INGUINAL HERNIA - MS GENERAL SURGERY LONG CASE
Image-Enriched Complete University Examination Guide
Sources: Bailey & Love 28th Ed · Schwartz 11th Ed · Fischer's Mastery of Surgery 8th Ed · S. Das 13th Ed · Thieme General Anatomy Atlas · EHS/HerniaSurge Guidelines 2018
PART 1: SURGICAL ANATOMY WITH IMAGES
1.1 Sites of All Abdominal Wall Hernias
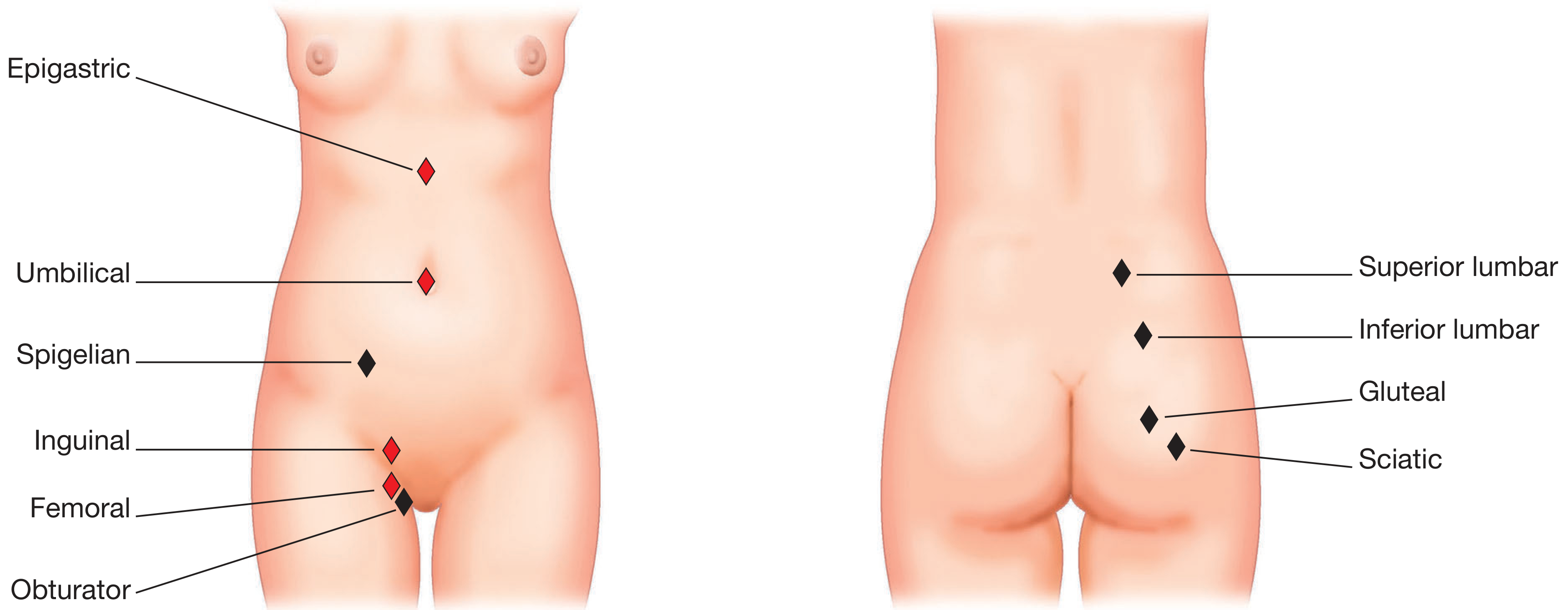
Figure 1. Sites of abdominal wall hernias - common hernias in red, rare in black. Incisional and parastomal hernias can occur at various sites.
(Bailey & Love's Short Practice of Surgery, 28th Edition)
Examiner Q: Name all the sites where a hernia can occur in the groin.
A: Inguinal (indirect, direct), femoral, obturator, spigelian (lateral border of rectus). In the groin specifically: indirect inguinal (through deep ring - most common), direct inguinal (through Hesselbach's triangle), femoral (through femoral ring). All three emerge through the myopectineal orifice of Fruchaud.
1.2 Close Relationships of Inguinal, Direct, and Femoral Hernias
Figure 2. The close relationships of direct inguinal, indirect inguinal, and femoral hernias. Note the key landmark - the inferior epigastric artery - and the position of the femoral vessels.
(Bailey & Love's Short Practice of Surgery, 28th Edition)
Key points from this image:
| Hernia | Relation to Inferior Epigastric Artery | Relation to Inguinal Ligament | Relation to Pubic Tubercle |
|---|
| Indirect inguinal | Lateral to IEA | Above | Medial to |
| Direct inguinal | Medial to IEA | Above | Medial to |
| Femoral | Below and lateral | Below | Lateral to |
Examiner Trap: The inferior epigastric artery is the single most important intraoperative and clinical landmark. Candidates who confuse "medial" and "lateral" in relation to the IEA for direct vs indirect hernia ALWAYS fail this question.
