Tubercular otitis media in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
tubercular otitis media tuberculosis ear clinical features diagnosis management
search_medical_text
tuberculous otitis media pathology bacteriology complications treatment antitubercular therapy
search_medical_image
tubercular otitis media ear drum perforation pale mucosa
GradeResponse
GradeResponse
GradeResponse
search_medical_text
tuberculosis middle ear otitis media CSOM chronic suppurative pathogenesis spread
search_medical_text
tuberculous otitis media multiple perforations facial nerve palsy histology granuloma diagnosis PCR
search_medical_image
tuberculous otitis media histopathology granuloma Langhans giant cells caseation
GradeResponse
I now have all the material needed for a comprehensive, examination-ready answer. Let me compile the full 50-mark essay.
TUBERCULAR OTITIS MEDIA (TOM)
A Comprehensive 50-Mark Answer
As per RGUHS Syllabus | References: Scott-Brown, Cummings, Stell & Maran, Zakir Hussain, Dhingra, Hazarika + Recent Advances
OUTLINE
- Introduction & Historical Background
- Incidence & Epidemiology
- Etiopathogenesis
- Routes of Infection
- Pathology & Histopathology
- Clinical Features (Cardinal Features)
- Investigations & Diagnosis
- Differential Diagnosis
- Complications
- Treatment (Medical + Surgical)
- Recent Advances
- Flowcharts & Diagrams
- Summary Table
1. INTRODUCTION
Tubercular Otitis Media (TOM) is a chronic, specific granulomatous infection of the middle ear and mastoid cleft caused by Mycobacterium tuberculosis. It is one of the oldest and most deceptive forms of otitis media — presenting insidiously, mimicking chronic suppurative otitis media (CSOM), and often diagnosed only on histopathology.
"Tuberculosis of the ear is one of the most deceptive of all diseases of the temporal bone, presenting with features indistinguishable from CSOM." — Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (7th ed.)
TOM accounts for 0.04–0.9% of all cases of chronic otitis media in developed countries, but in endemic regions like India, it remains a significant clinical entity. With the resurgence of tuberculosis due to HIV co-infection and multidrug-resistant (MDR-TB) strains, the incidence of TOM is rising globally.
2. EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Incidence (Global) | 0.04–0.9% of CSOM cases |
| Incidence (India) | Higher; exact data under-reported |
| Age | Any age; more common in children (primary) and adults (secondary) |
| Sex | Males slightly more affected |
| Associated factors | HIV/AIDS, immunosuppression, poverty, malnutrition, pulmonary TB |
| Side | Usually unilateral; bilateral in miliary TB |
(Dhingra PL, Diseases of Ear, Nose and Throat, 7th ed.; Hazarika P, Textbook of ENT and HNS)
3. ETIOPATHOGENESIS
Causative Organism
- Mycobacterium tuberculosis (primary cause) — an obligate aerobe, acid-fast bacillus (AFB), Gram-positive cell wall
- M. bovis — via contaminated unpasteurized milk (rare today)
- Atypical mycobacteria — in immunocompromised patients
Pathogenesis
M. tuberculosis reaches the middle ear → engulfed by macrophages → failure of intracellular killing → granuloma formation → caseation necrosis → spread to mastoid, ossicles, labyrinth, facial nerve canal.
┌─────────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF TOM │
│ │
│ M. tuberculosis bacilli enter middle ear │
│ ↓ │
│ Phagocytosed by alveolar macrophages/monocytes │
│ ↓ │
│ Intracellular survival (escape phagolysosomal killing) │
│ ↓ │
│ T-lymphocyte sensitization → CMI response │
│ ↓ │
│ Granuloma formation (Epithelioid cells + Langhans GC) │
│ ↓ │
│ Central Caseation Necrosis │
│ ↓ │
│ Spread → Mastoid → Ossicles → Labyrinth → Facial N. │
│ ↓ │
│ Bone destruction → Fibrosis → Sequestrum formation │
└─────────────────────────────────────────────────────────────┘
4. ROUTES OF INFECTION
Primary Routes (Scott-Brown, Vol 3 / Stell & Maran):
┌──────────────────────────────────────────────────────────────┐
│ ROUTES OF INFECTION IN TOM │
│ │
│ 1. HAEMATOGENOUS (Most Common in Children) │
│ Primary pulmonary TB → Bacteremia → Middle ear │
│ │
│ 2. EUSTACHIAN TUBE (Most Common overall / Adults) │
│ Nasopharyngeal TB → Ascending via ET → Middle ear │
│ (Especially in primary nasopharyngeal TB) │
│ │
│ 3. EXTERNAL AUDITORY CANAL (Rare) │
│ Direct inoculation through perforated TM │
│ │
│ 4. LYMPHATIC SPREAD │
│ Cervical lymph nodes → Retropharyngeal → ET → ME │
│ │
│ 5. DIRECT EXTENSION │
│ TB mastoiditis → Middle ear │
│ TB of petrous apex → Labyrinthitis │
└──────────────────────────────────────────────────────────────┘
(Zakir Hussain, Clinical ENT; Cummings Otolaryngology HNS, 7th ed.)
