IUGR
Reading File
search_medical_text
intrauterine growth restriction IUGR etiology classification pathophysiology
search_medical_text
IUGR diagnosis surveillance management fetal monitoring
search_medical_image
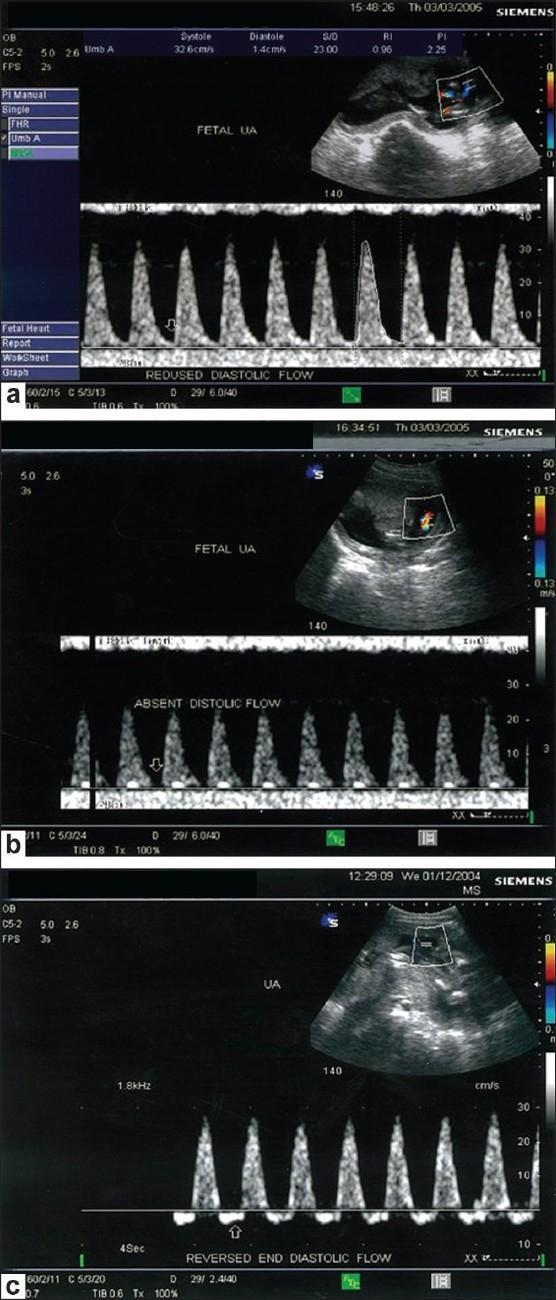
IUGR fetal Doppler umbilical artery waveform
GradeResponse
GradeResponse
GradeResponse
search_medical_text
small for gestational age SGA fetal growth restriction causes maternal fetal placental
search_medical_text
fetal growth restriction Doppler biophysical profile delivery timing neonatal outcome
GradeResponse
GradeResponse
The retrieved results are limited, so I'll synthesize a comprehensive answer drawing from my clinical knowledge, supplemented by the retrieved content.
Intrauterine Growth Restriction (IUGR)
Definition & Classification
IUGR refers to a fetus that fails to reach its genetically predetermined growth potential, typically defined as an estimated fetal weight (EFW) or abdominal circumference (AC) < 10th percentile for gestational age on ultrasound, with evidence of a pathological process (distinguishing it from constitutional smallness).
| Term | Definition |
|---|---|
| SGA (Small for Gestational Age) | Birth weight < 10th percentile; may be constitutional |
| IUGR | Pathological failure to reach growth potential (< 10th percentile + Doppler/functional compromise) |
| Severe IUGR | EFW < 3rd percentile |
Two phenotypes:
- Symmetric IUGR (~20–30%): All parameters reduced proportionally; onset early (< 28 wks); often fetal/chromosomal cause
- Asymmetric IUGR (~70–80%): Head-sparing with reduced abdominal circumference; onset late; typically placental/uteroplacental insufficiency
Etiology
Maternal (~25–30%)
- Hypertensive disorders (preeclampsia, chronic hypertension)
- Diabetes with vascular disease
- Autoimmune conditions (antiphospholipid syndrome, SLE)
- Chronic renal disease
- Severe anemia, malnutrition, underweight
- Smoking, alcohol, cocaine use
- PCOS (OR ~1.77 vs. non-PCOS pregnancies; Assessment and Management of PCOS, p. 136)
- Thrombophilias
Placental (~40%)
- Placental insufficiency / uteroplacental insufficiency (most common)
- Placenta previa, abruption
- Velamentous cord insertion
- Circumvallate placenta
Fetal (~15%)
- Chromosomal anomalies (trisomy 13, 18, 21; Turner syndrome)
- Structural congenital anomalies
- Inborn errors of metabolism
- Multiple gestation (twin-twin transfusion)
Infectious (~5–10%)
- TORCH infections: Toxoplasma, Other (syphilis, VZV, parvovirus B19), Rubella, CMV, Herpes
Pathophysiology
The final common pathway is reduced oxygen and nutrient delivery to the fetus:
- Defective trophoblast invasion → inadequate spiral artery remodeling
- Increased placental vascular resistance → ↑ umbilical artery pulsatility
- Fetal redistribution response: vasodilation of cerebral/coronary/adrenal circulation ("brain-sparing" = ↓ MCA resistance)
- Progressive decompensation: absent/reversed end-diastolic flow (AEDF/REDF) in umbilical artery → venous pulsations in ductus venosus → fetal death
Diagnosis
Screening
- Uterine artery Doppler at 20–24 weeks (↑ PI / notching predicts placental insufficiency)
- Serial symphysis-fundal height (SFH) measurements — flattening or lag triggers ultrasound
Ultrasound Biometry
- Abdominal circumference (AC) — most sensitive single parameter
- EFW < 10th percentile (severe < 3rd percentile)