1.3 Superficial Dissection of the Inguinal Region (Male, Female, and Ligament)
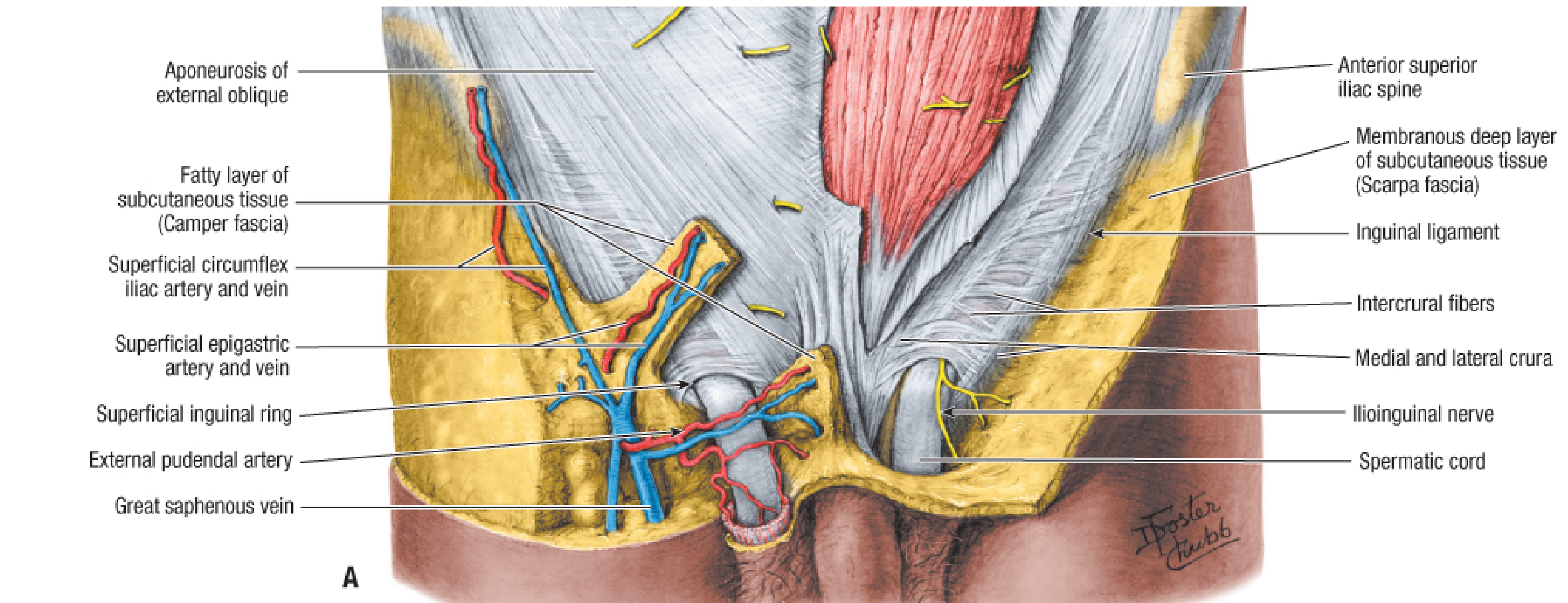
Figure 3A. Superficial dissection of the male inguinal region showing Camper's fascia, superficial inguinal vessels, and inguinal lymph nodes.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.1A)
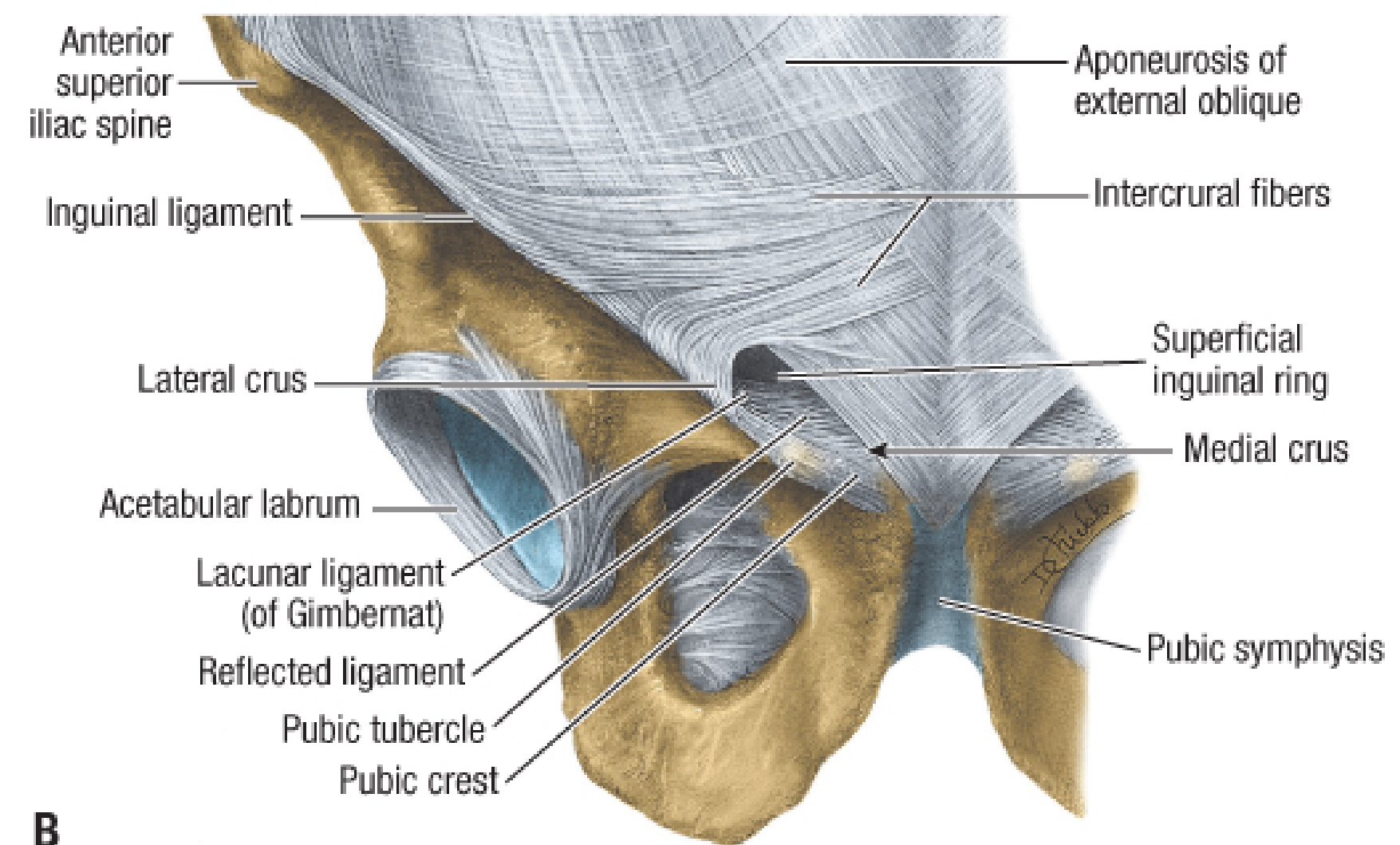
Figure 3B. Inguinal ligament and superficial inguinal ring showing medial and lateral crura and intercrural fibers.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.1B)
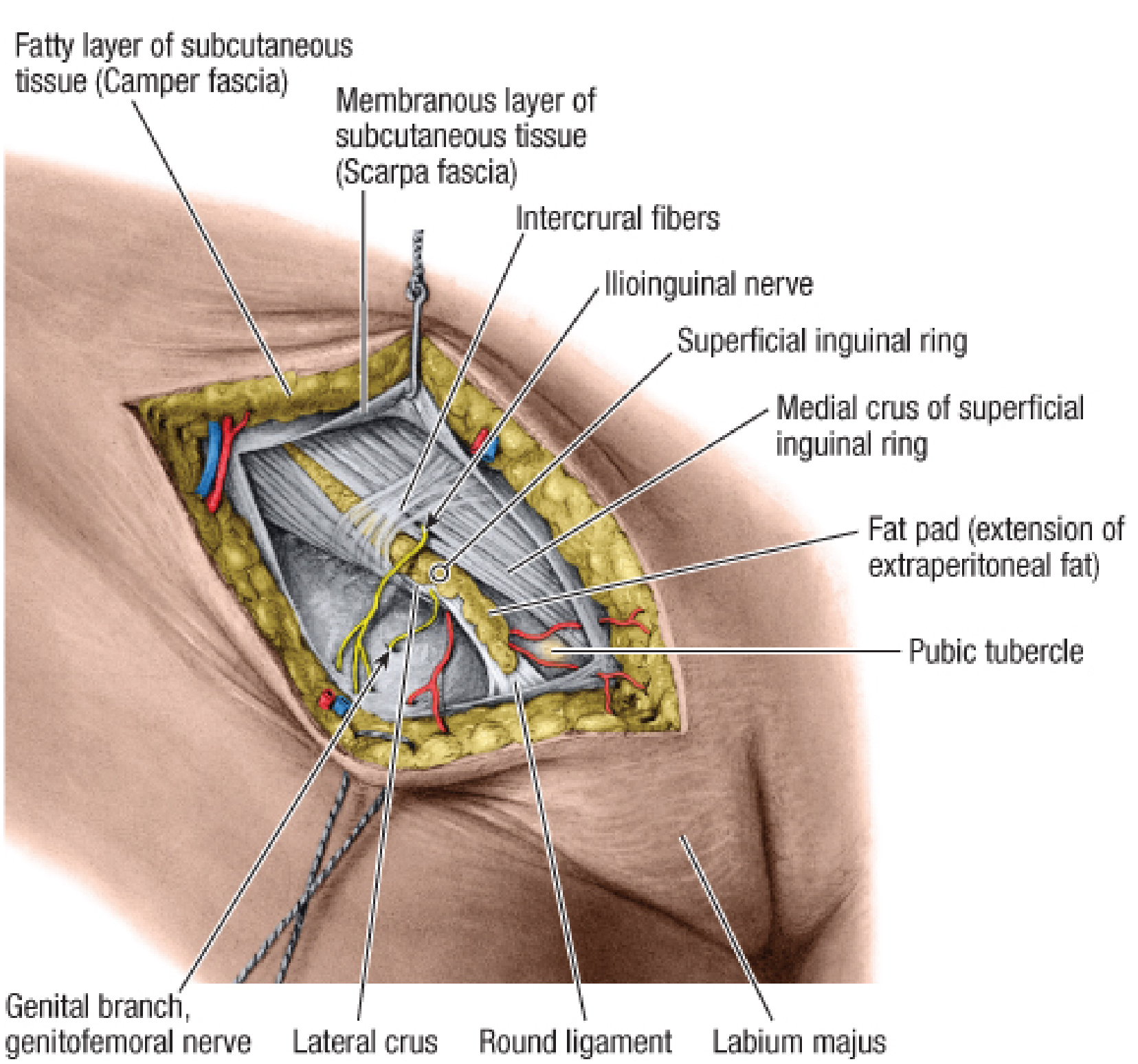
Figure 3C. Female inguinal region. The round ligament of the uterus exits the superficial inguinal ring and divides into fibrous strands attaching to the labium majus.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.1C)
Viva Q: What is the "canal of Nuck"?
A: The inguinal canal in the female is sometimes called the canal of Nuck. A patent processus vaginalis in the female causes a hydrocele of the canal of Nuck (equivalent to indirect inguinal hernia in males). A Nuck hydrocele presents as a groin swelling in young females.
1.4 Deep Inguinal Region - Serial Dissections and Canal Anatomy
Figure 4. Deep inguinal region. Serial dissections (A, B) and the inguinal canal (C). Note the deep inguinal ring in transversalis fascia, the iliopubic tract below it, and the arrangement of nerves.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.2)
Anatomy Summary from this Image:
LAYERS OF THE INGUINAL REGION (lateral to medial, superficial to deep):
=======================================================================
1. Skin
2. Subcutaneous fat (Camper's fascia - fatty layer)
3. Scarpa's fascia (membranous layer - important for wound closure)
