Areas of auslation air entery names and benefits of vaious patint on patinet in icu and waht is ventilation and percussion how it helps in postion
lung auscultation areas air entry breath sounds names
ICU patient positioning types benefits prone supine lateral
lung auscultation areas diagram chest
chest physiotherapy percussion vibration postural drainage technique ICU
Auscultation, Patient Positioning in ICU & Chest Physiotherapy
1. Areas of Auscultation & Air Entry
Auscultation Points (Standard 8-Point Protocol)
| Point | Location | Side |
|---|---|---|
| L1 / R1 | 2nd Intercostal Space (ICS), Midclavicular Line | Right / Left (Anterior Upper) |
| L2 / R2 | 5th ICS, Midclavicular Line | Right / Left (Anterior Lower) |
| L3 / R3 | 4th ICS, Midaxillary Line | Right / Left (Lateral) |
| L4 / R4 | 10th ICS, Midaxillary Line | Right / Left (Lateral Lower) |
| Posterior Upper | Between spine and scapula, upper third | Bilateral |
| Posterior Lower | Below scapula, 9th–10th ICS | Bilateral |
Always auscultate apex to base, comparing side to side.
Types of Breath Sounds on Auscultation
| Breath Sound | Normal Location | Character | Significance |
|---|---|---|---|
| Vesicular | Most lung fields | Soft, low-pitched, inspiratory > expiratory | Normal peripheral lung |
| Bronchial | Over trachea/manubrium | Loud, high-pitched, expiratory > inspiratory | If heard peripherally = consolidation |
| Bronchovesicular | 1st–2nd ICS anteriorly, between scapulae posteriorly | Medium pitch, I = E | Normal at these sites |
| Tracheal | Over trachea | Very loud, harsh | Normal |
Added (Adventitious) Sounds
| Sound | Description | Cause |
|---|---|---|
| Crackles (Rales) | Fine or coarse popping sounds, inspiratory | Pulmonary edema, pneumonia, fibrosis |
| Wheeze | High-pitched musical, expiratory | Bronchospasm, asthma, COPD |
| Rhonchi | Low-pitched, coarser, clears with cough | Secretions in large airways |
| Stridor | High-pitched inspiratory | Upper airway obstruction |
| Pleural Rub | Grating, leathery sound | Pleuritis |
| Egophony | "EEE" sounds like "AYY" | Consolidation (pneumonia) |
| Bronchophony / Whispered Pectoriloquy | Increased transmission of voice sounds | Consolidation |
2. Patient Positions in the ICU — Types & Benefits
A. Supine Position (Flat on Back)
- When used: Standard resting position, hemodynamically unstable patients, spinal precautions
- Benefits: Easy access for procedures, resuscitation, monitoring
- Risks: Promotes atelectasis, aspiration, pressure ulcers, VAP (ventilator-associated pneumonia)
B. Semi-Recumbent / Head of Bed 30–45°
- Standard of care for all ventilated ICU patients
- Benefits:
- ↓ Risk of aspiration and VAP
- ↓ Gastroesophageal reflux
- Improves diaphragm excursion vs. flat supine
- Recommended by CDC and SCCM guidelines
C. Prone Position (Face Down)
- When used: Moderate-to-severe ARDS (PaO₂/FiO₂ < 150 mmHg)
- Benefits (PROSEVA Trial 2013; ESICM/ATS 2017 Guidelines):
- Improves oxygenation by recruiting dependent (dorsal) lung zones
- Better homogenization of lung stress — reduces ventilator-induced lung injury
- Decreases right ventricular strain
- Reduces V/Q mismatch
- Mortality benefit: 16-hour/day prone sessions → significant reduction in 28-day mortality
- Risks: Pressure sores (face, chest), accidental extubation, hemodynamic instability
D. Lateral Decubitus (Side-Lying)
- When used: Unilateral lung disease, to aid secretion clearance, postural drainage
- Benefits:
- "Good lung down" position improves oxygenation to healthier lung
- Facilitates drainage of secretions from affected lobes
- Reduces aspiration risk
E. Trendelenburg (Head-Down Tilt)
- When used: Shock (historically), postural drainage of upper lobes, central line insertion
- Benefits: Increases venous return in hypotension
- Risks: Increases ICP, worsens respiratory effort — now used selectively
F. Reverse Trendelenburg (Head-Up Tilt)
- When used: ↑ Intracranial pressure, facial/airway edema, bariatric patients
