C)
- Already being given - continue this
Nebulization with Salbutamol (Budecort optional) if wheeze or chest tightness
- 2.5mg salbutamol in 2.5mL NS via nebulizer TID
IV fluids: DNS or NS 500mL over 6-8 hours if patient is not eating/drinking
- Maintains hydration, helps with fever
STEP 6 - BLOOD TRANSFUSION DECISION (Critical Step)
- Normally, the transfusion threshold is Hb <7 g/dL
- But with bilateral lung disease and borderline SpO2, her tissues are receiving far less oxygen than normal - her lungs can't compensate for the low Hb
- Decision: Transfuse 1-2 units Packed Red Blood Cells (PRBC)
- Target post-transfusion Hb: 9-10 g/dL
- Give each unit over 3-4 hours with slow rate (she has lung disease - avoid fluid overload)
- If worried about fluid overload, give Inj. Furosemide 20mg IV between units
One unit of PRBC typically raises Hb by ~1 g/dL.
STEP 7 - START IRON SUPPLEMENTATION
Tab. Ferrous Sulfate 325mg (contains ~65mg elemental iron)
- Give ONCE daily on empty stomach in the morning
- OR Tab. Ferrous Ascorbate 100mg BD (better tolerated, better absorption)
"Once-daily administration of ferrous sulfate 325mg on an empty stomach is a typical dosage that maximizes absorption while maintaining high tolerance."
- Take iron with a glass of lemon juice or orange juice (Vitamin C increases absorption by 30%)
- Do NOT take with tea, coffee, milk, or antacids (reduce absorption)
- Stools will turn black - this is normal, not a concern
- Side effects: nausea, constipation - start with OD, can increase to BD after 1 week
STEP 8 - INVESTIGATE THE CAUSE OF ANEMIA (Free - Just Ask)
- How many days is your period? (Normal 3-7 days)
- How many pads per day? (>5 pads/day = heavy)
- Do you pass clots? (Clots = significant blood loss)
- Any recent weight loss, loss of appetite, change in bowel habits? (screen for GI cause)
- Any history of worm infestation? (hookworm = major IDA cause in India)
STEP 9 - DAILY MONITORING (No Cost)
| Parameter | Target |
|---|---|
| Temperature | Should come down within 48-72h |
| RR | Should fall below 24 within 48h |
| SpO2 | Maintain ≥94% on O2, try to wean O2 by day 3 |
| HR | Should normalize as fever settles |
| BP | Monitor - any drop = alarm |
| Urine output | >0.5 mL/kg/hr |
STEP 10 - DISCHARGE CRITERIA & FOLLOW-UP
- Afebrile for 24 hours
- RR <24/min
- SpO2 ≥94% on room air (no supplemental O2)
- Tolerating oral food and medicines
- Hb stable post-transfusion
- Tab. Azithromycin 500mg OD (complete 5-day course if not done)
- Tab. Ferrous Sulfate/Ferrous Ascorbate OD for 3-6 months
- Tab. Paracetamol 650mg SOS for fever
- Follow-up in 1 week - recheck Hb, assess iron response
- Gynaecology referral if menorrhagia confirmed
Quick Reference Summary
DAY 0 (Today):
✅ Admit to ward
✅ CXR + RBS (2 tests only - affordable)
✅ Start Inj. Ceftriaxone 2g IV OD + Tab. Azithromycin 500mg OD
✅ O2 via nasal prongs - target SpO2 94-96%
✅ Arrange 1-2 units PRBC transfusion
✅ Start Tab. Ferrous Sulfate 325mg OD
✅ IV fluids + Paracetamol PRN
DAY 1-2:
✅ Monitor temp, RR, SpO2 q8h
✅ Post-transfusion Hb check
✅ Continue antibiotics
DAY 3-4:
✅ If improving → consider switching to oral antibiotics
✅ Recheck CRP if not improving
DAY 5-7:
✅ If criteria met → discharge with oral antibiotics + iron
✅ 1-week follow-up appointment
- Fishman's Pulmonary Diseases and Disorders
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Goldman-Cecil Medicine International Edition

here is the xray of that pt
Chest X-Ray Analysis
Technical Adequacy
- Projection: PA (Postero-Anterior) - correct
- Rotation: Slight rotation to the left (spinous processes slightly off-center)
- Inspiration: Adequate - 6-7 ribs visible anteriorly
- Exposure: Adequate
Systematic Reading (A-B-C-D-E)
A - Airway
- Trachea is midline - no deviation
- No foreign body
- Carina angle appears normal
B - Bones
- Ribs, clavicles, scapulae - no fractures seen
- Vertebral bodies appear intact
- No lytic/sclerotic lesions
C - Cardiac
- Cardiac silhouette appears normal in size (CTR appears <50%)
- Cardiac borders are well-defined
- No cardiomegaly
