Top 10 heart diseases with ecg finding
Reading File
Finding Sources
Finding Sources
Searching Images
ECG findings heart diseases myocardial infarction atrial fibrillation
Finding Sources
Finding Sources
Finding Sources
Searching Images
STEMI ST elevation myocardial infarction ECG 12-lead
Finding Sources
Finding Sources
Finding Sources
Searching Images
atrial fibrillation ECG irregularly irregular absent P waves
Finding Sources
Finding Sources
Searching Images
hypertrophic cardiomyopathy ECG deep S waves LVH
I now have comprehensive data to compile the full answer. Let me present the top 10 heart diseases with their ECG findings:
Top 10 Heart Diseases & Their ECG Findings
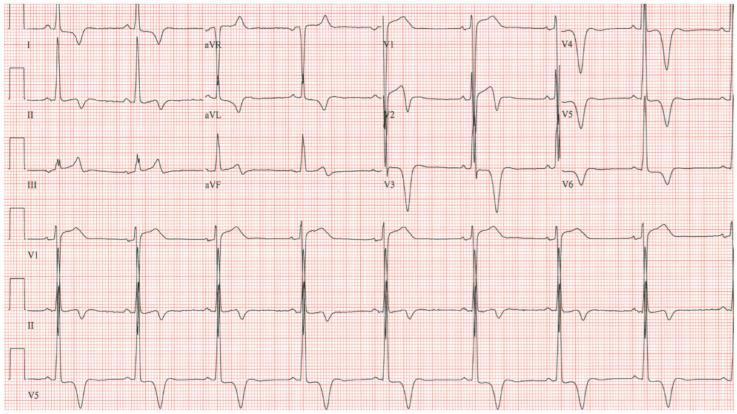
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Findings:
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex "tombstone" morphology)
- Hyperacute (peaked) T-waves — earliest change
- Pathological Q-waves — develop within hours (indicate transmural necrosis)
- Reciprocal ST-depression in opposite leads
- T-wave inversion in the evolving phase
Localisation by leads:
| Territory | ST Elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | V1–V2 depression + tall R | RCA/LCx |
Goldman-Cecil Medicine — "Acute MI is classified based on whether the ECG shows ST-segment elevation (STEMI) or not (NSTEMI)."
2. 💓 Atrial Fibrillation (AF)
ECG Findings:
- Absent P waves — replaced by chaotic fibrillatory (f) waves (best seen in V1)
- Irregularly irregular R-R intervals — hallmark finding
- Narrow QRS complexes (unless aberrant conduction)
- Rapid ventricular response (>100 bpm) if uncontrolled
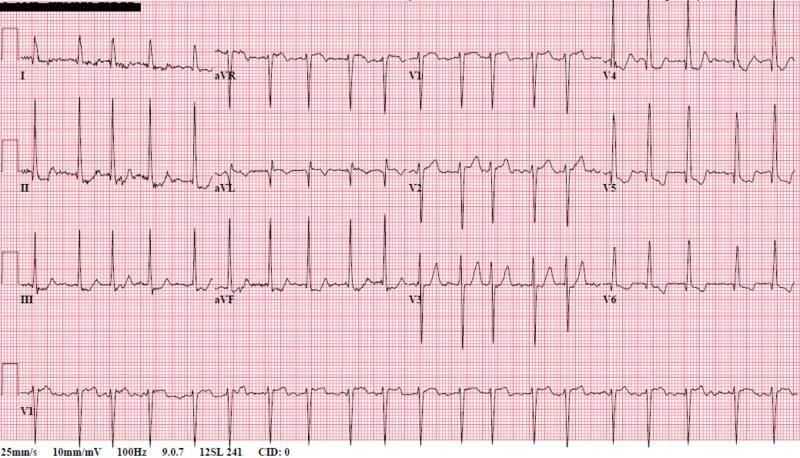
Braunwald's Heart Disease — "New atrial fibrillation or flutter" is a classic ECG manifestation of structural cardiac disease.
3. 🫁 Acute Pericarditis
ECG Findings (4 classic stages):
- Stage I: Diffuse concave ST elevation in nearly all leads (except aVR & V1) + PR depression (pathognomonic)
- Stage II: ST normalises, PR depression persists
- Stage III: T-wave inversions
- Stage IV: ECG normalises
Key differentiators from STEMI:
- ST elevation is diffuse (not regional)
- PR depression is present
- No reciprocal ST depression (except in aVR)
- No Q-waves
Washington Manual — "Classic ECG findings are diffuse ST-segment elevation with PR depression." Mulholland Surgery — "The EKG classically shows diffuse ST elevations without Q waves or T-wave inversion. PR depression can also be seen."
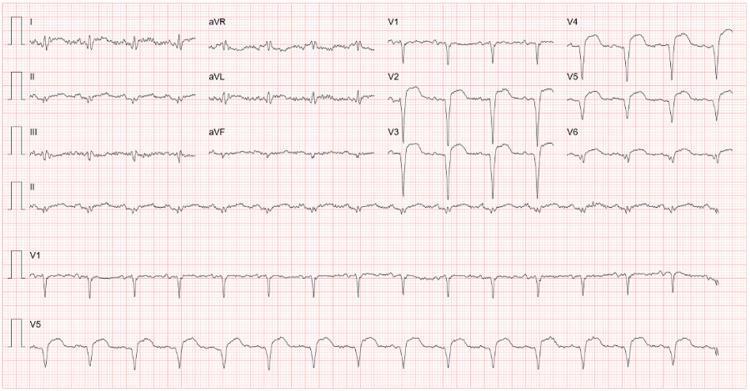
4. 💗 Hypertrophic Cardiomyopathy (HCM)
ECG Findings:
- Left ventricular hypertrophy (LVH) — Sokolow-Lyon criteria: deep S in V1 + tall R in V5 (sum >35 mm)
- Deep, broad Q-waves in lateral leads (I, aVL, V5–V6) — "septal Q-waves" (pseudoinfarction pattern)
- "Giant" symmetric T-wave inversions — especially in apical HCM (Yamaguchi syndrome) V3–V5 (up to 15 mm deep)
- Left axis deviation
- Atrial fibrillation common
Tintinalli's Emergency Medicine — "Deep S-wave voltage (28 mm S in V2) and deep broad Q-waves are characteristic HCM ECG findings."
