Vascular access in dialysis and it complications
Reading File
Finding Sources
Searching PubMed
"vascular access" AND "hemodialysis" AND complications
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
hemodialysis vascular access arteriovenous fistula graft types diagram
I now have comprehensive content to write a complete, detailed answer. Let me compile everything.
Vascular Access in Dialysis and Its Complications
Overview
Reliable vascular access is the lifeline of hemodialysis (HD). No single type of access fulfills all desired requirements, so the access strategy must be individualized based on patient anatomy, comorbidities, life expectancy, and the ESKD "Life Plan" concept introduced by the 2019 KDOQI guidelines.
The three major types of HD vascular access are:
- Arteriovenous fistula (AVF)
- Arteriovenous graft (AVG)
- Tunneled central venous catheter (TDC)
1. Types of Vascular Access
1.1 Arteriovenous Fistula (AVF)
The AVF — introduced by Brescia and colleagues in 1966 — remains the preferred access. It is entirely subcutaneous, preserves arterial flow to the hand, and has the best long-term patency with fewest complications.
Preferred hierarchy (distal-to-proximal, following KDOQI):
| Priority | Type | Details |
|---|---|---|
| 1st | Radiocephalic (Brescia-Cimino) | Radial artery → cephalic vein at wrist |
| 2nd | Forearm basilic AVF | Radial or ulnar artery → basilic vein |
| 3rd | Brachiocephalic (upper arm) | Brachial artery → cephalic vein |
| 4th | Brachiobasilic (requires transposition) | Brachial artery → transposed basilic vein |
Pre-operative assessment:
- Arterial: triphasic waveform, equal bilateral BPs; brachial artery ≥3 mm, radial/ulnar ≥2 mm
- Venous: cephalic or basilic vein ≥2 mm diameter, depth ≤6 mm
- Allen test to confirm intact palmar arch before using radial artery inflow
- Central venous evaluation if history of central lines or arm swelling
Maturation: AVF requires 4–6 weeks minimum for maturation. A mature AVF shows a continuous thrill, low-pitch bruit, and adequate flow on duplex ultrasound. The "rule of 6s": flow ≥600 mL/min, diameter ≥6 mm, depth ≤6 mm.
Sabiston Textbook of Surgery, p. 2391
1.2 Arteriovenous Graft (AVG)
Used when native vessels are inadequate for AVF creation. Made from expanded polytetrafluoroethylene (ePTFE), polyurethane, or biologically processed bovine carotid artery.
