Electrical events of cardiac cycle
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Electrical Events of the Cardiac Cycle
The cardiac cycle is driven by a precisely timed sequence of electrical events - impulse generation, conduction, depolarization, and repolarization - that are reflected on the surface ECG as distinct waves and intervals.
1. The Normal ECG
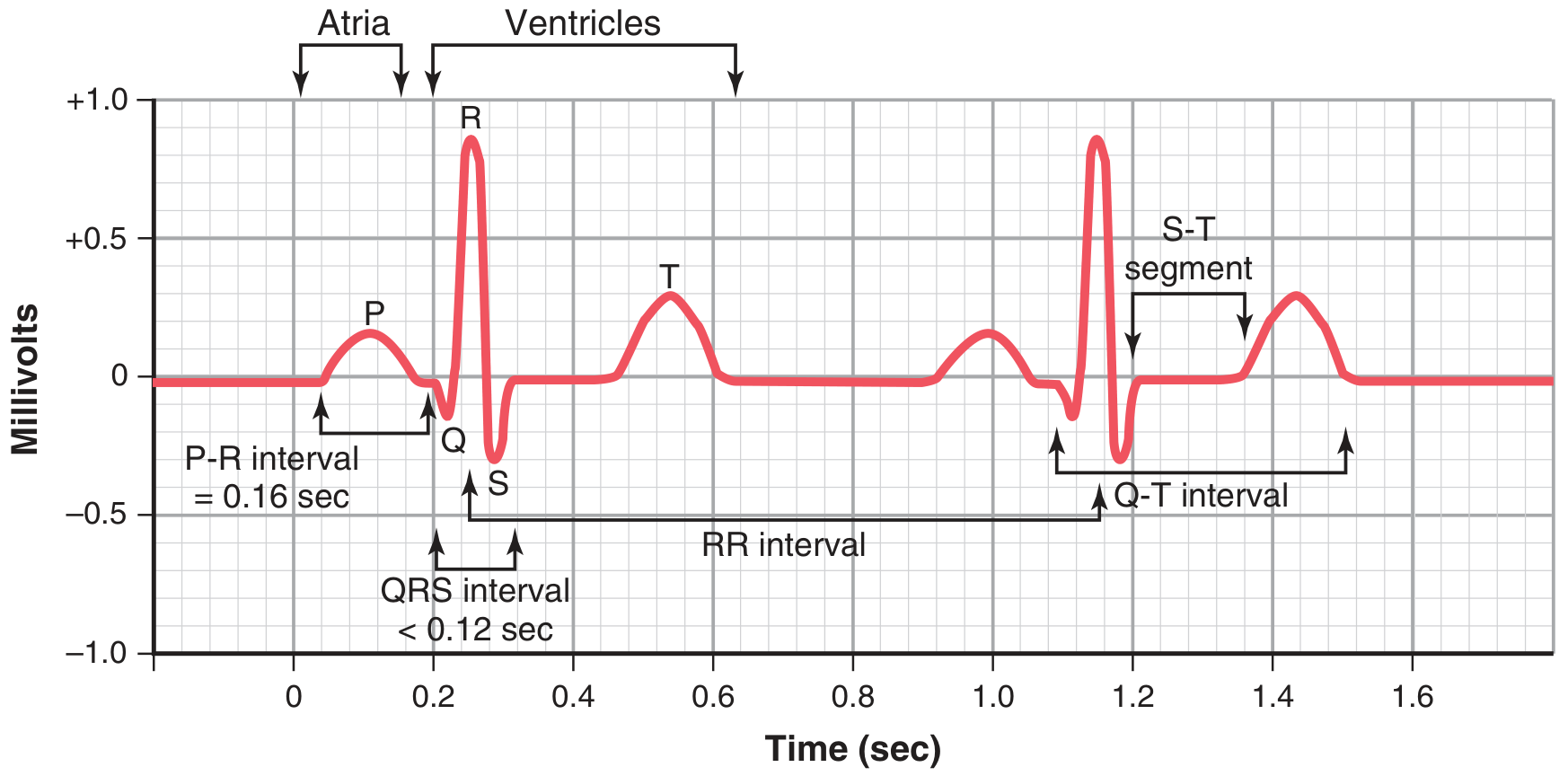
Figure 11.1, Guyton and Hall Textbook of Medical Physiology
2. Origin and Conduction of the Impulse
The electrical impulse originates at regular intervals in the sinoatrial (SA) node (usually 60-100 bpm). From there:
- SA node fires spontaneously (automaticity via slow phase 4 depolarization)
- Impulse spreads rapidly through the atria via internodal pathways
- Enters the atrioventricular (AV) node - the only conduction pathway between atria and ventricles