4. External oblique aponeurosis (forms anterior wall of canal)
5. Internal oblique muscle (forms roof + anterior wall laterally)
6. Transversus abdominis muscle (forms roof)
7. Transversalis fascia (forms posterior wall; deep ring is defect here)
8. Preperitoneal fat
9. Peritoneum
Deep Inguinal Ring: The deep inguinal ring is the beginning of the evagination of the transversalis fascia. Its lower margin is reinforced by the iliopubic tract (thickened inferior edge of transversalis fascia). The iliopubic tract then crosses the femoral canal anteriorly to attach to Cooper's ligament - this is why the iliopubic tract is a critical landmark in TEP/TAPP.
1.5 Hesselbach's Triangle and Direct vs Indirect Hernia Anatomy
Figure 5. Hesselbach's (inguinal) triangle and the relationship of direct vs indirect inguinal hernias to the inferior epigastric vessels, spermatic cord, and inguinal ligament.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.3)
Key Diagram: Hesselbach's Triangle
INFERIOR
EPIGASTRIC ARTERY
(superolateral
border)
/
/
RECTUS / INDIRECT HERNIA
SHEATH ─────X (lateral to IEA)
(medial / \
border) / \
/ ↑ \
/ DIRECT\
/ HERNIA \
─────────────────────────────────────
INGUINAL LIGAMENT (inferior border)
Direct hernia: Passes through Hesselbach's triangle - medial to inferior epigastric vessels. Lies adjacent to (not within) the spermatic cord. Covered by external spermatic fascia only (not cremasteric or internal spermatic fascia).
Indirect hernia: Passes through the deep ring - lateral to inferior epigastric vessels. Lies within the spermatic cord - covered by all three cord coverings (internal spermatic fascia + cremasteric fascia + external spermatic fascia).
