Horners syndrome
Reading File
Finding Sources
Searching PubMed
"Horner syndrome" diagnosis management
Reading File
Reading File
Searching Images
Horner syndrome ptosis miosis anhydrosis eye
Reading File
Loading Image
Loading Image
Reading File
Searching Images
sympathetic pathway three neuron Horner syndrome diagram anatomy
Loading Image
I have all the information needed. Here is a comprehensive overview of Horner syndrome.
Horner Syndrome (Oculosympathetic Palsy)
Definition
Horner syndrome results from disruption of the sympathetic innervation to the eye and face at any point along its three-neuron pathway. The full name is Bernard-Horner syndrome; it is also called oculosympathetic palsy.
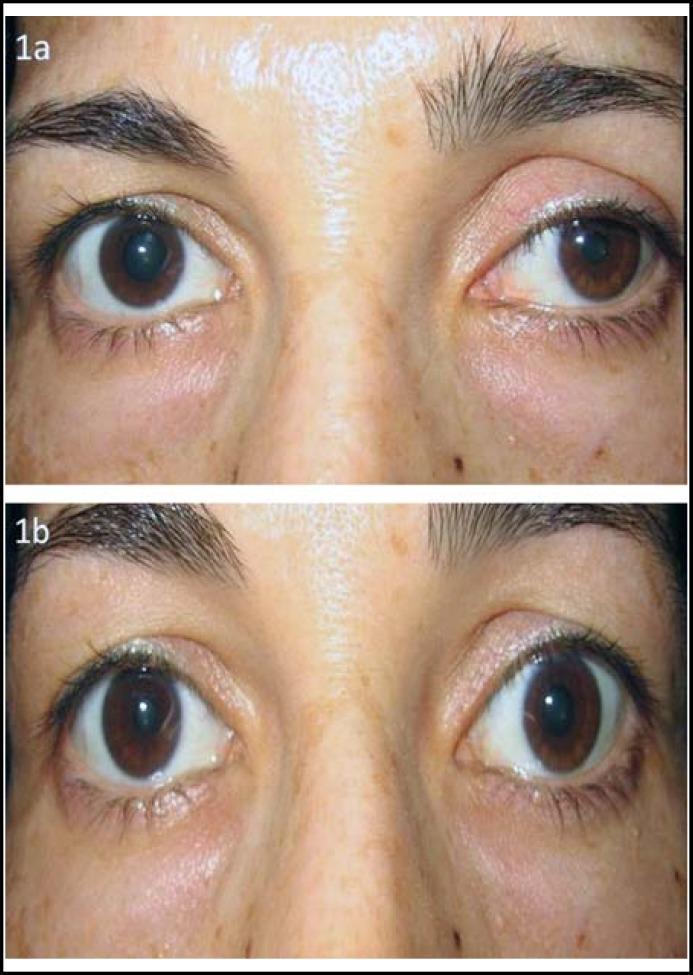
Classic Triad
| Sign | Mechanism |
|---|---|
| Ptosis (partial, ~1–2 mm) | Loss of innervation to Müller's smooth muscle in the upper lid |
| Miosis (small pupil) | Loss of sympathetic input to the pupillary dilator muscle |
| Anhidrosis | Loss of sympathetic innervation to ipsilateral sweat glands of face/neck |
Additional findings:
- Dilation lag — the affected pupil dilates more slowly than the contralateral pupil when lights are extinguished; this is often the most reliable sign
- Upside-down ptosis — lower lid elevation (elevation of the inferior tarsal muscle) causing a narrowed palpebral fissure
- Apparent enophthalmos — an illusion caused by the narrowed fissure, not true retraction
- Heterochromia iridis — in congenital cases, the affected iris is lighter (lack of pigmentation)
- Conjunctival injection — in acute cases
Key distinction: Anisocoria is more obvious in the dark than in ambient light (contrast with 3rd nerve palsy, where the large pupil is more apparent in light). The direct and consensual light reflexes are intact.
