Opioids
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive morphine monograph. Let me compile the full answer.
Morphine - Complete Drug Profile
1. Source & Classification
Morphine is the principal alkaloid of opium, derived from the poppy Papaver somniferum. It is present at ~10% concentration in crude opium. The term opiate specifically refers to naturally occurring alkaloids like morphine, codeine, thebaine, and papaverine, while opioid describes all compounds acting at opioid receptors. Morphine is chemically a phenanthrene derivative with five fused rings.
- Katzung's Basic and Clinical Pharmacology, 16e
2. Mechanism of Action
Opioid Receptor Types
| Receptor | Functions | Preferred Endogenous Ligands |
|---|---|---|
| μ (mu) | Supraspinal & spinal analgesia, sedation, respiratory depression, slowed GI transit, hormone modulation | Endorphins > enkephalins > dynorphins |
| δ (delta) | Supraspinal & spinal analgesia, hormone modulation | Enkephalins > endorphins & dynorphins |
| κ (kappa) | Analgesia, psychotomimetic effects, slowed GI transit | Dynorphins |
Morphine is a full agonist at the μ-opioid receptor - the primary analgesic receptor. It also has some activity at δ and κ receptors.
Sites of action along the pain pathway:
- Peripheral - acts on inflamed/damaged peripheral tissues
- Spinal cord - inhibits dorsal horn pain transmission neurons AND inhibits release of excitatory transmitters (e.g. substance P) from primary afferents
- Supraspinal - acts in the periaqueductal gray, amygdala, thalamus, and anterior cingulate gyrus
The μ receptor is associated with TRPV1 and substance P-expressing nociceptors. Morphine is unique in that it reduces both the sensory and affective (emotional) components of pain - unlike NSAIDs which only affect the sensory component.