- Serial measurements every 2–4 weeks to assess growth velocity (crossing centiles is as important as absolute value)
Doppler Studies (key for surveillance & timing)
| Doppler Vessel | Finding | Significance |
|---|---|---|
| Umbilical artery (UA) | ↑ PI / S:D ratio | Placental resistance |
| UA | Absent end-diastolic flow (AEDF) | High risk — consider delivery |
| UA | Reversed end-diastolic flow (REDF) | Imminent deterioration — urgent delivery |
| Middle cerebral artery (MCA) | ↓ PI (brain-sparing) | Cerebrovascular redistribution |
| Cerebroplacental ratio (CPR) | < 1 | Independent predictor of adverse outcome |
| Ductus venosus (DV) | Absent/reversed A-wave | Pre-terminal; delivery indicated |
Biophysical Profile (BPP)
- Scores fetal tone, movement, breathing, amniotic fluid, and NST (0–10)
- Score ≤ 4: high risk of acidosis, consider delivery
- Score 6: repeat in 4–6 hours
Management
Antepartum
- Identify and treat underlying cause (e.g., optimize BP in hypertension, treat infection)
- Aspirin (low-dose, 100–150 mg/day from 11–14 weeks): reduces risk of placental IUGR in high-risk women
- No proven intervention improves growth directly once IUGR is established
- Optimize maternal nutrition, stop smoking/drugs
- Corticosteroids if preterm delivery anticipated (< 34 weeks)
- Magnesium sulfate for neuroprotection if < 32 weeks
Surveillance Frequency
| Severity | UA Doppler | BPP/NST | Growth USS |
|---|---|---|---|
| EFW < 10th, normal Doppler | Every 2 weeks | Weekly | Every 2–4 weeks |
| Abnormal UA PI, normal diastole | Twice weekly | Twice weekly | Every 2 weeks |
| AEDF | 2–3× weekly | Daily BPP | Every 1–2 weeks |
| REDF | Daily | Daily | — |
| Abnormal DV | Deliver | — | — |
Timing of Delivery
| Gestational Age | Indication | Recommended Action |
|---|---|---|
| ≥ 37 weeks | Any IUGR | Deliver |
| 34–37 weeks | AEDF, deteriorating BPP | Consider delivery |
| 32–34 weeks | REDF, BPP ≤ 4 | Deliver after steroids |
| < 32 weeks | Abnormal DV, BPP ≤ 4 | Deliver (balance prematurity risk) |
ACOG recommends delivery at 36–37 weeks for most cases of placental IUGR.
Mode of Delivery
- Vaginal delivery is acceptable if no acute compromise
- Continuous electronic fetal monitoring in labor is mandatory
- Low threshold for cesarean section with abnormal Dopplers (AEDF/REDF) or non-reassuring CTG
Complications
Perinatal
- Stillbirth / intrauterine fetal demise (IUFD)
- Birth asphyxia, meconium aspiration
- Hypoglycemia, hypothermia, polycythemia
- Necrotizing enterocolitis (NEC)
- Respiratory distress syndrome (prematurity)
- Neurodevelopmental impairment
Long-term (Barker Hypothesis / Fetal Origins of Adult Disease)
- Hypertension, coronary artery disease
- Type 2 diabetes / insulin resistance
- Obesity
- SGA is associated with ↑ risk of hypertension and diabetes in the offspring (Management of CVD and Pregnancy, p. 78)
Key Points Summary
- IUGR ≠ SGA — IUGR implies pathological growth failure confirmed by Doppler/functional compromise
- Placental insufficiency is the most common cause in developed countries
- Umbilical artery Doppler is the cornerstone of surveillance — AEDF/REDF are delivery triggers
- No treatment restores normal fetal growth; management is surveillance + timely delivery
- Long-term cardiovascular and metabolic risks are significant for both mother and offspring
This is a shared conversation. Sign in to Orris to start your own chat.