This is the most clinically important anatomical distinction. Examiners always ask this.
1.6 Inguinal Ligament, Femoral Canal, and Femoral Sheath
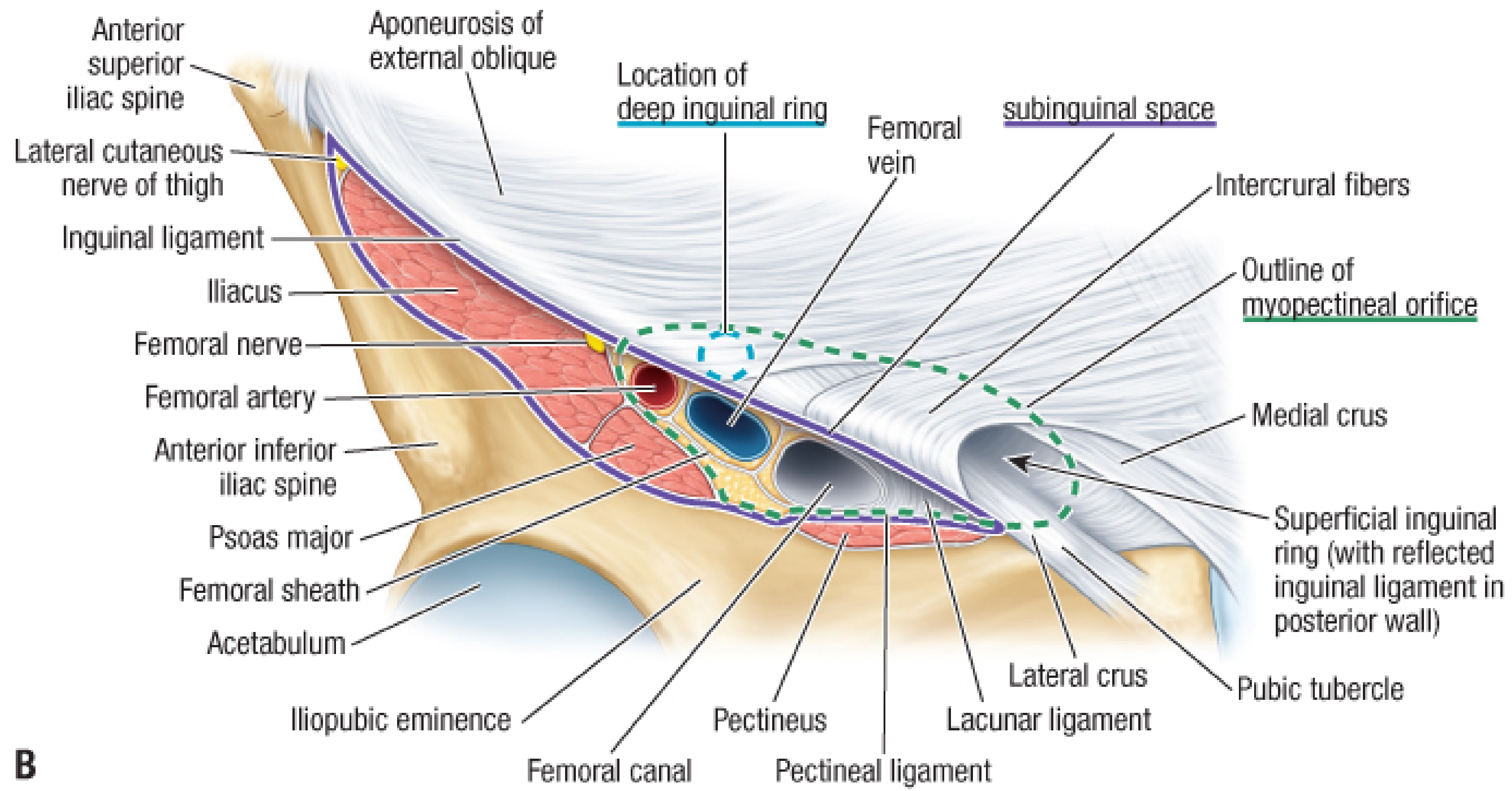
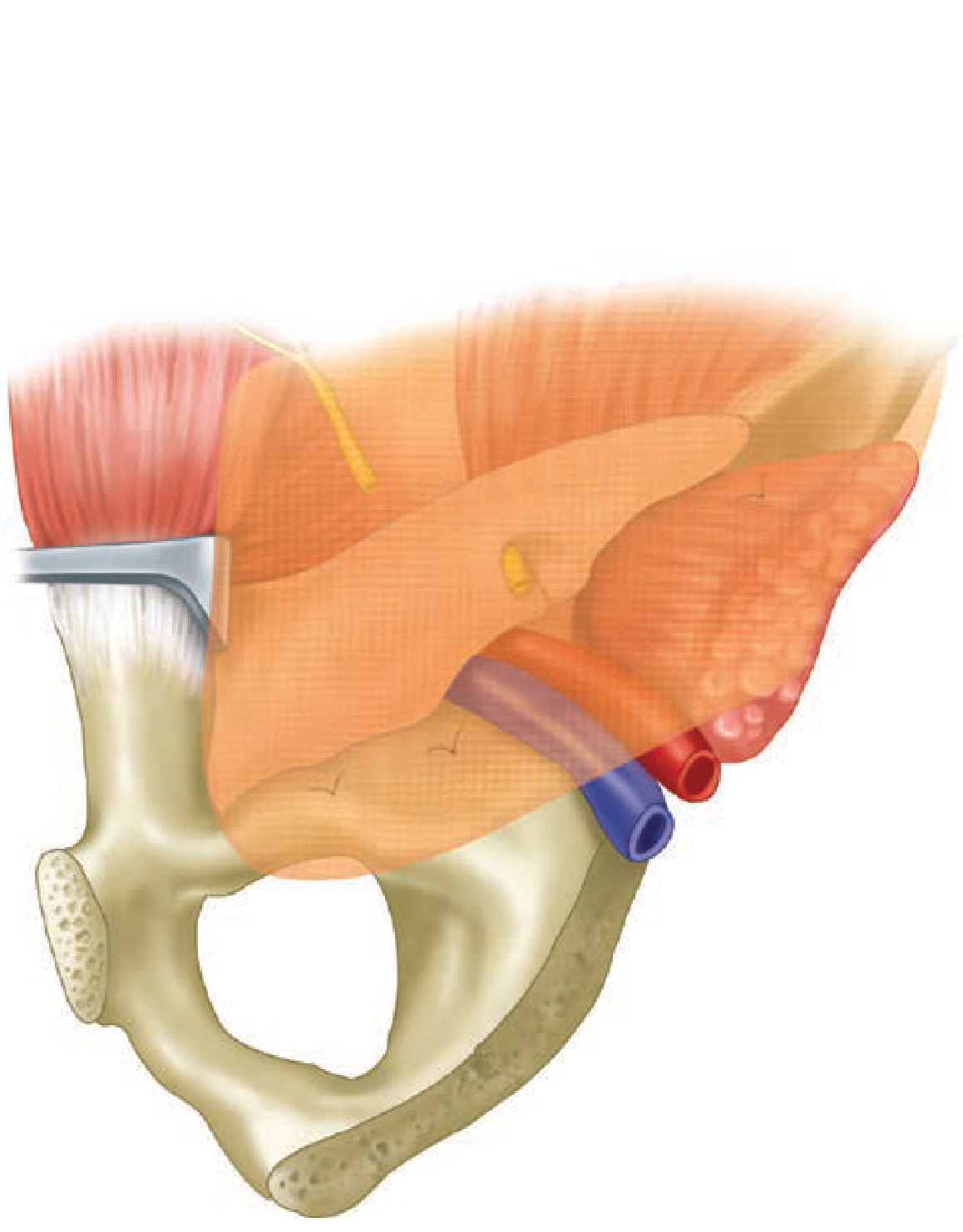
Figure 6. Inguinal ligament, femoral canal, and femoral sheath showing the relationship of the femoral artery, vein, and canal (most medial). Note the femoral ring.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.5A)
Femoral Ring Boundaries (For Femoral Hernia - KEY for MCQ):
| Border | Structure |
|---|
| Anterior (and inferior) | Iliopubic tract / inguinal ligament |
| Medial | Lacunar (Gimbernat's) ligament - rigid, sharp edge |
| Posterior | Pectineal (Cooper's) ligament and pectineus fascia |