D - Diaphragm
- Right hemidiaphragm visible
- Left hemidiaphragm appears slightly obscured by haziness in left lower zone
- Costophrenic angles - right appears sharp; left CP angle shows possible blunting (early/small pleural effusion on left cannot be excluded)
E - Everything Else (Lung Fields)
- Right lower zone: Increased patchy haziness / opacity - consistent with infiltrate or early consolidation
- Right mid zone: Some increased bronchovascular markings
- Right upper zone: Relatively clear
- Left lower zone: Significant haziness / increased opacity - more prominent than the right
- Left mid zone: Patchy opacification - perihilar region shows increased markings
- Left upper zone: Relatively preserved but hazy compared to right upper
- Bilateral lower zone predominant opacities - patchy, heterogeneous
- Pattern is consistent with bilateral bronchopneumonia (patchy, not lobar)
- The left side is more affected than the right
- No clear lobar consolidation - this is a patchy/interstitial-bronchopneumonic pattern
Radiological Impression
Bilateral bronchopneumonia, left > right, with lower zone predominance. Pattern is consistent with atypical/bacterial CAP or mixed infection. Possible early left-sided pleural effusion - left CP angle slightly blunted. No pneumothorax. No cardiomegaly. No frank lobar consolidation.
What This X-Ray Tells Us Clinically
| Finding | Significance |
|---|---|
| Bilateral patchy opacities | Confirms bilateral lung involvement - matches bilateral crepitations on auscultation |
| Lower zone predominance | Typical of CAP (gravity-dependent), aspiration component possible |
| No lobar consolidation | Supports atypical organism (Mycoplasma, Chlamydophila) rather than classic pneumococcal pneumonia which gives lobar consolidation |
| Left > Right | Left lung more affected - important for monitoring |
| Possible left pleural effusion | Small parapneumonic effusion - common with bacterial pneumonia; monitor closely |
| No cardiomegaly | Rules out cardiac pulmonary edema as a cause of bilateral haziness |
Impact on Management - What Changes?
Confirms:
- Admit is absolutely correct - bilateral infiltrates with treatment failure
- Combination antibiotics confirmed - Ceftriaxone + Azithromycin must start NOW
Watch for - Parapneumonic Effusion (Left Side):
- The left CP angle blunting needs monitoring
- If patient worsens or develops pleuritic chest pain - repeat CXR in 48h
- If effusion grows - may need diagnostic tap (but defer unless symptomatic)
Atypical Pattern Confirmed:
- Bilateral patchy infiltrates without lobar consolidation is the classic radiological picture of atypical pneumonia (Mycoplasma, Chlamydophila)
- This explains why Monocef alone failed - the X-ray pattern itself is pointing to atypical organism
- Azithromycin is now even more strongly indicated
CURB-65 Update:
- Multilobar/bilateral involvement is a minor severity criterion per IDSA/ATS
- This pushes towards closer monitoring and ensures ward admission is the right call
Updated Final Drug Chart
IMMEDIATE ORDERS:
1. Inj. Ceftriaxone 2g IV in 100mL NS over 30 min - OD
2. Tab. Azithromycin 500mg orally - OD (with water, 1hr before food)
3. O2 via nasal prongs 2-4 L/min - maintain SpO2 94-96%
4. Tab. Paracetamol 650mg - q6h when temp >38.5°C
5. Inj. DNS 500mL + KCl 20mEq IV over 8h (hydration)
6. Tab. Ferrous Sulfate 325mg OD - morning empty stomach
7. Arrange 1 unit PRBC transfusion (Hb 7.5 + bilateral pneumonia)
MONITORING:
- Temp, RR, SpO2, BP, HR - every 6 hours
- Repeat CXR at 48-72h if no improvement
DURATION:
- Antibiotics: 5 days total
- Review at 72h - if CRP falling + temp settling = on track
pt not willing to admit and asks for daily hospital visit
Patient Refusing Admission - Management Strategy
Step 1: Counsel the Patient First (Don't Skip This)
"Aapko do problems hain - ek lung infection jo abhi bhi control mein nahi hai, aur doosra khoon ki kami. Dono milke bahut dangerous hain. Agar aap ghar jaati hain aur raat ko breathe karna mushkil ho gaya toh emergency mein aana padega - woh zyada expensive aur risky hoga."