- Katzung's Basic and Clinical Pharmacology, 16e
Structure-Activity Relationships
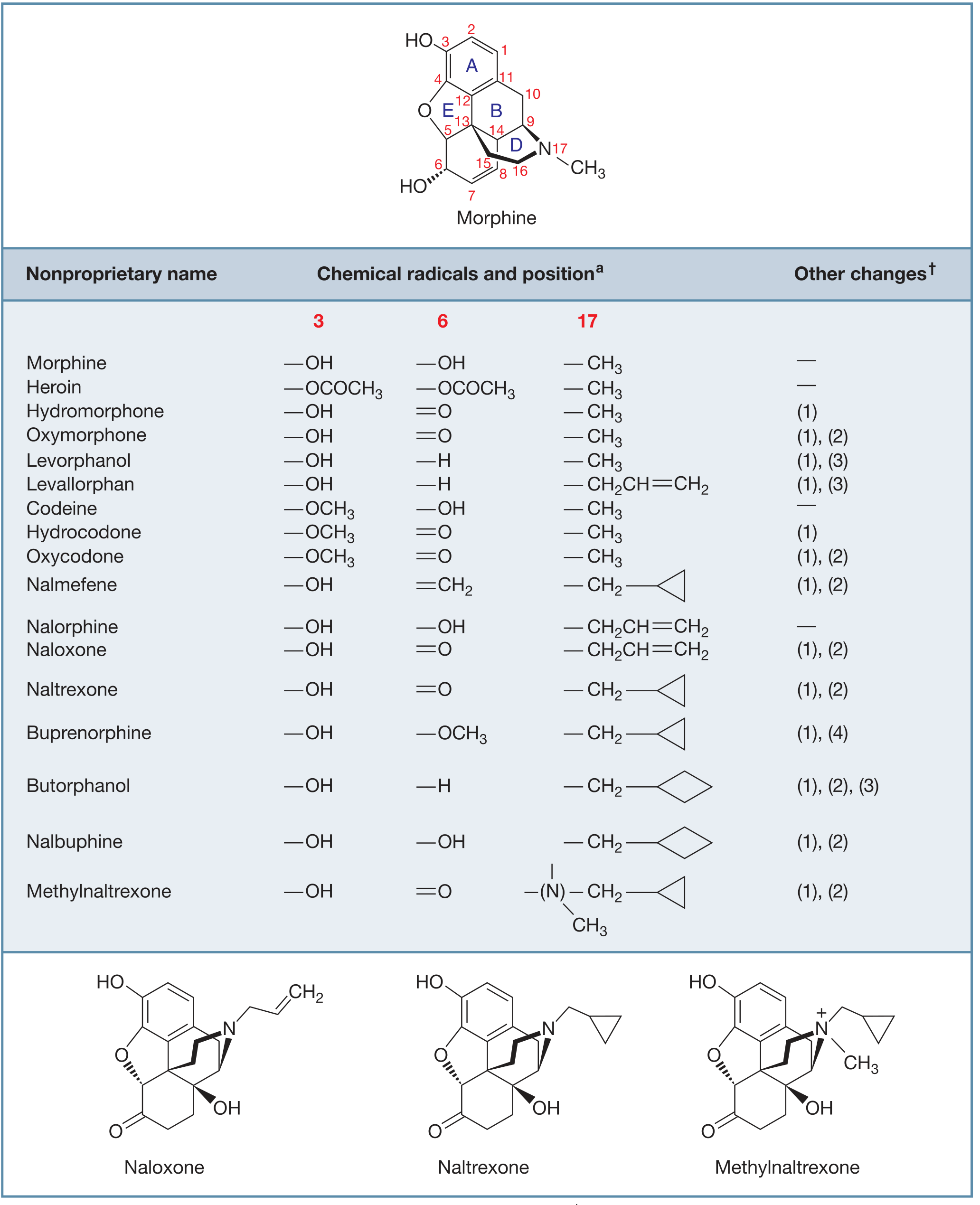
Key modifications from morphine that generate related drugs:
- Heroin (diacetylmorphine): -OCOCH₃ at positions 3 & 6 → faster CNS penetration
- Codeine: -OCH₃ at position 3 → protects 3-OH, better oral bioavailability, must be converted to morphine by CYP2D6 to be active
- Naloxone: allyl group on N + additional -OH → strong μ-receptor antagonist
- Hydromorphone: =O at position 6 → potent semisynthetic agonist
3. Pharmacokinetics
| Parameter | Details |
|---|---|
| Oral bioavailability | ~25% (significant first-pass hepatic glucuronidation) |
| Protein binding | ~1/3 in plasma |
| t½ (morphine) | ~2-3 hours |
| BBB penetration | Low relative to fentanyl, heroin, and methadone |
| Primary metabolism | Glucuronidation to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G) |
| Excretion | Renal (primarily as M3G); 90% excreted within 24 hours |
Metabolite pharmacology:
- M6G (morphine-6-glucuronide): Pharmacologically active, ~2× more potent than morphine; accounts for a significant portion of analgesia. Excreted renally - accumulates in renal failure, prolonging and intensifying effects.
- M3G (morphine-3-glucuronide): Very low opioid receptor affinity; may contribute to excitatory/neuroexcitatory effects of morphine.
- A minor pathway: N-demethylation to normorphine.
Route comparison: IV acts promptly. SC/IM have variable absorption. Oral is slow and erratic. Extended-release oral preparations give more consistent plasma levels. Morphine is also effective via epidural/intrathecal routes due to adequate transdural movement.