5. PATHOLOGY & HISTOPATHOLOGY
Macroscopic Features
- Pale, oedematous middle ear mucosa (vs. red/hyperaemic in CSOM)
- Multiple perforations of tympanic membrane — pathognomonic
- Central, large, or subtotal perforation common
- Caseous yellowish-white material in middle ear
- Granulation tissue — pale, avascular
- Bone erosion — mastoid, ossicles, labyrinth
- Sequestra of necrotic bone
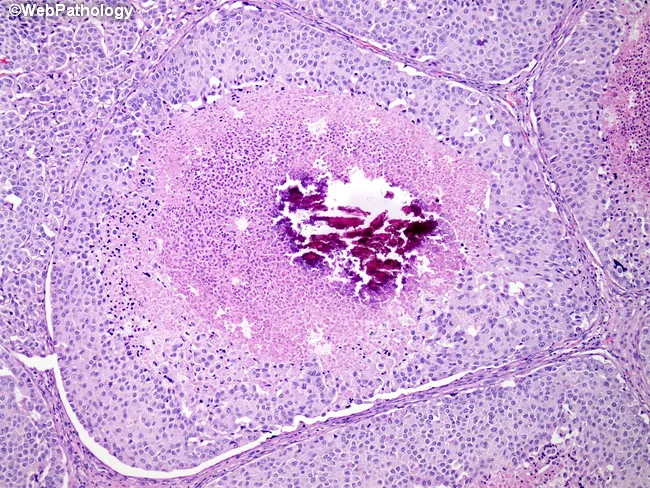
Microscopic / Histopathological Features
(Hallmark — diagnosed on biopsy)
| Feature | Finding |
|---|---|
| Granuloma | Epithelioid cell granuloma — pathognomonic |
| Giant cells | Langhans-type multinucleated giant cells |
| Caseation | Central caseous necrosis |
| Lymphocytic cuffing | Peripheral lymphocytes around granuloma |
| Fibrous capsule | Surrounding thin fibrous rim |
| AFB | Ziehl-Neelsen stain: acid-fast bacilli (may be sparse) |
| Vascular supply | Poor — avascular granulation |
Histopathology Image:
6. CLINICAL FEATURES
Cardinal Features of TOM
"The hallmarks of TOM are multiple perforations, painless otorrhoea, early and severe conductive hearing loss, early facial nerve palsy, and pale avascular granulations." — Dhingra PL, Diseases of Ear, Nose and Throat
A. Symptoms
| Symptom | Characteristics |
|---|---|
| Otorrhoea | Painless, scanty, watery/serous (not purulent), persistent, non-malodorous initially |
| Hearing Loss | Early, severe conductive loss; may have SNHL in advanced disease |
| Otalgia | Usually absent (painless — key feature) |
| Tinnitus | May be present in labyrinthine involvement |
| Vertigo | Labyrinthine fistula or TB labyrinthitis |
| Facial weakness | Early facial palsy — 17–40% cases (unique to TOM) |
B. Signs (Otoscopic Findings)
┌─────────────────────────────────────────────────────────────────┐
│ OTOSCOPIC FINDINGS IN TOM │
│ │
│ • MULTIPLE perforations (2–4) of pars tensa — PATHOGNOMONIC │
│ • Perforations later coalesce → LARGE CENTRAL / SUBTOTAL TM │
│ • PALE, AVASCULAR granulations in middle ear │
│ • Discharge: THIN, WATERY, ODOURLESS │
│ • PALE, OEDEMATOUS mucosa (not hyperaemic as in CSOM) │
│ • ABSENT light reflex; dull, thickened TM margins │
│ • Ossicular destruction (late) │
│ │
│ KEY DIFFERENTIATING POINT: │
│ CSOM → Red, granular, mucopurulent, foul-smelling │
│ TOM → Pale, watery, odourless, multiple perforations │
└─────────────────────────────────────────────────────────────────┘
Otoscopic Image:

C. Systemic Features
- Fever (low-grade, evening rise)
- Night sweats, weight loss, malaise
- Cervical lymphadenopathy (scrofula)
- Features of pulmonary TB (cough, hemoptysis)
- May present without systemic TB — isolated TOM
7. INVESTIGATIONS & DIAGNOSIS
Diagnostic Flowchart
┌──────────────────────────────────────────────────────────────────┐
│ DIAGNOSTIC ALGORITHM FOR TOM │
│ │
│ CLINICAL SUSPICION │
│ (CSOM not responding to standard treatment + │
│ Multiple perforations + Pale granulations + │
│ Early facial nerve palsy) │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ INITIAL INVESTIGATIONS │ │
│ │ • Ear swab - AFB smear & C/S │ │
│ │ • Chest X-ray (PA view) │ │
│ │ • Mantoux/Tuberculin test │ │
│ │ • ESR, CBC, CRP │ │
│ │ • PTA (Pure Tone Audiometry) │ │
│ └────────────────────┬────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ CONFIRMATORY INVESTIGATIONS │ │