- Her SpO2 is borderline - at home if it drops below 90%, it becomes life-threatening
- She has bilateral lung involvement - this is NOT mild pneumonia
- She already failed one antibiotic course - this means the infection is stubborn
- Her blood count (Hb 7.5) means her body has very little reserve to fight
Step 2: Document Informed Refusal (Legally Important)
- Have her sign an LAMA (Leave Against Medical Advice) form
- Document clearly in notes:
- Risks explained verbally
- Patient understood and still refused
- Vitals at time of refusal recorded
- This protects you legally
Step 3: Outpatient "Hospital Visit" Protocol (Daily OPD)
Every Day (Morning Visit - 1 to 1.5 hours):
Day 1-3 (First 3 days - IV treatment at hospital):
-------------------------------------------------
1. Check vitals: Temp, SpO2, RR, BP, HR
→ If SpO2 <92% or RR >30 = ADMIT immediately, no negotiation
2. Inj. Ceftriaxone 1g IV in 100mL NS over 30 minutes - OD
(give in OPD/daycare chair, observe for 30 min after)
3. Nebulization: Salbutamol 2.5mg in 2.5mL NS - once daily at visit
4. Check if she is tolerating oral medications
5. Send home with oral medications (below)
Day 4-5 (Step-down to oral only - if improving):
-------------------------------------------------
If by Day 3:
✅ Temp coming down
✅ RR <24
✅ SpO2 stable ≥94% on room air
→ Stop IV, switch fully to oral antibiotics
→ Continue daily visit just for vitals check
If NOT improving by Day 3 → insist on admission again
Step 4: Oral Medications to Send Home (Take Every Day)
| Medicine | Dose | Timing | Duration |
|---|---|---|---|
| Tab. Azithromycin 500mg | 1 tab OD | Morning, 1hr before food | 5 days |
| Tab. Paracetamol 650mg | 1 tab SOS | Only if temp >38.5°C | As needed |
| Tab. Ferrous Sulfate 325mg | 1 tab OD | Morning empty stomach with lemon water | 3-6 months |
| Tab. Vitamin C 500mg | 1 tab OD | With iron tablet | 3-6 months |
Step 5: Strict Red Flag Instructions - Give in Writing
"Turant hospital aao agar yeh ho:"
- Breathlessness increases suddenly
- Lips or fingers turn blue/dusky
- SpO2 drops (if she has a pulse oximeter at home - tell her to check)
- Cannot speak full sentences due to breathlessness
- Chest pain develops
- Confusion, drowsiness
- No urine for more than 8 hours
- Fever goes above 103°F and doesn't settle with paracetamol
Step 6: The Blood Transfusion Problem
- Many centers can transfuse 1 unit PRBC over 3-4 hours as a day procedure
- She comes in morning, gets transfused, goes home evening
- This is a reasonable compromise
- Frame it to her: "Ek baar 4 ghante baithna hoga, uske baad thakaan aur saans phoolna kaafi kam ho jayega"
Step 7: Day-by-Day Review Checklist
| Day | Expected | Action if Not Improving |
|---|---|---|
| Day 1 | Temp may still be high, SpO2 same | Continue plan |
| Day 2 | Temp starting to settle, feel slightly better | Continue plan |
| Day 3 | RR should be coming down, less breathless | If no change → push for admission |
| Day 5 | Afebrile, SpO2 stable, RR <24 | Switch to oral only, reduce visits |
| Day 7 | Should be significantly better | Repeat CXR if possible |
The Non-Negotiables - Be Firm About These
- Daily visits are NOT optional - if she misses even one day, call her or family
- If SpO2 drops below 92% at any point - she must come to emergency directly
- No improvement by Day 3 = she must admit - put this in writing
- Azithromycin must be taken every single day - stopping early is dangerous
Practical Note

this is the interpretation given by radiology
Radiology Report Analysis & Clinical Correlation
What the Radiologist Said (Verbatim)
- Low lung volume study with mildly elevated right hemidiaphragm
- Mild bibasal linear atelectatic/fibrotic streaks, more prominent in left lower zone
- No focal air-space consolidation
- No pleural effusion or pneumothorax
- Cardiomediastinal silhouette within normal size limits
- Mild bilateral hilar prominence
- No acute bony abnormality
- Multiple external metallic artefacts over chest wall
Low-volume chest with mild bibasal subsegmental atelectatic/fibrotic changes, left > right. Mild bilateral hilar prominence. No focal pneumonic consolidation, pleural effusion, or pneumothorax. Advice clinical correlation.