- Benefits: Reduces cerebral venous congestion, improves respiratory mechanics in obese patients
G. Sitting / High Fowler's Position (≥60°)
- When used: Respiratory distress, post-extubation, post-cardiac surgery
- Benefits: Maximum diaphragm descent, best FRC (functional residual capacity), eases work of breathing
3. Chest Physiotherapy: Percussion & Vibration
A. Percussion (Clapping)
- Creates mechanical energy waves transmitted through the chest wall into lung tissue
- Loosens and dislodges thick, adherent mucus from bronchial walls
- Moves secretions from smaller airways → larger airways → trachea → can be suctioned or coughed out
- Position the patient for the target lobe (see below)
- Cup hands and rhythmically clap at 40–60 claps/minute
- Apply for 3–5 minutes per segment
- Follow with vibration and/or suctioning
B. Vibration
- Oscillations are transmitted into airways, promoting mucus movement toward the central airways
- Enhances mucociliary clearance
- Works synergistically with percussion
C. Postural Drainage — Position + Percussion/Vibration
| Lobe/Segment | Patient Position |
|---|---|
| Upper lobe — Apical | Sitting upright, slightly reclined |
| Upper lobe — Anterior | Supine, flat |
| Upper lobe — Posterior | Sitting, leaning forward |
| Middle lobe / Lingula | Left/right lateral, foot of bed raised 15°, rotated slightly |
| Lower lobe — Anterior | Supine, Trendelenburg (foot raised 30°) |
| Lower lobe — Posterior | Prone, Trendelenburg (foot raised 30°) |
| Lower lobe — Lateral | Lateral decubitus, foot raised |
Summary: How Percussion + Vibration + Position Work Together
Position (gravity-assisted drainage)
+
Percussion (loosens secretions)
+
Vibration (moves secretions centrally)
+
Cough / Suction (expels secretions)
= Effective Airway Clearance in ICU
- Prevents and treats atelectasis
- Reduces risk of ventilator-associated pneumonia (VAP)
- Improves oxygenation and lung compliance
- Facilitates weaning from mechanical ventilation
- Clears secretions in patients unable to cough (sedated/intubated)
Clinical Pearl: In intubated ICU patients, percussion and vibration are always followed by endotracheal suctioning to remove the mobilized secretions, since the cough reflex is suppressed.
What is ventilation perfusion ration normal values and benifits in postion of ventilation perfusion
ventilation perfusion ratio normal values V/Q ratio physiology
ventilation perfusion mismatch positioning effects prone lateral ICU oxygenation
ventilation perfusion ratio V/Q lung zones diagram
Ventilation/Perfusion (V/Q) Ratio — Normal Values, Physiology & Effect of Positioning
1. What is the V/Q Ratio?
V/Q = Alveolar Ventilation ÷ Pulmonary Blood Flow
2. Normal Values
| Parameter | Normal Value |
|---|---|
| Overall V/Q ratio (whole lung) | 0.8 (approx.) |
| Total alveolar ventilation (V̇) | ~4 L/min |
| Total pulmonary perfusion (Q̇) | ~5 L/min |
| V/Q at lung apex (Zone 1) | ~3.3 (high — more ventilation than perfusion) |
| V/Q at lung base (Zone 3) | ~0.6 (low — more perfusion than ventilation) |
| V/Q = ∞ (dead space) | Ventilation with NO perfusion (e.g., pulmonary embolism) |
| V/Q = 0 (shunt) | Perfusion with NO ventilation (e.g., consolidation, atelectasis) |
The normal lung has minor V/Q heterogeneity even in health, primarily due to gravity and differences in airway/vascular architecture (Harrison's Principles, p. 7864).
3. West's Lung Zones — V/Q Distribution in the Upright Lung
APEX (Zone 1)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
V̇ HIGH | Q̇ LOW → V/Q ~3.3
Alveoli are OVER-ventilated relative to perfusion
→ Acts like "physiologic dead space"
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
MIDDLE (Zone 2)
V̇ MEDIUM | Q̇ MEDIUM → V/Q ~1.0
Best matching of ventilation and perfusion
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
BASE (Zone 3)
V̇ LOW | Q̇ HIGH → V/Q ~0.6
Alveoli are UNDER-ventilated relative to perfusion
→ Acts like "physiologic shunt"