│ │ • BIOPSY of granulation tissue (GOLD STANDARD) │ │
│ │ → H&E: Caseating granuloma + Langhans GC │ │
│ │ → ZN stain: AFB │ │
│ │ • Culture on Lowenstein-Jensen medium (6-8 wks) │ │
│ │ • PCR (IS6110 gene) — rapid, sensitive │ │
│ │ • IGRA (Interferon Gamma Release Assay) │ │
│ └────────────────────┬────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ IMAGING │ │
│ │ • HRCT Temporal Bone: │ │
│ │ - Soft tissue in mastoid/ME │ │
│ │ - Bone destruction pattern (diffuse, lytic) │ │
│ │ - Sequestrum │ │
│ │ - Labyrinthine erosion │ │
│ │ - Facial nerve canal involvement │ │
│ │ • MRI: Abscess, meningeal involvement │ │
│ └─────────────────────────────────────────────────────┘ │
└──────────────────────────────────────────────────────────────────┘
Investigations in Detail
| Investigation | Findings in TOM |
|---|---|
| Ear swab AFB smear | Low yield (AFB sparse in ME secretions) |
| Culture (L-J medium) | Gold standard for bacteriology; takes 6–8 weeks |
| Mantoux test | Positive (>10 mm induration); negative in immunocompromised |
| IGRA (QuantiFERON-TB Gold) | More specific than Mantoux; unaffected by BCG |
| Chest X-ray | Pulmonary TB in 30–50%; may be normal |
| HRCT Temporal Bone | Bony erosion, soft tissue density, sequestrum, labyrinthine fistula |
| Biopsy (H&E + ZN) | Definitive diagnosis — caseating granuloma + Langhans GCs |
| PCR (IS6110) | Rapid, sensitive (>90%), specific; detects MDR strains |
| PTA | CHL / mixed / SNHL depending on extent |
| ESR, CRP | Raised non-specifically |
| HIV serology | Mandatory in all TOM cases |
(Scott-Brown 7th ed., Vol 3; Cummings 7th ed., Ch 137; Hazarika P, HNS)
8. DIFFERENTIAL DIAGNOSIS
| Feature | TOM | CSOM (Mucosal) | CSOM (Squamosal) | Wegener's | Syphilitic OM |
|---|---|---|---|---|---|
| Perforations | Multiple | Central single | Attic/marginal | Variable | Variable |
| Discharge | Watery, odourless | Mucopurulent | Foul, scanty | Variable | Variable |
| Granulations | Pale, avascular | Red, vascular | — | Ulcerative | — |
| Facial palsy | Early (17–40%) | Late/rare | Present | Rare | Rare |
| Bone erosion | Diffuse lytic | — | Localised | Diffuse | — |
| Histology | Caseating granuloma | Chronic inflammation | Cholesteatoma | Non-caseating granuloma | Spirochetes |
| Response to ABx | Poor | Good | Poor | Steroids | Penicillin |
9. COMPLICATIONS
Flowchart of Complications
┌──────────────────────────────────────────────────────────────────┐
│ COMPLICATIONS OF TOM │
│ │
│ TUBERCULAR OTITIS MEDIA │
│ ↓ │
│ ┌───────────────────┼───────────────────┐ │
│ ↓ ↓ ↓ │
│ INTRATEMPORAL INTRACRANIAL SYSTEMIC │
│ COMPLICATIONS COMPLICATIONS COMPLICATIONS │
│ │ │ │ │
│ • Facial nerve • Meningitis • Miliary TB │
│ palsy (17-40%) • Brain abscess • Dissemination │
│ • Labyrinthitis • Sigmoid sinus • Vertebral TB │
│ • Labyrinthine thrombosis (Pott's) │
│ fistula • Extradural • TB lymphadenitis │
│ • Mastoiditis abscess • Hepatic TB │
│ • Petrositis • Subdural • Renal TB │
│ • Subperiosteal empyema │
│ abscess • Lateral sinus │
│ • Ossicular thrombophlebitis │
│ necrosis │
│ • SNHL │
│ • Tympanosclerosis │
└──────────────────────────────────────────────────────────────────┘
Important Notes on Complications:
