Acoustic and non acoustic reflexes and their importance 10 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, exam-ready 10-mark answer for your MS ENT examination:
Acoustic and Non-Acoustic Reflexes and Their Importance
Introduction
The middle ear contains two muscles - the stapedius (smallest skeletal muscle in the body, innervated by CN VII) and the tensor tympani (innervated by CN V3 via the otic ganglion). Both muscles stiffen the ossicular chain when they contract, increasing middle ear impedance. Their reflexes are classified based on the stimulus that triggers them.
I. The Acoustic Reflex (Stapedial Reflex)
Definition
The acoustic reflex is the contraction of the stapedius muscle in response to a loud sound stimulus. It is the dominant sound-evoked middle ear muscle reflex in humans. (In some animals, the tensor tympani also contracts in response to sound, but in humans the stapedius reflex is the primary pathway.)
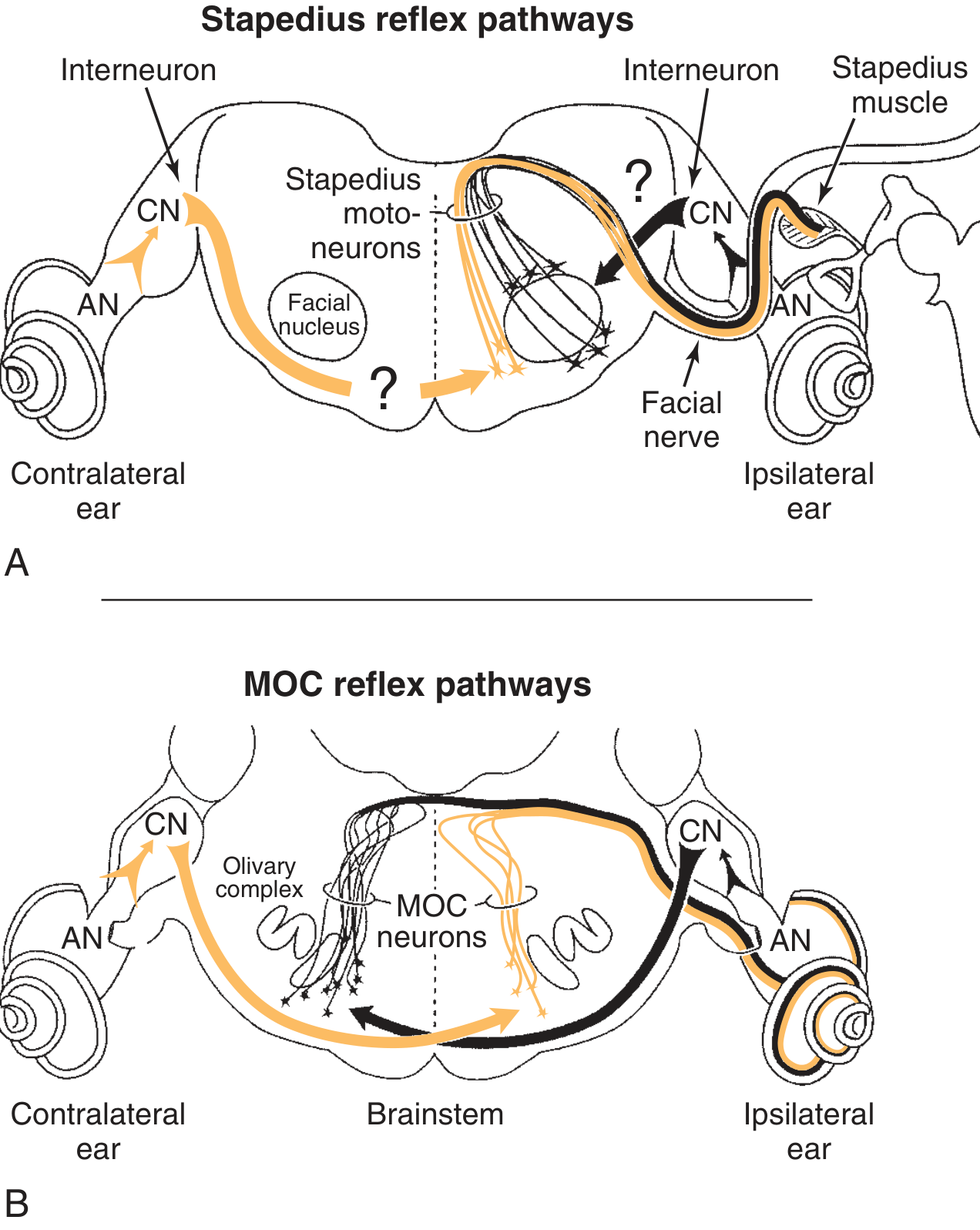
Reflex Arc
A. Ipsilateral acoustic reflex (stimulus and recording in same ear):
- Loud sound → Cochlea → Auditory nerve (CN VIII)
- Ipsilateral ventral cochlear nucleus
- Trapezoid body
- Ipsilateral facial motor nucleus (or ipsilateral medial superior olive)
- Ipsilateral facial nerve (CN VII)
- Ipsilateral stapedius muscle contracts
B. Contralateral acoustic reflex (crossed reflex):
- Loud sound → Cochlea → Auditory nerve (CN VIII)
- Ipsilateral ventral cochlear nucleus
- Crosses via trapezoid body to contralateral medial superior olive
- Contralateral facial motor nucleus
- Contralateral facial nerve
- Contralateral stapedius muscle
A unilateral sound stimulus produces bilateral stapedius contraction - analogous to the consensual pupillary light reflex.