- Can be used within 24–72 hours (early cannulation grafts) or 2–4 weeks after placement
- Lower long-term patency than AVF; most common failure is venous anastomotic stenosis from neointimal hyperplasia
- 12-month primary patency: 43–64%; secondary patency: 71–86%
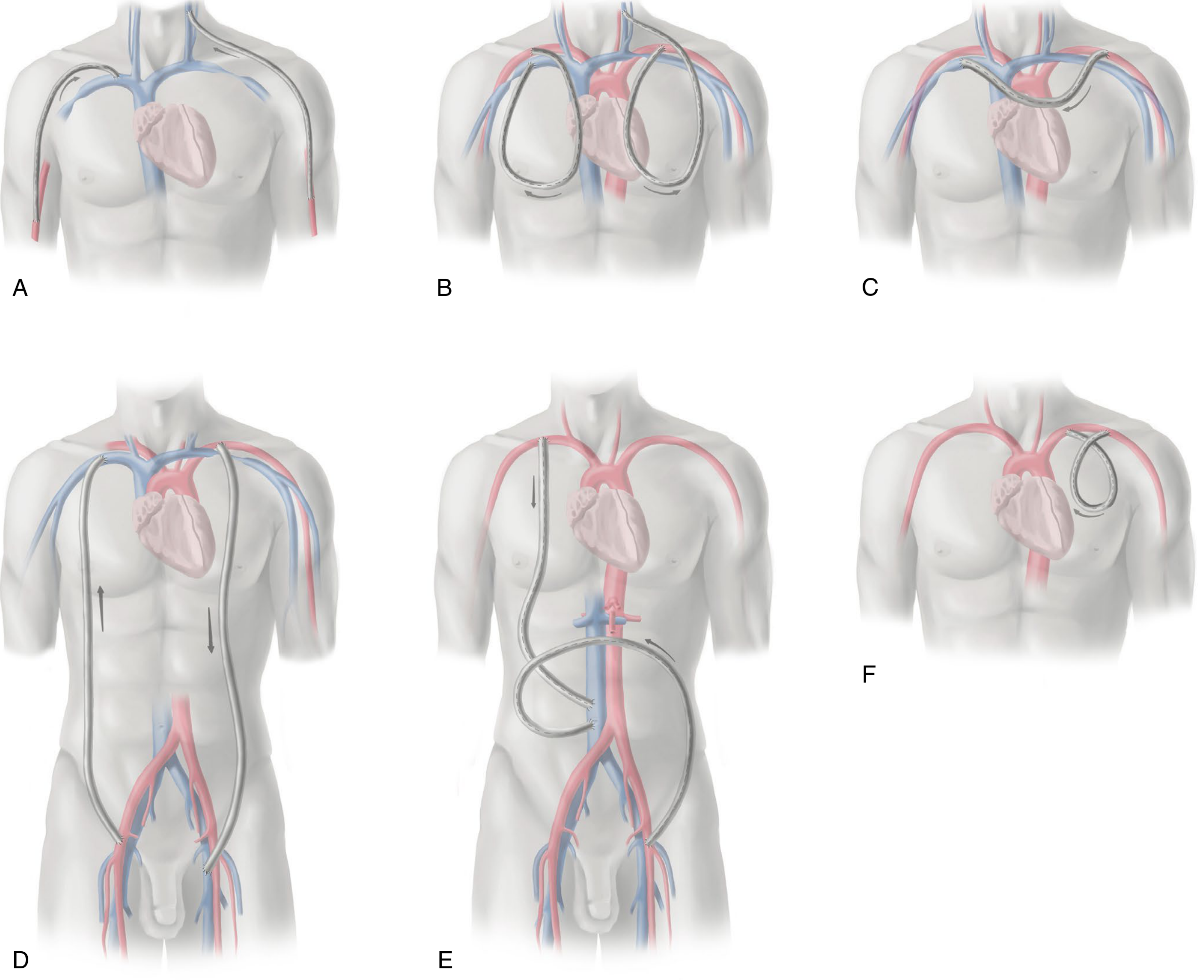
Configurations when upper extremity vessels are exhausted:
- Cervical AVG (brachial artery → subclavian or jugular vein)
- Chest wall loop AVG (axillary artery → axillary vein)
- Axillofemoral AVG
1.3 Tunneled Dialysis Catheter (TDC)
Inserted through a subcutaneous tunnel, typically in the internal jugular or femoral vein; the cuff anchors the catheter and reduces infection. TDCs are used:
- As a bridge to permanent access maturation
- When permanent access is not feasible
- As long-term access in limited-life patients
The problem: ~80% of patients in the United States start HD with a catheter. Catheter use is associated with higher mortality, more hospitalizations, and greater cost than AVF. KDOQI advocates a "catheter-last" approach rather than the older "fistula-first" paradigm.
2. "Vein Preservation" Strategy
Patients with CKD who may need future HD should avoid:
- PICC lines (cause venous stenosis in cephalic/basilic veins)
- Repeated venipuncture in the forearm cephalic vein
- Blood pressure measurement in the planned access arm
Brenner and Rector's The Kidney, p. 2703
3. Access Monitoring & Surveillance
Physical examination remains the most important monitoring technique:
- Normal AVF: soft, compressible, continuous thrill; low-pitch bruit
- Venous outflow stenosis: bounding, pulsatile fistula that does not flatten when the arm is raised
- Inflow/anastomotic stenosis: diminished thrill
Objective tools include:
- Static/dynamic venous pressure monitoring (serial measurements more valuable than single threshold)
- Ultrasound dilution method (Transonic device) — measures access blood flow; decline predicts impending failure
- Declining Kt/V or prolonged hemostasis time should prompt access evaluation
Primary patency = function without any intervention since creation. After any intervention, secondary patency applies.
Brenner and Rector's The Kidney, p. 2154
4. Complications of Vascular Access
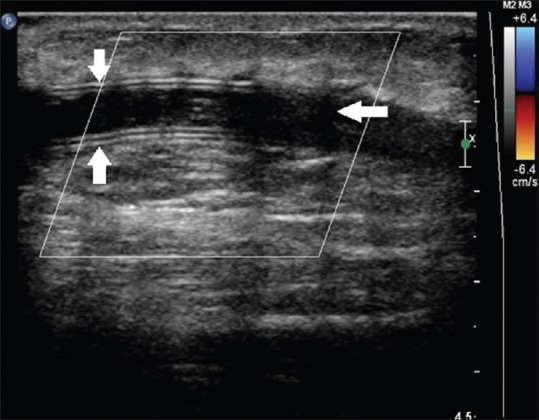
4.1 Stenosis and Thrombosis
The most common cause of access failure.