- Facial nerve palsy is the most characteristic complication — occurs early, may be the presenting feature, and may resolve completely with ATT (Zakir Hussain, Clinical ENT)
- Labyrinthitis — presents as sudden SNHL + vertigo; indicates spread to inner ear
- Intracranial complications — rare but serious; mortality high
- Petrous apex involvement — Gradenigo's syndrome (TOM + VI nerve palsy + retro-orbital pain)
10. TREATMENT
Treatment Flowchart
┌──────────────────────────────────────────────────────────────────┐
│ TREATMENT ALGORITHM FOR TOM │
│ │
│ CONFIRMED TOM DIAGNOSIS │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ MEDICAL TREATMENT (MAINSTAY) │ │
│ │ │ │
│ │ INTENSIVE PHASE (2 months): │ │
│ │ HRZE = Isoniazid + Rifampicin + │ │
│ │ Pyrazinamide + Ethambutol │ │
│ │ │ │
│ │ CONTINUATION PHASE (4 months): │ │
│ │ HR = Isoniazid + Rifampicin │ │
│ │ (Total: 6 months standard; 9-12 months if │ │
│ │ complications/meningitis/MDR) │ │
│ └────────────────────┬────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ ADJUVANT THERAPY │ │
│ │ • Pyridoxine 10 mg/day (INH neuropathy prevention) │ │
│ │ • Corticosteroids (controversial — see below) │ │
│ │ • Aural toilet + local care │ │
│ └────────────────────┬────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ ASSESS RESPONSE AT 2 MONTHS │ │
│ │ Good response → Continue HR x 4 months │ │
│ │ Poor/MDR → Culture sensitivity + DST │ │
│ │ MDR regimen: Bedaquiline + Linezolid + │ │
│ │ Pretomanid (BPaL) or individualised │ │
│ └────────────────────┬────────────────────────────────┘ │
│ ↓ │
│ ┌─────────────────────────────────────────────────────┐ │
│ │ SURGICAL TREATMENT │ │
│ │ (After completing ATT / for residual disease) │ │
│ │ │ │
│ │ 1. MASTOIDECTOMY (Cortical/Modified Radical) │ │
│ │ — Remove sequestra, caseous material │ │
│ │ — If intratemporal complication │ │
│ │ │ │
│ │ 2. TYMPANOPLASTY │ │
│ │ — After ATT completion (>12 months quiescence) │ │
│ │ — Repair TM perforation │ │
│ │ — Ossiculoplasty if ossicular destruction │ │
│ │ │ │
│ │ 3. FACIAL NERVE DECOMPRESSION │ │
│ │ — If FNP persists after 6 weeks ATT │ │
│ │ — If worsening on ATT │ │
│ │ │ │
│ │ 4. COCHLEAR IMPLANT │ │
│ │ — If profound SNHL after ATT │ │
│ └─────────────────────────────────────────────────────┘ │
└──────────────────────────────────────────────────────────────────┘
Anti-Tubercular Drug Dosages
| Drug | Abbreviation | Dose (Adult) | Dose (Child) | Key Side Effect |
|---|---|---|---|---|
| Isoniazid | H | 5 mg/kg (max 300 mg/day) | 10 mg/kg | Hepatotoxicity, peripheral neuropathy |
| Rifampicin | R | 10 mg/kg (max 600 mg/day) | 15 mg/kg | Hepatotoxicity, orange discolouration |
| Pyrazinamide | Z | 25 mg/kg (max 2g/day) | 35 mg/kg | Hepatotoxicity, hyperuricaemia |
| Ethambutol | E | 15 mg/kg/day | 20 mg/kg | Optic neuritis, colour vision loss |
| Pyridoxine | B6 | 10–25 mg/day | — | Prevents INH neuropathy |
(Harrison's Principles of Internal Medicine, 21st ed., p.4179; Cummings, Ch.137)
Corticosteroids in TOM
- Role: Reduce inflammatory oedema, may aid facial nerve recovery
- Indication: Facial nerve palsy, labyrinthitis, severe oedema
- Regimen: Prednisolone 1 mg/kg/day tapering over 4–6 weeks alongside ATT
- Controversial: No RCT data; used empirically (Scott-Brown, 7th ed.)