| Lateral | Femoral vein (medial wall of femoral sheath) |
Why femoral hernias strangulate so readily: The lacunar ligament (Gimbernat's) forms a rigid, unyielding, crescent-shaped medial border. The entire ring is rigid bony and ligamentous. Any swelling of hernial contents immediately compromises blood supply. Strangulation rate of femoral hernia = ~40% at presentation.
1.7 Anomalous Obturator Artery (Corona Mortis)
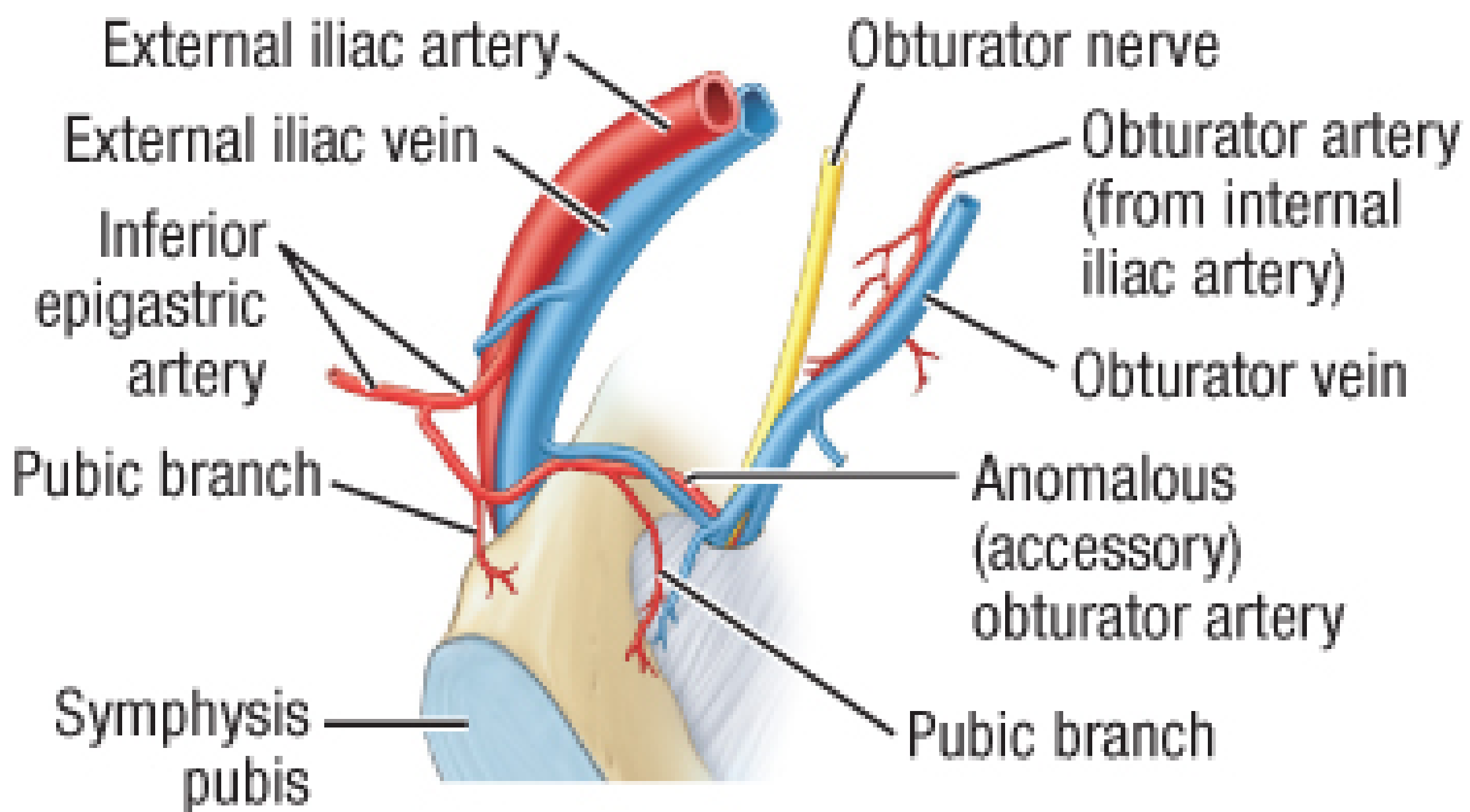
Figure 7. Anomalous obturator artery arising from the external iliac or inferior epigastric artery (instead of the internal iliac). Present in ~30% of individuals. Lies on or near Cooper's ligament. If divided or torn = profuse, life-threatening hemorrhage.