Special populations:
-
Renal failure: M6G accumulates - reduce dose/frequency
-
Elderly: smaller volume of distribution + declining renal function - use lower doses
-
Liver disease: pharmacokinetics relatively preserved due to compensatory extrahepatic metabolism
-
Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews Pharmacology
4. Pharmacological Effects (Organ System by System)
CNS
- Analgesia - both sensory and affective pain components
- Euphoria - floating sensation, lessened anxiety (IV administration); dysphoria can also occur
- Sedation - drowsiness, clouding of mentation; disrupts normal REM and non-REM sleep patterns
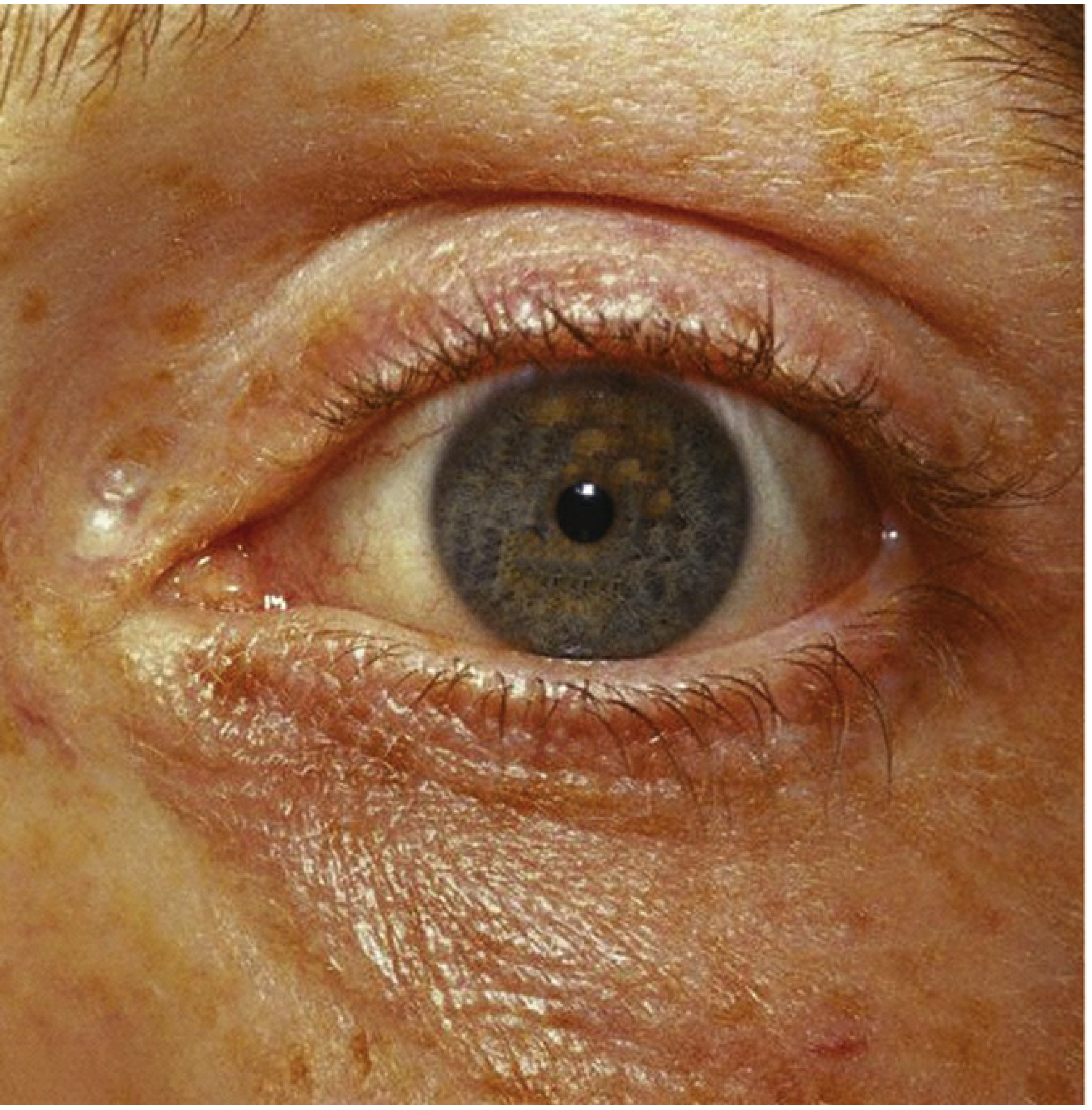
- Miosis (pinpoint pupils) - parasympathetically mediated; minimal tolerance develops, making it a key diagnostic sign in overdose
- Truncal rigidity - at high doses, increased tone in large trunk muscles, reduces thoracic compliance (particularly relevant with IV high-dose use in anesthesia)
- Nausea/vomiting - direct stimulation of the chemoreceptor trigger zone (CTZ) in the area postrema
Respiratory
- Respiratory depression - dose-related, inhibits brainstem respiratory centers; elevates PaCO₂; depresses response to CO₂ challenge
- Cough suppression - useful clinically (codeine); but may allow secretion accumulation
- Contraindicated or use with great caution in: asthma, COPD, cor pulmonale, increased intracranial pressure
Cardiovascular
- Minimal effects at therapeutic doses
- Hypotension and bradycardia at higher doses
- Cerebral vasodilation secondary to CO₂ retention → increased intracranial pressure - contraindicated in head trauma
- Histamine release → vasodilation, urticaria, bronchoconstriction
Gastrointestinal
- Constipation - decreased motility, increased circular smooth muscle tone, increased anal sphincter tone; no tolerance develops to this effect
- Increased biliary tract pressure (contraction of gallbladder, constriction of biliary sphincter)
- Useful for diarrhea (decreases GI motility)
Genitourinary
- Inhibits urinary bladder voiding reflex + increases sphincter tone → urinary retention; may require catheterization
Skin
- Histamine release from mast cells → urticaria, sweating, flushing, pruritus
- Pruritus also occurs centrally (especially with neuraxial administration; incidence 70-100%)
Hormonal
- Prolonged use → opioid-induced androgen deficiency (OPIAD) via suppression of hypothalamic-pituitary-gonadal axis → decreased testosterone → decreased libido, fatigue, depression, osteoporosis
Immune