Aural Toilet
- Daily suction clearance of middle ear discharge
- Antiseptic ear drops (Ciprofloxacin ear drops) for secondary infections
- Avoid water entry (ear plugs)
11. RECENT ADVANCES
A. Molecular Diagnostics
- Xpert MTB/RIF (GeneXpert): Rapid PCR-based detection in <2 hours; simultaneously detects rifampicin resistance; sensitivity ~88%, specificity ~98% for ear granulation tissue (Blevins et al., 2020)
- Whole Genome Sequencing (WGS): Identifies exact strain, full drug susceptibility pattern; gold standard for MDR-TB diagnosis
- Loop-Mediated Isothermal Amplification (LAMP): Point-of-care test, no sophisticated equipment; useful in low-resource settings
B. MDR-TB & New Drug Regimens
- Bedaquiline (B): Diarylquinoline — ATP synthase inhibitor; first new class in 40 years
- Pretomanid (Pa): Nitroimidazole; approved for XDR-TB
- Linezolid (L): Oxazolidinone; active against MDR strains
- BPaL Regimen (Bedaquiline + Pretomanid + Linezolid): 6-month regimen for XDR-TB — WHO 2022 guidelines
- Delamanid: Approved for MDR-TB in children
C. Imaging Advances
- HRCT Temporal Bone with 3D reconstruction: Better delineation of ossicular chain, facial nerve canal, labyrinthine fistula (Radiographics 2021)
- Diffusion-Weighted MRI (DW-MRI): Distinguishes tuberculoma from abscess/cholesteatoma
- PET-CT: For staging systemic TB involvement, treatment monitoring
D. Surgical Advances
- Endoscopic Ear Surgery (EES): Transcanal endoscopic approach for middle ear exploration and biopsy with minimal morbidity
- Cochlear Implantation post-TOM: Successful outcomes reported even with cochlear fibrosis if done after ATT completion (Ear Hear 2022)
- Osseointegrated Bone Conduction Devices (BAHA): For mixed/conductive HL when reconstruction not feasible
E. Immunotherapy
- Adjunctive Immunotherapy: Vitamin D supplementation reduces time to sputum conversion; IL-2 therapy under trial
- TB Vaccine (M72/AS01E): Phase 2b results show 50% efficacy against active TB in latent-infected adults (NEJM 2019)
F. RGUHS-Specific Recent Advances to Note
- WHO 2022 Updated Treatment Guidelines: 6-month HRZE/HR still standard; BPaL for XDR
- National TB Elimination Programme (NTEP) — India's revised PMDT (Programmatic Management of Drug-Resistant TB) guidelines 2021
- NIKSHAY portal — digital TB notification system; all TOM cases must be notified
- 4-month regimen trial (TBTC S31/ACTG A5349): Rifapentine + Moxifloxacin — non-inferior to 6-month for drug-susceptible TB (NEJM 2021)
12. COMPREHENSIVE FLOWCHART: TOM AT A GLANCE
┌─────────────────────────────────────────────────────────────────────┐
│ TUBERCULAR OTITIS MEDIA │
│ COMPLETE OVERVIEW │
│ │
│ AETIOLOGY │
│ M. tuberculosis → AFB, aerobe, slow-growing │
│ ↓ │
│ ROUTES: ET (adults) → Haematogenous (children) → │
│ EAC (direct) → Lymphatic │
│ ↓ │
│ PATHOLOGY │
│ Granuloma → Caseation → Necrosis → Bone erosion │
│ ↓ │
│ CLINICAL FEATURES │
│ ┌────────────────────────────────────────────────┐ │
│ │ Painless watery otorrhoea │ │
│ │ + Multiple TM perforations (PATHOGNOMONIC) │ │
│ │ + Pale avascular granulations │ │
│ │ + Early Facial Nerve Palsy (17-40%) │ │
│ │ + Severe CHL disproportionate to signs │ │