(Fischer's Mastery of Surgery, 8th Edition - Figure 221.6)
Corona Mortis ("Crown of Death"): This is the anastomotic loop between the obturator artery (normal or anomalous) and the external iliac/inferior epigastric arteries. It runs across or near Cooper's ligament. During TEP/TAPP, never apply blind tacks or sutures to Cooper's ligament without visualizing this vessel. Hemorrhage here is the classic catastrophic complication of laparoscopic hernia repair.
1.8 Testicular Descent and Processus Vaginalis
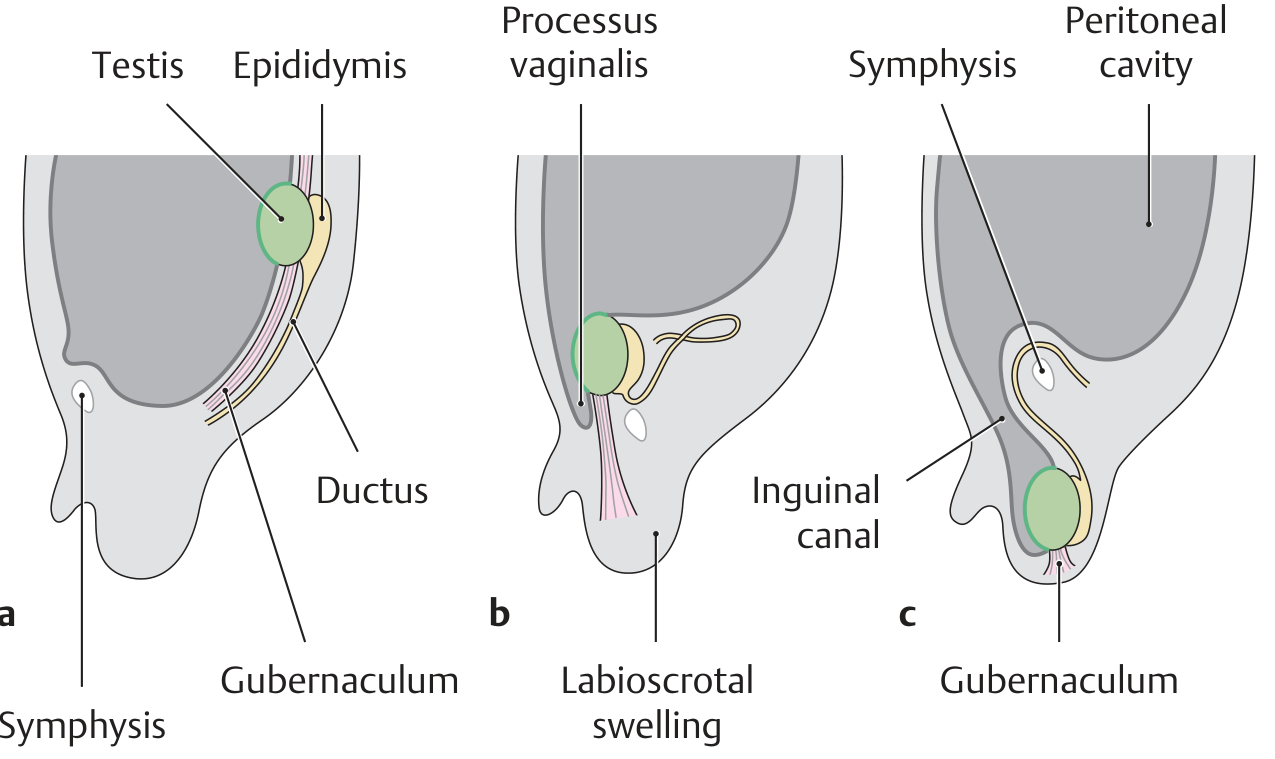
Figure 8A. Stages of testicular descent: (a) 2nd month - at urogenital fold, (b) 3rd month - at inguinal canal entrance, (c) at birth - in scrotum, (d) after obliteration of processus vaginalis. Note the gubernaculum pulling the testis through the inguinal canal.