- AVF: usually juxta-anastomotic stenosis or venous outflow stenosis
- AVG: neointimal hyperplasia at the venous anastomosis is the dominant mechanism
- Presentation: declining flow, difficulty cannulating, prolonged bleeding time, reduced Kt/V
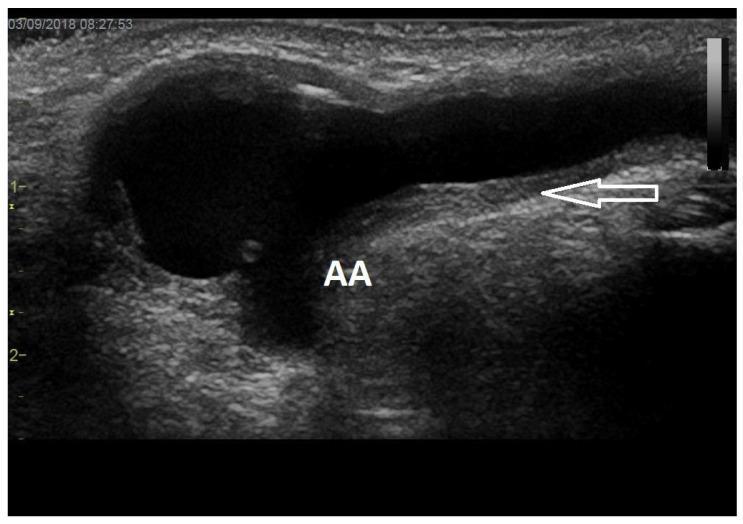
Ultrasound findings:
Management:
- Percutaneous transluminal angioplasty (PTA/venoplasty) — first-line for most stenoses
- Stent placement: evidence supports stent superiority over balloon alone for venous anastomotic stenosis of AVG (RCT, n=190)
- Thrombectomy (pharmacomechanical or surgical) for acute thrombosis
- Central venous stenosis: balloon venoplasty ± stent; surgical bypass (jugular turndown) as last resort
4.2 Infection
AVF infections are uncommon due to autologous tissue. AVG infections are more frequent (ePTFE is susceptible to biofilm formation). Catheter infections are the most serious.
| Access Type | Infection Rate | Common Organisms |
|---|---|---|
| AVF | Lowest | S. aureus, gram-negatives |
| AVG | Intermediate | S. aureus, Pseudomonas |
| TDC | Highest | S. aureus (MRSA common), CoNS |
TDC infections:
- Exit-site infection: erythema/exudate at skin entry — treat topically ± systemic antibiotics
- Tunnel infection: cellulitis along tunnel track — requires catheter removal
- Catheter-related bloodstream infection (CRBSI): bacteremia from catheter — requires antibiotics ± catheter removal; S. aureus and Candida generally mandate removal; other organisms may be "salvaged" with antibiotic lock therapy
Early identification of local catheter infections is key to preventing systemic sepsis. A 2023 systematic review (PMID 37178476) specifically addressed systematic surveillance of local TDC infections.
4.3 Venous Hypertension (Central Venous Stenosis/Occlusion)
- Results from prior central venous catheters (subclavian > internal jugular) causing fibrotic stenosis
- Presentation: ipsilateral arm edema, dilated chest wall veins, facial/neck swelling, difficulty achieving adequate dialysis
- Investigation: CT venogram or catheter-based venogram
- Treatment: balloon venoplasty; stent if significant recoil; surgical bypass if endovascular fails
4.4 Aneurysms and Pseudoaneurysms
- True aneurysms (AVF): degeneration of venous wall from repeated cannulation; progressive dilation
- Pseudoaneurysms (AVG): failure of ePTFE graft wall integrity at cannulation sites; risk of rupture
- Indications for intervention: rapid expansion, skin breakdown/ulceration, infection, pain, cosmetic concern, inability to cannulate
- Management: surgical resection/interposition graft, endovascular covered stent
4.5 Hemodialysis Access-Induced Distal Ischemia (HAIDI) / "Steal Syndrome"
Access creation diverts blood from the distal limb through a low-resistance circuit.