- AV nodal delay: conduction takes ~0.15 seconds - this delay allows atrial contraction to propel blood into the ventricles before ventricular systole
- Impulse travels down the Bundle of His -> left and right bundle branches -> Purkinje fibers
- Activation starts at the endocardial surface near the apex and sweeps to the epicardial surface at the base
- Complete ventricular activation is achieved in <0.1 seconds, ensuring synchronous, hemodynamically effective contraction
- Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 357
3. Cardiac Action Potential Phases
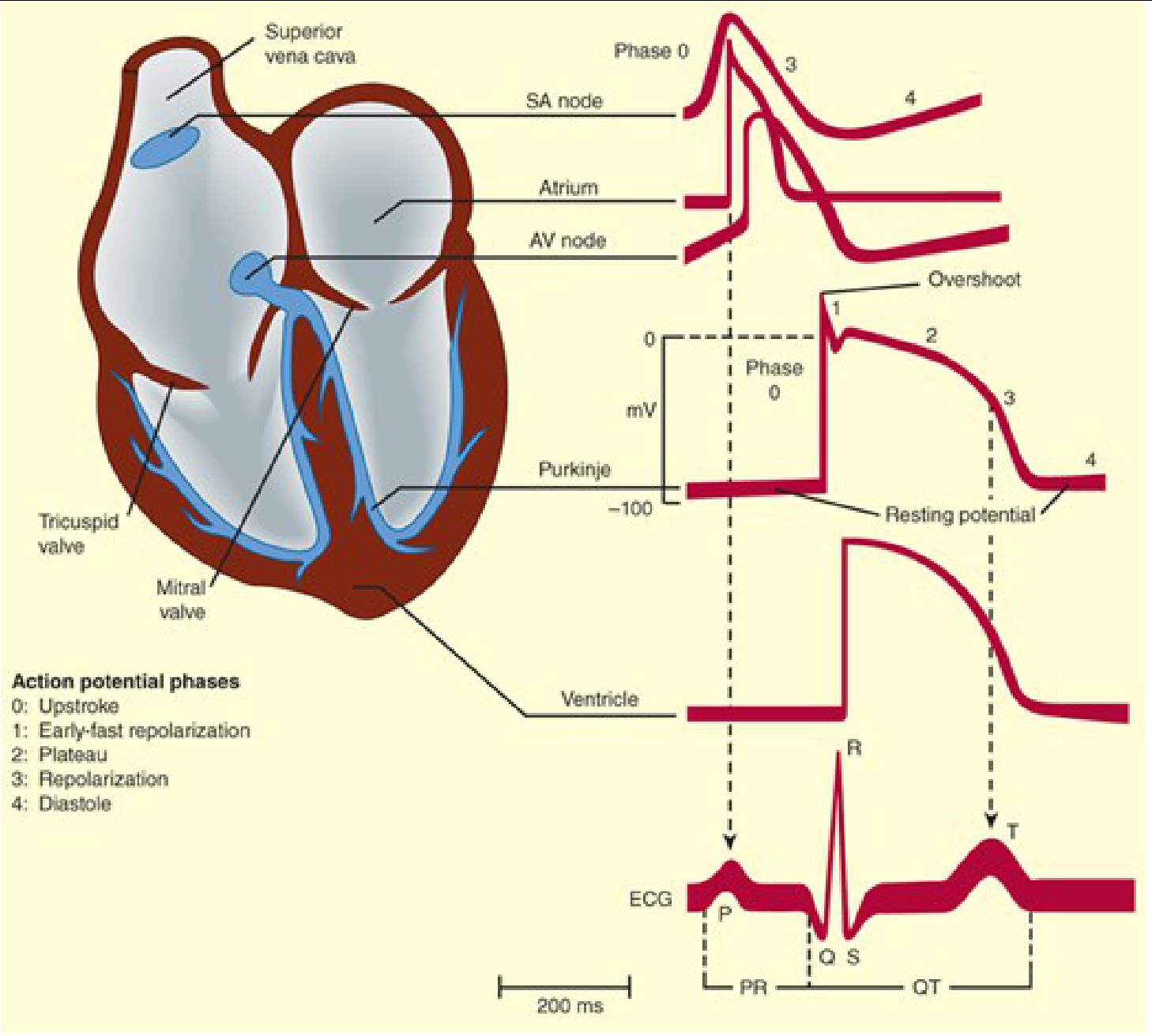
Katzung's Basic and Clinical Pharmacology, 16th Edition
Ventricular Action Potential (5 Phases)
The resting membrane potential of ventricular myocytes is approximately -90 mV.