- Inhibits natural killer cell activity, lymphocyte proliferation - may influence tumor progression
- Modulates lymphocyte function and antibody production
Labour
-
May prolong the second stage of labour by transiently decreasing strength, duration, and frequency of uterine contractions
-
Katzung's Basic and Clinical Pharmacology, 16e; Lippincott Illustrated Reviews Pharmacology
5. Tolerance & Dependence
Tolerance develops to most effects with repeated use, including:
- Analgesia, euphoria, respiratory depression, sedation, nausea
No tolerance (or minimal) develops to:
- Miosis
- Constipation
Physical dependence develops with sustained use. Abrupt discontinuation causes a withdrawal syndrome: anxiety, restlessness, lacrimation, rhinorrhea, yawning, piloerection ("gooseflesh"), diaphoresis, muscle aches, diarrhea, insomnia, tachycardia, and hypertension. Symptoms peak at ~36-72 hours and resolve over ~7-10 days with morphine.
6. Clinical Uses
- Severe acute pain - post-operative, trauma, MI (morphine is part of acute coronary syndrome management to reduce preload/anxiety)
- Cancer pain - particularly moderate-to-severe; oral extended-release formulations used for sustained relief
- Acute pulmonary edema - reduces preload, anxiety, sympathetic drive
- Dyspnea in palliative care
- Premedication for anesthesia
- Neuraxial analgesia - epidural/intrathecal for postoperative, obstetric, and cancer pain
Routes available: oral (IR and ER), IV, SC, IM, epidural, intrathecal, rectal
7. Overdose Triad
The classic opioid toxidrome (useful clinically):
- Pinpoint pupils (miosis) - pathognomonic
- Respiratory depression / apnea
- CNS depression / coma
Treatment: Naloxone (IV/IM/intranasal) - competitive μ-receptor antagonist. Acts within 1-2 minutes IV but has a shorter duration than morphine, so repeat dosing or a continuous infusion may be required.
8. Key Contraindications & Cautions
| Situation | Reason |
|---|---|
| Head trauma / raised ICP | CO₂ retention → cerebral vasodilation → worsening ICP |
| Asthma | Histamine release → bronchoconstriction |
| COPD / cor pulmonale | Respiratory depression can be fatal |
| Renal failure | M6G accumulation → prolonged respiratory depression |
| Labour | May depress neonatal respiration |
| Concurrent CNS depressants | Additive sedation and respiratory depression |
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics | Katzung's Basic and Clinical Pharmacology, 16e | Lippincott Illustrated Reviews: Pharmacology | Miller's Anesthesia, 10e
This is a shared conversation. Sign in to Orris to start your own chat.