│ │ + CSOM not responding to antibiotics │ │
│ └────────────────────────────────────────────────┘ │
│ ↓ │
│ INVESTIGATIONS │
│ Biopsy (H&E+ZN) → PCR → Culture → HRCT → IGRA │
│ ↓ │
│ TREATMENT │
│ 2HRZE + 4HR (6 months standard) │
│ Surgery: Mastoidectomy + Tympanoplasty (after ATT) │
│ ↓ │
│ COMPLICATIONS │
│ FNP → Labyrinthitis → Mastoiditis → Intracranial │
│ ↓ │
│ PROGNOSIS │
│ Good with early diagnosis + complete ATT │
│ FNP usually recovers; SNHL may be permanent │
└─────────────────────────────────────────────────────────────────────┘
13. SUMMARY TABLE: KEY FACTS FOR RGUHS EXAM
| Topic | Key Points |
|---|---|
| Causative organism | M. tuberculosis (AFB); M. bovis rare |
| Most common route | Eustachian tube (adults); Haematogenous (children) |
| Pathognomonic feature | Multiple perforations of TM |
| Cardinal symptom | Painless, watery, odourless otorrhoea |
| Characteristic complication | Early facial nerve palsy (17–40%) |
| Gold standard diagnosis | Biopsy — caseating granuloma + Langhans GCs on H&E |
| Rapid molecular test | GeneXpert MTB/RIF (PCR) |
| Imaging of choice | HRCT Temporal Bone |
| Treatment | 2HRZE + 4HR (RNTCP/NTEP protocol) |
| Surgery timing | After ATT; tympanoplasty only after >12 months of quiescence |
| Surgery for FNP | Decompress if no improvement at 6 weeks on ATT |
| Prognosis | Good if early; SNHL may be permanent |
| Notifiable disease | Yes — NIKSHAY portal (NTEP India) |
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 7th Edition — Gleeson et al.; Vol 3, Chapter on Specific Infections of the Ear
- Cummings Otolaryngology Head & Neck Surgery, 7th Edition — Flint et al.; Chapter 137 — Chronic Otitis Media
- Stell & Maran's Textbook of Head and Neck Surgery and Oncology, 5th Edition — Watkinson JC et al.
- Zakir Hussain, Clinical ENT — Chapter on Specific Otitis Media
- Dhingra PL & Dhingra S, Diseases of Ear, Nose and Throat and Head & Neck Surgery, 7th Edition — Chapter on Tuberculosis of Ear
- Hazarika P, Nayak DR, Balakrishnan R, Textbook of ENT and Head & Neck Surgery — Clinical Companion, 3rd Edition
- Harrison's Principles of Internal Medicine, 21st Edition — Chapter on Mycobacterial Diseases (pp. 4179)
- WHO Global Tuberculosis Report 2022 — Updated treatment guidelines; BPaL regimen
- RNTCP/NTEP India, Programmatic Management of Drug-Resistant TB Guidelines, 2021
- Blevins SM et al. (2020) — Xpert MTB/RIF in temporal bone TB
- Slattery WH, Brackmann DE — Otologic manifestations of tuberculosis (Otolaryngol HNS)
- NEJM 2021 — 4-month TB regimen: TBTC S31/ACTG A5349 trial (Dorman et al.)
- NEJM 2019 — M72/AS01E vaccine efficacy (Van Der Meeren et al.)
Examiner's Note (RGUHS): TOM is a favourite 50-mark long essay question. Focus on: (1) Cardinal clinical features with pathognomonic multiple perforations, (2) Histopathology — granuloma with Langhans GCs, (3) Diagnostic algorithm with biopsy as gold standard and PCR as rapid test, (4) 2HRZE + 4HR regimen, (5) Surgery only after ATT completion, (6) Recent advances — GeneXpert, BPaL regimen, NTEP/NIKSHAY. Draw all flowcharts neatly. Mention facial palsy prominently.
This is a shared conversation. Sign in to Orris to start your own chat.