| Phase | Name | Ionic Mechanism |
|---|---|---|
| Phase 0 | Rapid depolarization (upstroke) | Opening of voltage-gated Na+ channels - fast inward Na+ current; membrane rapidly depolarizes to +20 to +30 mV (overshoot) |
| Phase 1 | Early rapid repolarization | Closure of Na+ channels + opening of transient K+ channels (Kv4.2, Kv4.3, Kv1.4) - brief initial repolarization |
| Phase 2 | Plateau | Balanced inward L-type Ca2+ current and outward K+ current maintain near-zero potential; lasts ~200 ms; triggers excitation-contraction coupling |
| Phase 3 | Late rapid repolarization | Closure of Ca2+ channels + delayed increase of K+ efflux through multiple K+ channels; membrane returns to resting potential |
| Phase 4 | Resting potential / Spontaneous depolarization | In working myocytes: stable at -90 mV. In pacemaker cells (SA node, AV node, Purkinje): slow spontaneous depolarization due to "funny current" (If) - gradual return to threshold |
- Ganong's Review of Medical Physiology, 26th Edition
SA/AV Node (Slow-Response) Action Potential
SA and AV nodal cells differ from working myocytes:
- Resting potential is less negative (~-55 to -65 mV)
- Upstroke (Phase 0) depends on Ca2+ channels (not Na+), making it slower and less steep
- Phase 4 is not stable - spontaneous drift toward threshold (automaticity) driven by If ("pacemaker current"), ICa,T, and declining IK
- This automaticity is why the SA node naturally fires at 60-100 bpm; AV node at 40-60 bpm; Purkinje at 20-40 bpm (hierarchy of automaticity)
4. ECG Waves and Their Electrical Correlates
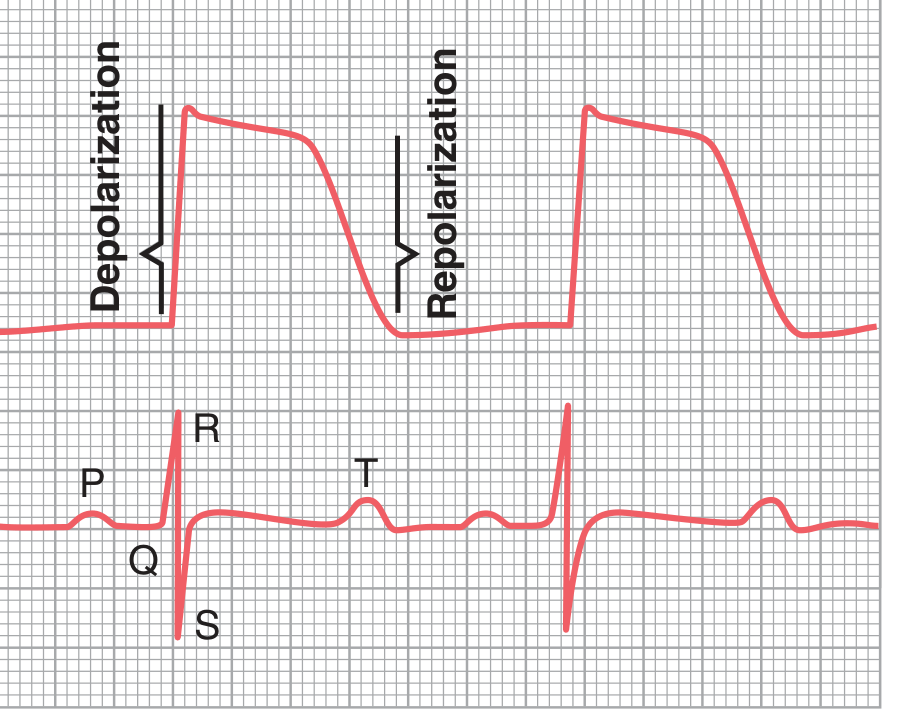
Figure 11.3, Guyton and Hall - Action potential (top) correlated with simultaneous ECG (bottom)
| ECG Feature | Electrical Event | Normal Duration/Amplitude |
|---|---|---|
| P wave | Atrial depolarization | 0.08-0.1 sec; 0.1-0.3 mV |
| PR interval | Atrial depolarization + AV nodal conduction delay | 0.12-0.20 sec |
| QRS complex | Ventricular depolarization | <0.12 sec; 1.0-1.5 mV |
| ST segment | Ventricular fully depolarized (plateau phase) | Isoelectric (no current flow when all cells are equally depolarized) |
| T wave | Ventricular repolarization | ~0.15 sec wide; 0.2-0.3 mV |
| QT interval | Duration of entire ventricular action potential | ~0.35-0.43 sec (rate-dependent) |
| U wave | Possibly late repolarization of Purkinje system / M cells | Small, follows T wave; more prominent at low heart rates or in hypokalemia |
- Guyton and Hall Textbook of Medical Physiology
- Katzung's Basic and Clinical Pharmacology, 16th Edition
5. Key Principle: Why the ECG Records Deflections
The ECG only records voltage when the heart muscle is partially polarized and partially depolarized - i.e., when current flows between different regions. When the muscle is either completely polarized (phase 4) or completely depolarized (phase 2/plateau), no current flows to the body surface and the ECG returns to baseline (isoelectric). This is why:
-
The PR segment is isoelectric (atria fully depolarized, AV node conducting)
-
The ST segment is isoelectric (ventricles fully depolarized at plateau)
-
Guyton and Hall Textbook of Medical Physiology, p. 143
6. Relationship to Mechanical Events
| Electrical Event | Mechanical Consequence |
|---|---|
| P wave | Atrial contraction begins |
| QRS complex | Ventricular contraction begins |
| ST segment | Ventricular contraction continues (systole) |
| T wave | Ventricular repolarization; relaxation begins |
| After T wave | Ventricular diastole (filling) |
The ventricles remain contracted until after the T wave ends, because repolarization must occur before relaxation is possible.