Anatomy: The Three-Neuron Arc
1st Neuron (Central) — Hypothalamus → Ciliospinal centre of Budge (C8–T2)
↓
2nd Neuron (Preganglionic) — Exit spinal cord → sympathetic chain →
around subclavian/carotid arteries → Superior cervical ganglion
↓
3rd Neuron (Postganglionic) — Along internal carotid → cavernous sinus →
V1 ophthalmic division → ciliary nerves → iris dilator & Müller's muscle
Causes by Lesion Location
First-order (Central) neuron
Hypothalamus to C8–T2 cord
- Lateral medullary (Wallenberg) syndrome — most classic central cause
- Pontine or brainstem stroke/haemorrhage/tumour
- Syringomyelia
- High cervical cord trauma (bilateral Horner in high transection)
- Multiple sclerosis
Second-order (Preganglionic) neuron
Ciliospinal centre to superior cervical ganglion
- Pancoast tumour (apical lung tumour) — most important peripheral cause
- Cervical rib / apical pleural disease
- Thyroid or mediastinal tumours
- Aortic aneurysm
- Brachial plexus injury (e.g., birth trauma → congenital Horner)
- Anterior/posterior thoracotomy
Third-order (Postganglionic) neuron
Superior cervical ganglion to orbit
- Carotid artery dissection — key vascular emergency; neck/face pain + Horner = dissection until proven otherwise
- Cavernous sinus lesion (thrombosis, aneurysm, tumour)
- Cluster headache (painful postganglionic Horner)
- Orbital lesion
- Nasopharyngeal carcinoma
Sweating pattern as localiser: Lesions at or proximal to the common carotid → anhidrosis of the entire face. Lesions distal to the carotid bifurcation → no sweating loss, or only medial forehead/nose (because facial sweating fibres travel with the external carotid, not the internal carotid). — Adams and Victor's Principles of Neurology, 12th Ed.
Pharmacological Testing
| Drug | Result in Horner | Interpretation |
|---|---|---|
| Cocaine 4–10% (blocks NE reuptake) | Fails to dilate affected pupil | Confirms oculosympathetic defect (any level) |
| Apraclonidine 0.5–1% (α-1 agonist) | Reversal of anisocoria — affected pupil dilates, normal pupil constricts | Confirms denervation supersensitivity; now preferred over cocaine |
| Hydroxyamphetamine 1% (releases NE from intact terminals) | No dilation = postganglionic (3rd neuron) lesion; Dilation = 1st or 2nd neuron lesion | Localises lesion to pre- vs. postganglionic |
The apraclonidine test exploits denervation supersensitivity — the denervated dilator muscle upregulates α-1 receptors and responds excessively to even a weak agonist. Wait ≥24–48 h after acute onset before testing (supersensitivity takes time to develop). — Neuroanatomy through Clinical Cases, 3rd Ed.
Differential Diagnosis of Anisocoria
| Condition | Dark Room | Light Room | Light Reflex | Key Feature |
|---|---|---|---|---|
| Horner syndrome | Anisocoria obvious | Less obvious | Intact | Dilation lag, ptosis |
| CN III palsy | Less obvious | Anisocoria obvious | Absent | Mydriasis, ophthalmoplegia |
| Afferent pupillary defect | No anisocoria | No anisocoria | Relative afferent defect | Swinging flashlight test |
| Physiological | Equal in both conditions | Equal | Intact | <0.6 mm, no other signs |
Workup / Imaging
Once confirmed pharmacologically, imaging is directed by clinical context:
- Acute painful Horner (neck pain, headache) → urgent MRI/MRA neck and brain to exclude carotid dissection
- Smoker / weight loss / shoulder pain → CT chest for Pancoast tumour
- Isolated, painless, chronic → MRI brain + neck (C8–T2 cord, mediastinum)
- Children → rule out neuroblastoma (urine catecholamines, chest/abdominal imaging)
Congenital Horner
- Usually caused by perinatal injury to the sympathetic chain in the neck (birth trauma)
- An autosomal dominant hereditary form also exists
- Key feature: heterochromia iridis — affected iris remains lighter because sympathetic innervation is needed for melanin deposition during development
- — Adams and Victor's Principles of Neurology, 12th Ed.
Key Associations to Remember
| Association | Cause |
|---|---|
| Horner + ipsilateral ataxia + contralateral pain/temp loss | Lateral medullary syndrome (Wallenberg) |
| Horner + ipsilateral shoulder/arm pain + lower brachial plexopathy | Pancoast tumour |
| Horner + acute neck pain after trivial trauma | Carotid artery dissection |
| Horner + severe periorbital pain, autonomic symptoms | Cluster headache (postganglionic) |
| Bilateral Horner | High cervical cord lesion, autonomic neuropathy |
| Horner in infant with heterochromia | Congenital / birth injury |
Sources: Adams and Victor's Principles of Neurology, 12th Ed. | Neuroanatomy through Clinical Cases, 3rd Ed. | Rosen's Emergency Medicine | Ganong's Review of Medical Physiology, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.