Honest Assessment: Do You Agree or Disagree?
The radiologist says "No consolidation, No effusion" - is this final?
| Radiology Report Says | Clinical Reality |
|---|---|
| No focal consolidation | True - no lobar pneumonia |
| Bibasal atelectatic/fibrotic streaks | This IS pathological - not normal |
| Mild bilateral hilar prominence | Key finding - suggests infection/inflammation in hilar lymph nodes |
| Low lung volume | Patient couldn't take deep breath - common in sick patients with pain/SOB |
| Advise clinical correlation | Radiologist himself is saying - don't rely on X-ray alone |
What "Bibasal Atelectatic/Fibrotic Streaks + Bilateral Hilar Prominence" Actually Means
1. Bibasal subsegmental atelectasis
- Small airways are collapsing at the bases
- This happens when a patient cannot breathe deeply due to pain, splinting, or infection
- In the context of fever + crepitations + SOB, these are atelectatic changes secondary to pneumonia - not incidental findings
- The infection causes mucus plugging → small airways collapse → crepitations on auscultation
2. Bilateral hilar prominence
- The hila are where major bronchi and pulmonary vessels meet
- Enlarged/prominent hila = reactive lymphadenopathy from active infection
- This is a soft but real radiological sign of active pulmonary infection
- Seen in early/atypical pneumonia, TB (must consider!), sarcoidosis
3. Low lung volume + elevated right hemidiaphragm
- Patient was in pain or too breathless to inspire properly
- A poor-inspiration film compresses lung markings, making infiltrates look worse OR can hide them
- The radiologist himself labels this "low volume study" - this means the film is suboptimal and may be underreporting lung pathology
Critical Point: This X-Ray Does NOT Rule Out Pneumonia
In atypical pneumonia (Mycoplasma, Chlamydophila), the inflammation is interstitial - it involves the walls between air sacs rather than filling the air sacs with fluid. This produces:
- No lobar consolidation
- Only subtle streaky infiltrates
- Bilateral hilar enlargement
- Normal or near-normal X-ray in early stages
Putting It All Together
| Evidence | Points To |
|---|---|
| Fever 3 days, SOB, RR 28 | Active pulmonary infection |
| Bilateral crepitations on auscultation | Alveolar/small airway disease |
| WBC 19,400 + Neutrophils 81% | Significant bacterial infection |
| CRP 102.6 mg/L | Active, uncontrolled inflammation |
| Failed ceftriaxone (beta-lactam) | Atypical organism |
| X-ray: bibasal streaks + hilar prominence | Consistent with atypical/early CAP |
| X-ray: no lobar consolidation | Confirms atypical pattern, not typical pneumococcal |
| Radiologist: "advise clinical correlation" | Radiologist agrees X-ray alone is insufficient |
Does This Change Management?
✅ Inj. Ceftriaxone 2g IV OD - continue
✅ Tab. Azithromycin 500mg OD - mandatory (atypical coverage)
✅ O2 support - continue
✅ Ferrous Sulfate OD - continue
✅ PRBC transfusion - still indicated (Hb 7.5 + respiratory compromise)
One Additional Consideration - Rule Out TB
- Sputum for AFB smear x3 (early morning) - very cheap, widely available
- Ask about: cough >2 weeks, evening rise of temperature, night sweats, weight loss, TB contact history
- If any suspicion → Sputum CBNAAT (GeneXpert) is the gold standard
Summary for You (The Treating Physician)
The radiology report is NOT alarming but is also NOT normal. The bibasal atelectasis, hilar prominence, and low-volume film in the context of your clinical findings (bilateral creps, CRP 102, WBC 19,400, failed beta-lactam) all point to atypical CAP. The radiologist himself asks for clinical correlation - and your clinical picture is clear.Trust your stethoscope and labs over a suboptimal X-ray. Treat accordingly. Screen for TB given hilar prominence. Keep the patient on the daily visit protocol and reassess at 72 hours.