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
| Zone | Ventilation | Perfusion | V/Q | Effect |
|---|---|---|---|---|
| Apex (Zone 1) | High | Low | ~3.3 | Dead space-like |
| Middle (Zone 2) | Moderate | Moderate | ~1.0 | Ideal matching |
| Base (Zone 3) | Lower | High | ~0.6 | Shunt-like |
4. Two Extremes of V/Q Mismatch
A. V/Q = ∞ (Dead Space)
- Ventilation present, NO perfusion
- Example: Pulmonary embolism — clot blocks blood flow to a ventilated alveolus
- Air is "wasted" — no gas exchange occurs
- ↑ Dead space → ↑ PaCO₂ (hypercapnia)
B. V/Q = 0 (Shunt)
- Perfusion present, NO ventilation
- Example: Atelectasis, consolidation (pneumonia), ARDS
- Venous (deoxygenated) blood passes through lung without being oxygenated
- ↑ Shunt → ↓ PaO₂ (hypoxemia) — does NOT respond well to supplemental O₂
5. V/Q Scan (Scintigraphy)
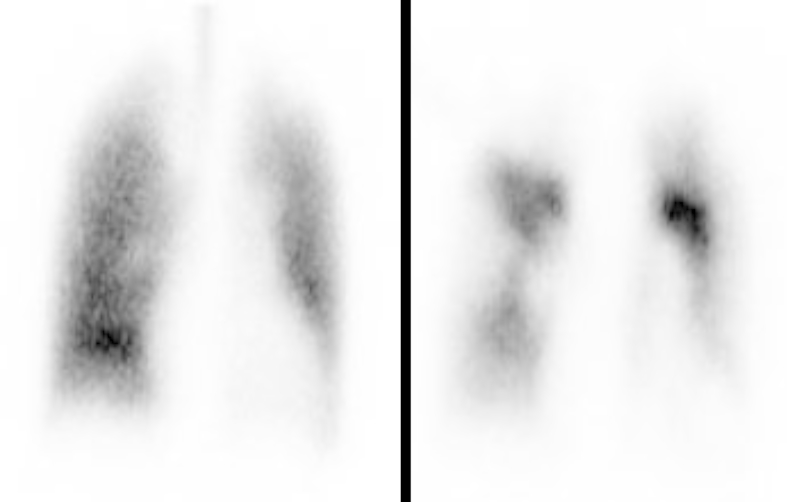
| V/Q Scan Result | Meaning |
|---|---|
| Matched defect (both V and Q abnormal in same area) | Suggests COPD, pneumonia |
| Mismatched defect (Q abnormal, V normal) | High probability for PE |
| Normal scan | Effectively rules out PE |
6. How Patient Positioning Improves V/Q Ratio
A. Prone Positioning
- In supine ARDS patients, the dorsal (back) lung is compressed by the heart and abdominal contents → collapsed, non-ventilated but still perfused → V/Q = 0 (shunt)
- Turning prone:
- Recruits dorsal alveoli (now non-dependent) → restores ventilation
- Reduces ventral over-distension
- Makes ventilation distribution more homogeneous
- Reduces dorsal-ventral transpulmonary pressure differences
- Improves perfusion distribution
Result: ↓ Shunt fraction → ↑ PaO₂/FiO₂ ratio → Better oxygenation
B. Lateral Decubitus ("Good Lung Down")
- Dependent lung (lower lung) receives more perfusion (gravity)
- If that lung is also better ventilated → improved V/Q matching
- Used in unilateral lung disease (e.g., one-sided pneumonia, pleural effusion)
- "Good lung down" = place the healthier lung in the dependent (lower) position to maximize its perfusion and ventilation matching
| Condition | Optimal Position | Rationale |
|---|---|---|
| Left lung pneumonia | Right lateral decubitus (right lung down) | Good right lung gets more perfusion |
| Right-sided pleural effusion | Left lateral decubitus | Good left lung gets more perfusion |
C. Sitting / Semi-Upright (High Fowler's 45–90°)
- Opens dependent basal alveoli
- Improves diaphragm excursion
- ↑ FRC (functional residual capacity)
- Reduces atelectasis at lung bases
- Better V/Q matching at the bases (Zone 3 ventilation improves)
D. Supine Position
- Basal lung zones compressed by abdominal organs
- Dorsal alveoli collapse → V/Q = 0 (shunt)
- Worsens oxygenation — should be avoided in respiratory failure
7. Summary Table — Positioning & V/Q Effects
| Position | Effect on Ventilation | Effect on Perfusion | V/Q Effect | Use In |
|---|---|---|---|---|
| Prone | Homogeneous, dorsal recruitment | Redistributed, more uniform | ↓ Shunt, ↑ V/Q matching | ARDS, severe hypoxemia |
| Lateral (good lung down) | Good lung ventilated better | Good lung perfused more | ↑ V/Q in good lung | Unilateral lung disease |
| Semi-recumbent 30–45° | ↑ FRC, ↓ atelectasis | Mild improvement | Moderate improvement | All ICU/ventilated patients |
| Sitting (>60°) | Best diaphragm movement | Normal distribution | Best overall V/Q | Spontaneously breathing |
| Supine flat | Basal collapse | Excess basal perfusion | ↑ Shunt, ↓ V/Q | Avoid in respiratory failure |
| Trendelenburg | Basal compression worsens | ↑ Apical perfusion | Worsens V/Q | Avoid in respiratory failure |
Key Clinical Takeaway
The goal of positioning in respiratory patients is to match ventilation to perfusion. Since perfusion is gravity-dependent, placing the best-ventilated (or most recruitable) lung in the dependent position — or using prone positioning to homogenize both — is the most powerful non-pharmacological tool to improve V/Q ratio and oxygenation in ICU patients.