Normal Values
| Parameter | Normal Value |
|---|---|
| Acoustic Reflex Threshold (ART) | 70-100 dB HL for pure tones |
| Sensation level at which reflex occurs | ~70 dB SL |
| Acoustic Reflex Decay test signal | 10 dB above ART for 10 seconds |
| Abnormal decay | Amplitude falls to <50% within 5 seconds |
II. Non-Acoustic Reflexes
These are reflexes that cause contraction of the middle ear muscles in response to non-auditory stimuli.
1. Tensor Tympani Reflex (Startle Reflex)
- Triggered by sudden non-acoustic stimuli: tactile stimulation (touch to face/body), sudden bright light, air puffs, and startle reactions
- Tensor tympani is innervated by CN V3 (mandibular branch of trigeminal) via the otic ganglion
- Contracts and pulls the malleus medially, stiffening the TM and ossicles
- In humans, tensor tympani shows minimal electrical activity in response to sound but responds measurably to stimuli causing a startle reaction
2. Self-Vocalization Reflex
- The stapedius muscle also contracts in response to self-generated vocalization (speaking, singing)
- This is a non-acoustic reflex protecting the inner ear from the speaker's own voice
- Cortical input modulates both middle ear muscles via this pathway
3. Electrical Stimulation Reflex
- In patients with bilateral profound sensorineural hearing loss, the stapedius reflex can be elicited by direct electrical stimulation (e.g., cochlear implant activation)
- Used clinically to assess facial nerve integrity in the deaf
4. Tactile/Cutaneous Reflex
- Touch to the perioral or periocular region can trigger tensor tympani contraction
- Pathway: Trigeminal afferents → trigeminal sensory nucleus → trigeminal motor nucleus → tensor tympani
III. Clinical Importance
A. Detection of Cochlear (Sensory) Lesions
- In cochlear hearing loss with loudness recruitment, the acoustic reflex occurs at a sensation level less than 60 dB above the pure-tone threshold
- This is because recruitment causes abnormally rapid growth of loudness - the reflex threshold is reached at a lower sensation level
- Useful for identifying cochlear (vs. neural) site of lesion
B. Detection of Retrocochlear (Neural) Lesions
- In vestibular schwannoma (acoustic neuroma) or eighth nerve lesions:
- Acoustic reflexes are often absent when the affected ear is stimulated
- Even if present, there is abnormal acoustic reflex decay (amplitude falls >50% within 5 seconds at 500 or 1000 Hz)
- Key principle: the degree of threshold elevation is disproportionate to the degree of audiometric loss
- Absence of contralateral reflexes with intact ipsilateral reflexes suggests a brainstem lesion affecting the crossed pathways
C. Topographic Diagnosis of Facial Nerve Lesions
- The nerve to stapedius branches from the facial nerve just past the second genu in the mastoid segment
- If the facial nerve lesion is proximal to the stapedius branch (high lesion): acoustic reflex is absent
- If the lesion is distal to the stapedius branch: acoustic reflex is present
- This allows localization of facial nerve injury along its course
- Fisch reported absent stapedius reflex in 69% of Bell's palsy (84% in complete paralysis)
- Recovery of the stapedius reflex within 4 weeks of facial paralysis predicts full facial recovery within 24 weeks - prognostic value
D. Detection of Conductive Hearing Loss
- Any middle ear disorder (fluid, ossicular fixation) prevents the TM from showing compliance change during stapedius contraction
- Reflexes are absent bilaterally when there is a conductive loss in the test ear
- Threshold: conductive loss >40 dB in the stimulus ear, or >10 dB in the probe (recording) ear abolishes the reflex
E. Acoustic Reflex Decay Test
- Presents a signal 10 dB above ART for 10 seconds
- Abnormal: amplitude decreases to ≤50% of original within 5 seconds
- Tested at 500 Hz and 1000 Hz (decay at higher frequencies is common in normal ears)
- Positive decay = retrocochlear disease (the nerve cannot sustain firing under continuous stimulation)
- Those with cochlear or conductive loss will show negative decay if a reflex is present
F. Protective Function
- Contraction of middle ear muscles increases ossicular impedance, attenuating sound reaching the cochlea
- This attenuation is frequency-dependent - more pronounced for low frequencies
- This protects against intense background noise (which is typically low frequency) and preserves speech frequency information
- Limitation: the reflex latency is ~25-150 ms - too slow to protect against impulsive noise (gunshots, explosions)
G. Audiological Test Battery Summary
| Condition | Ipsilateral Reflex | Contralateral Reflex | Decay |
|---|---|---|---|
| Normal | Present | Present | Negative |
| Conductive loss (probe ear) | Absent | Absent | - |
| Cochlear SNHL >70 dB | Absent | Absent | Negative |
| Cochlear SNHL <60 dB | At low SL (recruitment) | Present | Negative |
| Retrocochlear (8th nerve) | Absent or elevated threshold | Absent | Positive |
| Brainstem lesion | Variable | Absent with normal ipsi | Variable |
| Facial palsy (proximal) | Absent | Present (opposite side) | - |
Summary
The acoustic reflex (stapedius, CN VII, triggered by loud sound) and non-acoustic reflexes (tensor tympani, CN V3, triggered by startle/tactile stimuli) form the middle ear muscle reflex system. Their clinical importance spans: site-of-lesion audiometry (cochlear vs. retrocochlear vs. conductive), topographic facial nerve diagnosis, prognosis in Bell's palsy, and physiological cochlear protection. The acoustic reflex threshold and decay test are essential components of the impedance audiometry battery in ENT practice.
Sources: Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology; Shambaugh Surgery of the Ear; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.