(Thieme General Anatomy & Musculoskeletal System Atlas)
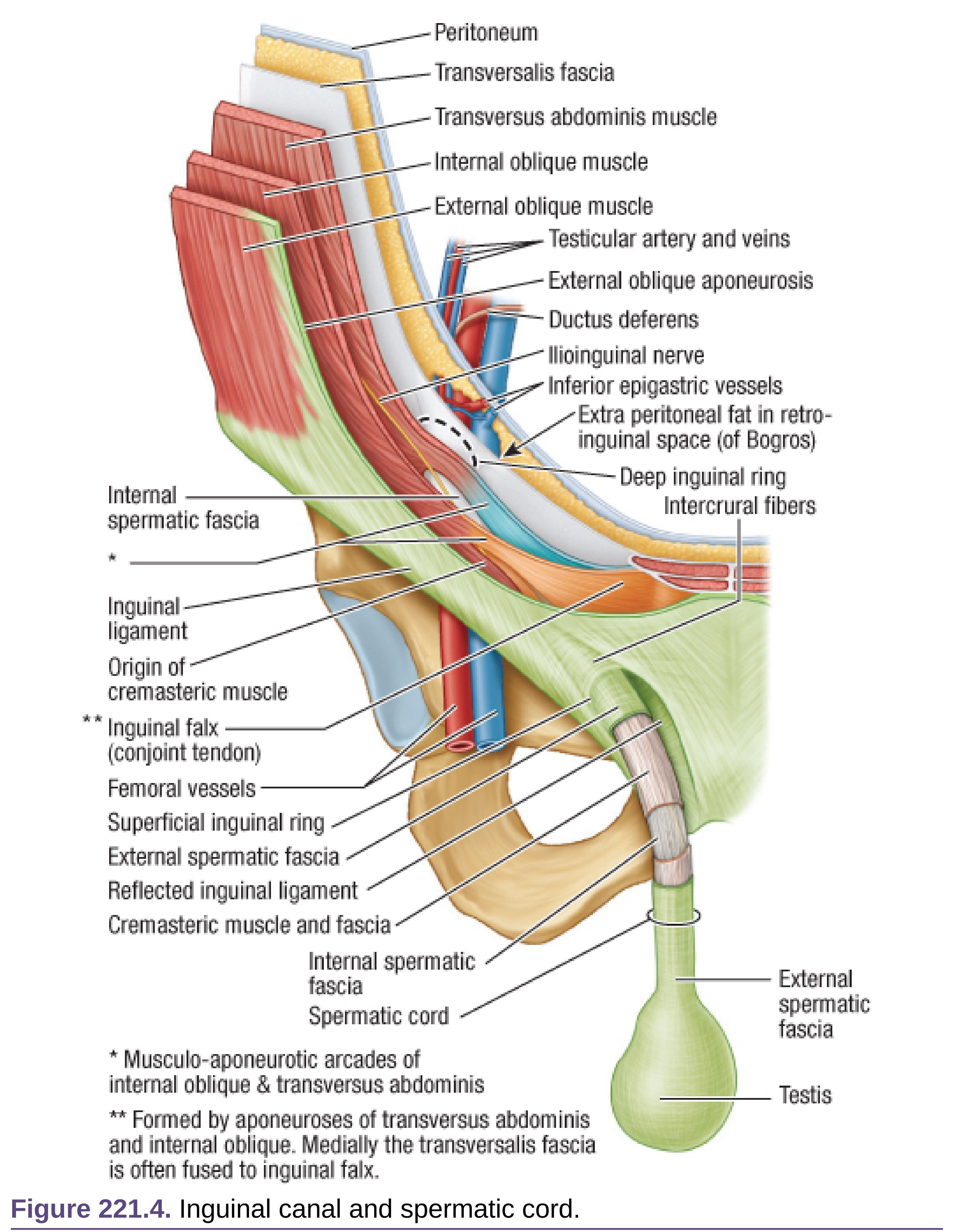
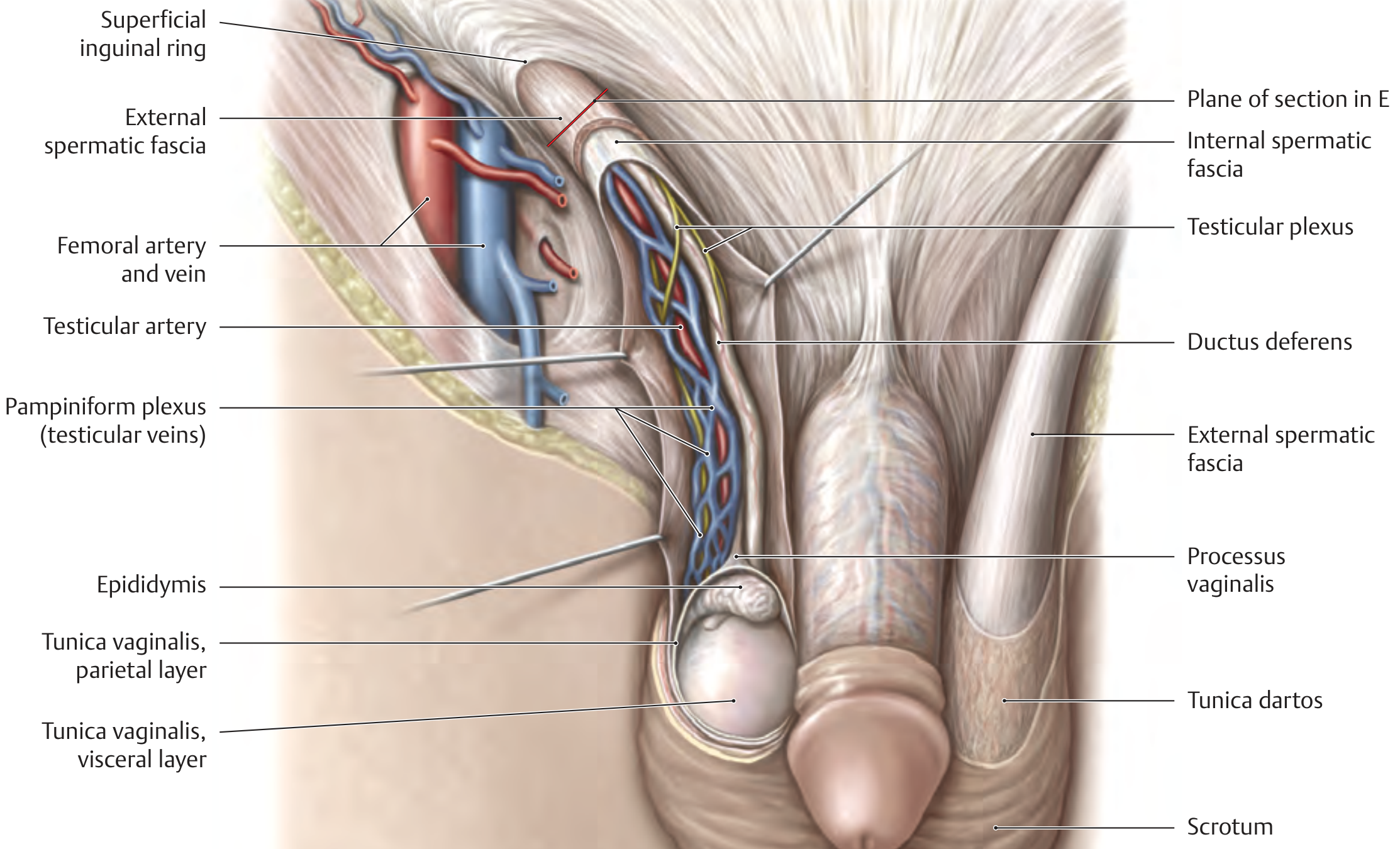
Figure 8B. Cross-sectional anatomy of the inguinal canal showing the three layers of the spermatic cord (formed by layers of abdominal wall pulled down with the testis).
(Thieme General Anatomy & Musculoskeletal System Atlas)
Coverings of the Spermatic Cord - Derived from Abdominal Wall Layers:
| Cord Covering | Derived From |
|---|
| External spermatic fascia | External oblique aponeurosis |
| Cremasteric fascia and muscle | Internal oblique muscle |
| Internal spermatic fascia | Transversalis fascia |
| Tunica vaginalis (around testis) | Peritoneum (processus vaginalis) |
Viva Q: Why does an indirect hernia lie WITHIN the cord while a direct hernia lies ADJACENT to it?