5. 🔁 Wolff-Parkinson-White (WPW) Syndrome / Pre-Excitation
ECG Findings (classic triad):
- Short PR interval (<120 ms) — accessory pathway bypasses AV node delay
- Delta wave — slurred upstroke at the beginning of the QRS (pre-excitation of ventricles)
- Widened QRS (>120 ms) — due to fusion of normal and accessory conduction
- Pseudo-ST/T changes (secondary repolarisation abnormalities)
- Can mimic LBBB or RBBB patterns depending on pathway location
Washington Manual — "WPW syndrome: short PR and a delta wave on the upstroke of QRS. Can have AVRT (orthodromic or antidromic) as the mechanism of SVT." Miller's Anesthesia — "WPW: characterised by a shortened PR interval and a delta wave (i.e., early activation/"pre-excitation" of the His–Purkinje system)."
6. ❤️ Heart Failure with LV Hypertrophy / Hypertensive Heart Disease
ECG Findings:
- LVH voltage criteria (Sokolow-Lyon, Cornell criteria)
- LV strain pattern — ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
- Left atrial enlargement — broad, bifid P-wave (P-mitrale) in lead II; biphasic P in V1
- Left axis deviation
- LBBB in advanced disease
- Atrial fibrillation (from left atrial dilatation)
Robbins Pathology — "ECG or echocardiographic findings of left ventricular hypertrophy. The disease comes to attention with the onset of atrial fibrillation (secondary to left atrial enlargement)."
7. 📉 AV Heart Block (2nd & 3rd Degree)
ECG Findings:
| Type | ECG Pattern |
|---|---|
| 1st degree | PR interval >200 ms, all P waves conducted |
| Mobitz I (Wenckebach) | Progressive PR lengthening → dropped QRS; usually benign |
| Mobitz II | Constant PR, sudden dropped QRS; higher risk of progression |
| 3rd degree (complete) | P-waves and QRS are completely dissociated; escape rhythm (junctional 40–60 bpm or ventricular 20–40 bpm) |
Goldman-Cecil — "Complete heart block is usually preceded by abnormal baseline ECG findings, such as bundle branch block or second-degree AV block." Washington Manual — "Mobitz II 2nd-degree AV block carries a higher risk of progression to complete heart block than Mobitz I."
8. 🫀 Non-ST Elevation ACS (NSTEMI / Unstable Angina)
ECG Findings:
- ST depression ≥0.5–1 mm (horizontal or downsloping) in ≥2 contiguous leads
- T-wave inversions (deep, symmetric)
- Transient ST elevation that resolves
- ECG may be normal in ~20–30% of cases
- No pathological Q-waves (subendocardial infarction)
Goldman-Cecil — "MI is classified based on whether the ECG shows ST elevation (STEMI) or not (NSTEMI). NSTEMI shows no ST elevation but elevated biomarkers."
9. 🔴 Aortic Stenosis
ECG Findings:
- LVH — high voltage (pressure overload pattern)
- LV strain — ST-depression and T-wave inversion in V5–V6, I, aVL
- Left axis deviation
- Left atrial enlargement (P-mitrale)
- Left bundle branch block (advanced disease)
- Atrial fibrillation (late)
Tintinalli's — "ECG findings are generally nonspecific. The most common abnormality is left ventricular hypertrophy."
10. 🔶 Dilated Cardiomyopathy (DCM)
ECG Findings:
- Sinus tachycardia — compensatory
- Left bundle branch block (LBBB) — very common; QRS >120 ms, broad notched R in I/V5–V6
- LVH or low voltage (in end-stage)
- Pathological Q-waves — pseudoinfarction pattern (fibrosis)
- Left atrial enlargement
- Atrial fibrillation, ventricular ectopics, ventricular tachycardia
Quick Reference Summary Table
| # | Disease | Key ECG Sign |
|---|---|---|
| 1 | STEMI | ST elevation + Q-waves (regional) |
| 2 | Atrial Fibrillation | No P-waves + irregularly irregular |
| 3 | Acute Pericarditis | Diffuse concave ST elevation + PR depression |
| 4 | Hypertrophic Cardiomyopathy | LVH + giant T inversions + septal Q-waves |
| 5 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 6 | Hypertensive Heart Disease / HF | LVH + strain pattern + P-mitrale |
| 7 | AV Block (complete) | P-QRS dissociation + escape rhythm |
| 8 | NSTEMI / Unstable Angina | ST depression + T-wave inversions |
| 9 | Aortic Stenosis | LVH + LV strain |
| 10 | Dilated Cardiomyopathy | LBBB + low voltage + pseudoQ |
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine
- Goldman-Cecil Medicine
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Tintinalli's Emergency Medicine
- Washington Manual of Medical Therapeutics
- Robbins & Kumar Basic Pathology
- Miller's Anesthesia
This is a shared conversation. Sign in to Orris to start your own chat.