7. Refractory Periods
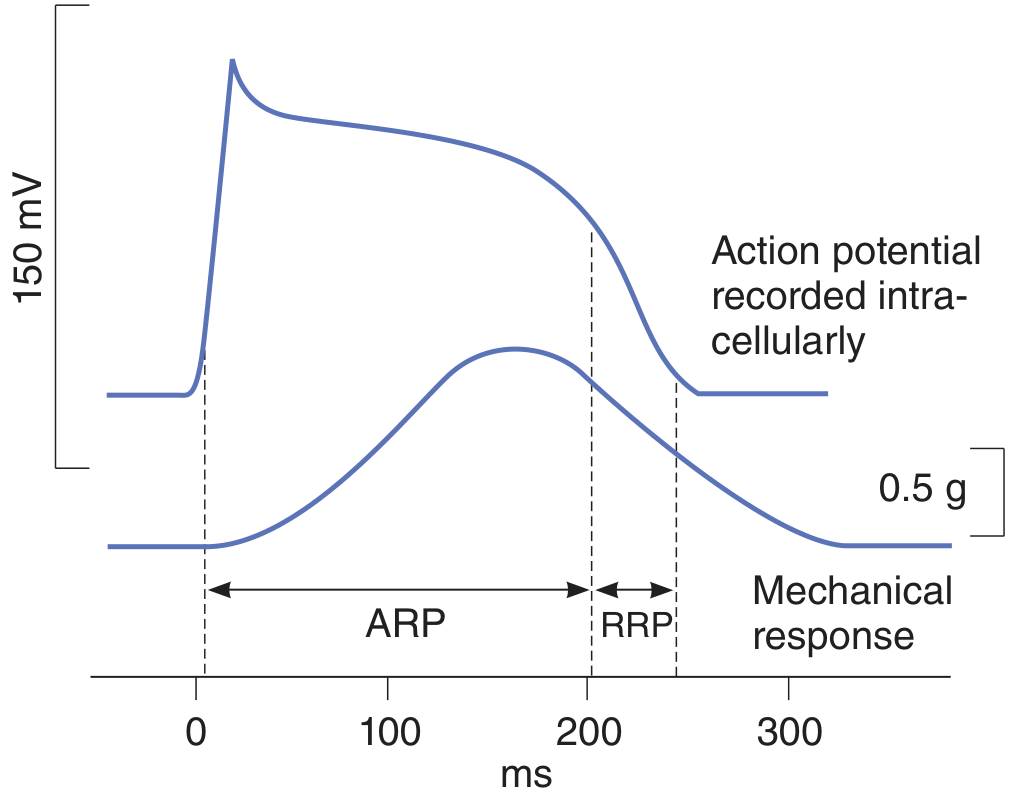
Ganong's Review of Medical Physiology, 26th Edition
- Absolute Refractory Period (ARP): corresponds to phases 0-2 (~0-200 ms); no stimulus can trigger another action potential regardless of strength - prevents tetanic contraction of cardiac muscle (critical for heart function)
- Relative Refractory Period (RRP): corresponds to phase 3 (~200-250 ms); only a supranormal stimulus can trigger an action potential; the cell is vulnerable to arrhythmias here ("R-on-T phenomenon")
The long refractory period, which coincides with the long plateau phase, is one of the most important protective features of cardiac physiology - it prevents summation and ensures each beat is followed by adequate diastolic filling.
Sources:
- Guyton and Hall Textbook of Medical Physiology - Chapters 10-11
- Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter 14
- Ganong's Review of Medical Physiology, 26th Edition - Chapter 5
- Medical Physiology (Boron & Boulpaep) - Chapter 22
This is a shared conversation. Sign in to Orris to start your own chat.