How it postion helps to improve conscious in patients in icu in detail with simple answer
patient positioning neurological consciousness improvement ICU head of bed elevation cerebral perfusion
positioning effects brain oxygenation arousal sedation reduction early mobilization ICU consciousness
How Positioning Helps Improve Consciousness in ICU Patients
Why ICU Patients Have Reduced Consciousness
| Reason | What Happens |
|---|---|
| Low oxygen (hypoxia) | Brain gets less O₂ → drowsy, confused |
| Low blood pressure | Less blood reaching brain → reduced alertness |
| High brain pressure (↑ ICP) | Brain gets squeezed → unconsciousness |
| Infections / sepsis | Toxins affect brain → delirium, confusion |
| Heavy sedation | Medications reduce alertness intentionally |
| Prolonged lying still | Reduces stimulation → brain becomes less active |
How Each Position Helps Improve Consciousness
1. 🛏️ Head of Bed Raised 30° (Semi-Recumbent)
Raising the head end of the bed to 30° is like tilting a water pipe — it allows excess fluid and pressure to drain away from the brain.
- ✅ Reduces Intracranial Pressure (ICP) — venous blood and CSF (brain fluid) drain more easily out of the skull
- ✅ Improves cerebral perfusion — stable blood flow reaches the brain
- ✅ Reduces brain swelling — helps brain cells recover faster
- ✅ Improves breathing → more oxygen → more alert brain
⚠️ Important: Going above 45° can sometimes reduce blood pressure to the brain (CPP drops). 30° is the sweet spot — it lowers ICP without reducing cerebral blood flow significantly.
2. 🔄 Upright / Sitting Position (High Fowler's 60–90°)
Sitting up stimulates the brain the same way waking up in the morning does — it signals the body that it's time to be alert.
- ✅ Sensory stimulation — upright posture activates the reticular activating system (RAS), the part of the brain responsible for wakefulness
- ✅ Better breathing → more oxygen to brain
- ✅ Reduces aspiration → fewer chest infections → less fever and toxins affecting the brain
- ✅ Encourages eye opening and interaction — gravity helps the patient "feel" the world
3. 🔃 Turning / Lateral Position (Side-Lying)
Lying on one side prevents pressure sores, keeps lungs clear, and allows better blood flow — all of which prevent complications that worsen consciousness.
- ✅ Prevents pressure ulcers — skin wounds cause pain and infection, which worsen brain function
- ✅ Clears lung secretions → better oxygenation → better brain function
- ✅ Prevents aspiration pneumonia → reduces fever/sepsis → less delirium
4. 🚶 Early Mobilization (Sitting at Edge of Bed / Standing)
Moving the patient — even just sitting them up at the edge of the bed — is like "waking the brain up" with natural stimulation.
- ✅ Activates the nervous system — movement sends signals to the brain
- ✅ Reduces ICU delirium (confusion/agitation) — one of the biggest causes of prolonged unconsciousness
- ✅ Improves blood circulation to all organs including the brain
- ✅ Reduces duration of mechanical ventilation → patient breathes more on their own → more alert
5. ⚠️ Positions to AVOID in Unconscious/Brain-Injured Patients
| Position | Why It Is Harmful |
|---|---|
| Flat supine (0°) | ↑ ICP, ↑ aspiration risk, worsens brain swelling |
| Head-down (Trendelenburg) | Blood pools in the brain → dangerously ↑ ICP |
| Neck flexed or rotated | Compresses jugular veins → impairs venous drainage from brain → ↑ ICP |
Simple Summary — Step by Step
Patient lying flat
↓
Brain swelling ↑, Oxygen ↓, Brain gets less blood
↓
Less conscious / confused / not responding
Raise head of bed to 30°
↓
Brain swelling ↓, Oxygen ↑, Better blood flow to brain
↓
Patient becomes more alert, opens eyes, responds
Quick Reference Table
| Position | Brain Benefit | Why It Helps Consciousness |
|---|---|---|
| 30° Head elevation | ↓ ICP, stable CPP | Best for brain-injured/swollen brain |
| 45–60° Semi-sitting | ↑ Oxygenation, ↓ aspiration | More oxygen = more alert |
| Lateral (side-lying) | Clears airway, prevents infections | Less chest infection = less delirium |
| Upright / sitting | Activates wakefulness centers | Natural stimulus to be conscious |
| Early mobilization | ↓ Delirium, ↑ nerve stimulation | Brain "wakes up" with movement |
| Flat/Trendelenburg | ↑ ICP ❌ | Avoid — worsens consciousness |
Bottom Line: In ICU, positioning is not just about comfort — it is a direct treatment for the brain. The right angle reduces pressure on the brain, increases oxygen delivery, prevents dangerous complications like delirium and pneumonia, and sends natural signals to the brain to stay awake and alert.