pt complaints of severe cough also
Managing Severe Cough in This Patient
First: Characterize the Cough (Ask These Questions)
| Question | Significance |
|---|---|
| Dry (no sputum) or productive (with sputum)? | Dry = suppress; Productive = help expectorate, never suppress |
| Color of sputum? | Yellow/green = bacterial; Rusty = pneumococcal; Blood-streaked = TB/severe infection |
| Worse at night? | Atypical pneumonia (Mycoplasma) causes paroxysmal nocturnal cough |
| Any wheeze with cough? | Bronchospasm component - needs bronchodilator |
| Cough since how long? | >2-3 weeks raises TB suspicion strongly |
Important Rule: DO NOT Suppress a Productive Cough
- Retain secretions in the airways
- Worsen atelectasis (already present on X-ray)
- Risk developing pneumonia complications
- Completely dry and non-productive
- Causing vomiting or sleep deprivation
- Causing rib pain / exhaustion
Prescription for Cough Based on Type
If PRODUCTIVE cough (most likely in this case):
1. Tab./Syrup Ambroxol 30mg TDS
- Mucolytic - thins out thick secretions, makes them easier to cough out
- Very safe, very affordable
- Take after food
2. Nebulization: Salbutamol 2.5mg + Ipratropium 500mcg in 2.5mL NS
- TID (three times a day) during hospital visit + once at home if nebulizer available
- Opens up airways, reduces bronchospasm, helps clear secretions
- Even without wheeze - helps in atypical pneumonia cough
3. Steam inhalation at home
- Boil water, add 1-2 drops Eucalyptus oil (Karvol/Vicks)
- Inhale steam under towel for 10 minutes - BD
- Loosens mucus, very effective, zero cost
If DRY cough (no sputum at all):
Tab. Levocloperastine 50mg or
Syrup Benadryl/Honitus 10mL TDS - after food
(mild central antitussive - reduces cough reflex)
The Severe Cough + Atypical Pneumonia Connection
- Attaches to respiratory epithelium and causes intense airway irritation
- Produces a cough that can last weeks even after antibiotics start
- Cough is often the last symptom to resolve
- X-ray often looks near-normal despite severe symptoms - exactly what we are seeing here
Also Add: Throat Soothing Measures
- Warm saline gargles: ½ tsp salt in warm water - 3-4 times daily
- Honey + ginger + warm water (home remedy - proven to reduce cough frequency)
- Keep room humid - dry air worsens cough
- Avoid cold water, cold drinks, ice cream completely
- Sleep with head slightly elevated (30°) - reduces post-nasal drip cough
Complete Updated Prescription (All Medicines Together)
DAILY HOSPITAL VISIT (IV/Nebulization):
----------------------------------------
1. Inj. Ceftriaxone 2g IV OD
2. Nebulization: Salbutamol 2.5mg + Ipratropium 500mcg TID
ORAL MEDICINES TO TAKE AT HOME:
---------------------------------
1. Tab. Azithromycin 500mg - OD, morning, 1hr before food (5 days)
2. Tab. Ambroxol 30mg - TDS, after food (7 days)
3. Tab. Paracetamol 650mg - SOS for fever >38.5°C
4. Tab. Ferrous Sulfate 325mg - OD, morning empty stomach (3-6 months)
5. Tab. Vitamin C 500mg - OD with iron tablet
HOME REMEDIES (Free):
----------------------
- Steam inhalation BD
- Warm saline gargles TID
- Honey + ginger in warm water at night
- Head elevated while sleeping
- No cold food/drinks
AVOID:
-------
❌ Cough suppressants (codeine, dextromethorphan) - she has productive cough
❌ NSAIDs (ibuprofen) - may mask fever
❌ Cold water, cold drinks
❌ Lying flat
What to Tell the Patient
"Yeh khansi infection ki wajah se hai - jab tak antibiotic kaam karna shuru karega (2-3 din), tab tak khansi rahegi. Ghabrana mat. Ambroxol tablet aur nebulization se balgam naram padega aur nikalna asaan hoga. Khansi rokne ki dawai mat lo - woh nuksaan degi."
Red Flag: When Severe Cough Means Something Worse
- Blood-streaked sputum (haemoptysis) → TB / fungal infection - send sputum AFB immediately
- Rusty brown sputum → Classic pneumococcal pneumonia - ensure adequate beta-lactam coverage
- Foul smelling thick sputum → Lung abscess / aspiration - need anaerobic coverage added
- Cough >3 weeks → Must rule out TB before continuing treatment
I am saying about this pt only she is having productive cough with yellowish phelm