Incidence:
- Forearm fistulas: <1%
- Antecubital-based fistulas: up to 8%
- AVG: often early onset (within 30 days)
Risk factors: Advanced age, female sex, diabetes, peripheral arterial disease, brachial artery inflow, large-diameter outflow conduit, prior steal
HAIDI grading (SVS):
| Grade | Features |
|---|---|
| 0 | No symptoms |
| 1 | Coldness/pallor; no pain |
| 2 | Ischemic pain on exercise or during dialysis |
| 3 | Ischemic rest pain, tissue necrosis, gangrene |
Workup: Photoplethysmography with/without fistula compression; duplex ultrasound assessing flow volume and direction
Management (depends on access flow volume):
- High-flow (>1 L/min): Banding (least invasive; 33% failure, 11% thrombosis) or Revision Using Distal Inflow (RUDI)
- Low/normal flow: DRIL (Distal Revascularization–Interval Ligation) — most effective; restores antegrade flow but sacrifices normal arterial continuity — or PAI (Proximal Arterial Inflow) — increases forearm pressure without sacrificing arterial continuity
- Radiocephalic fistulas: radial artery ligation distal to anastomosis (if palmar arch intact)
- Grade 3 ischemia / digital gangrene: access ligation
Sabiston Textbook of Surgery, p. 2393
4.6 Ischemic Monomelic Neuropathy (IMN)
- Acute, devastating complication occurring immediately after access creation (usually brachial artery-based access in diabetics)
- Caused by acute ischemia of peripheral nerves despite apparently intact macrovascular flow
- Presentation: severe burning pain, weakness, sensory loss in multiple nerve distributions of the hand immediately post-op
- No vascular insufficiency may be apparent clinically
- Management: immediate access ligation — delay leads to permanent neurological deficit
- Distinguished from steal syndrome by the absence of major ischemic skin changes
4.7 High-Output Heart Failure
- Access blood flow >1–2 L/min diverts cardiac output
- Particularly problematic in patients with pre-existing cardiomyopathy
- Presents with progressive dyspnea, increased cardiac output, and cardiomegaly
- Nicoladoni-Branham sign: compression of the access causes reflex bradycardia
- Management: access banding, conversion to a lower-flow configuration, or access ligation
4.8 Access Non-Maturation (AVF-Specific)
- Up to 30–40% of AVFs fail to mature sufficiently for use
- Causes: small vessel diameter, venous outflow stenosis, accessory veins stealing flow
- Maturation interventions: angioplasty of stenotic segments, accessory vein ligation, superficialization (surgical transposition of deep veins)
- The 2023 systematic review on non-conventional techniques for radiocephalic AVF (PMID 39096957) describes strategies to improve maturation rates
5. Peritoneal Dialysis Catheter Complications (Brief)
| Complication | Notes |
|---|---|
| Malfunction/poor drainage | Omental wrap, catheter displacement, constipation |
| Exit-site infection | Treated with local antibiotics |
| Tunnel infection | May need catheter removal |
| Peritonitis | Most serious — Staphylococcus and Streptococcus most common; gram-negative peritonitis carries worse prognosis |
Percutaneous placement is associated with fewer exit-site infections and peritonitis at 30 days compared to open surgical placement (meta-analysis data).
Summary Table
| Complication | AVF | AVG | TDC |
|---|---|---|---|
| Stenosis/thrombosis | ++ | +++ | + |
| Infection | + | ++ | +++ |
| Aneurysm | ++ | + (pseudo) | — |
| Steal/HAIDI | +/++ | ++ | — |
| IMN | + | + | — |
| High-output failure | + | + | — |
| Non-maturation | +++ | — | — |
| Central vein stenosis | + | + | +++ |
Key References:
- Sabiston Textbook of Surgery, 21st ed., Chapter 107 (Dialysis Access) — p. 2385–2397
- Brenner and Rector's The Kidney, 10th ed., Chapter 63 — p. 2703–2715
- KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update (Lok CE et al., Am J Kidney Dis 2020;75:S1–S164)
- PMID 37178476 — Systematic review: early identification of local infections in HD catheters (2023)
- PMID 39096957 — Systematic review: non-conventional techniques for radiocephalic AVF (2025)
- PMID 40123557 — Review: Alpha to Omega of Dialysis Access (AVF and AVG), Part 1 (2025)
This is a shared conversation. Sign in to Orris to start your own chat.