Because the indirect hernia sac passes through the deep ring along the same track taken by the testis during descent - it literally descends within the coverings of the cord. The direct hernia bulges through the posterior wall of the canal (Hesselbach's triangle) and merely lies adjacent to the cord, covered only by external spermatic fascia.
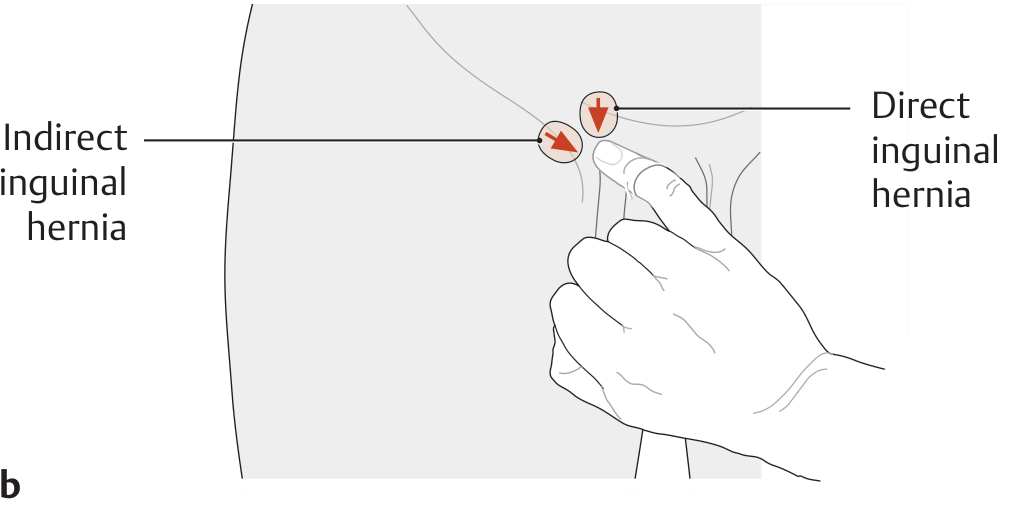
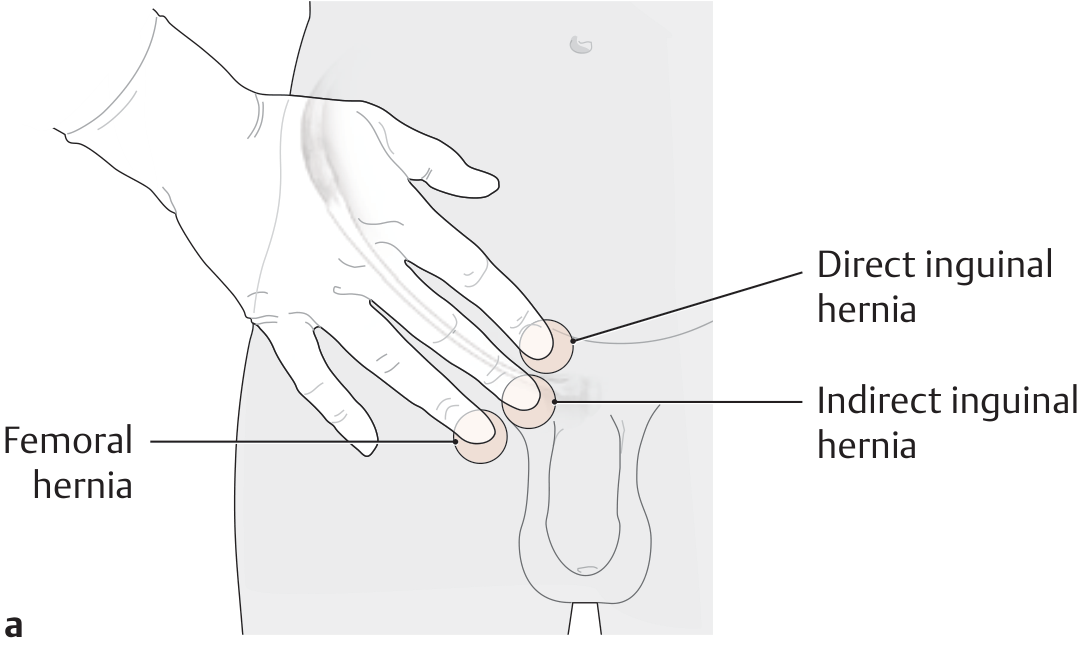
1.9 Three-Finger Rule for Clinical Examination
Figure 9. Zieman's three-finger palpation technique. The examiner places the thenar eminence on the ASIS:
- Index finger → points to the direct inguinal hernia site (Hesselbach's triangle)
- Middle finger → points to the indirect inguinal hernia site (deep ring)
- Ring finger → points to the femoral hernia site (femoral ring/fossa ovalis)
(Thieme General Anatomy & Musculoskeletal System Atlas)
Figure 10. Clinical location of inguinal vs femoral hernia relative to the inguinal ligament and pubic tubercle.
(Thieme General Anatomy & Musculoskeletal System Atlas)
Clinical Examination Steps with This Knowledge:
Step 1: Patient stands. Look for swelling.
Step 2: Palpate with three fingers (Zieman's technique) - identify which site bulges on coughing.
Step 3: Identify pubic tubercle - is the swelling medial+above (inguinal) or lateral+below (femoral)?
Step 4: Deep ring occlusion - compress the deep ring (middle finger position) and ask patient to cough:
- Hernia disappears = indirect (deep ring is its neck)
- Hernia still appears medially = direct (exits through Hesselbach's triangle regardless)
PART 2: CLINICAL PHOTOGRAPH
2.1 Clinical Appearance of Inguinal Hernia
Figure 11. Oblique (indirect) left inguinal hernia that becomes apparent when the patient coughs and persists until reduced when he lies down. This image demonstrates why the examination must be performed in the standing position first.
(Bailey & Love's Short Practice of Surgery, 28th Edition - Figure 64.13)
Key teaching point: Many inguinal hernias that are irreducible in the standing position will reduce spontaneously when the patient lies flat. If you examine only in the supine position, you will miss a significant proportion of hernias. Always examine standing first.
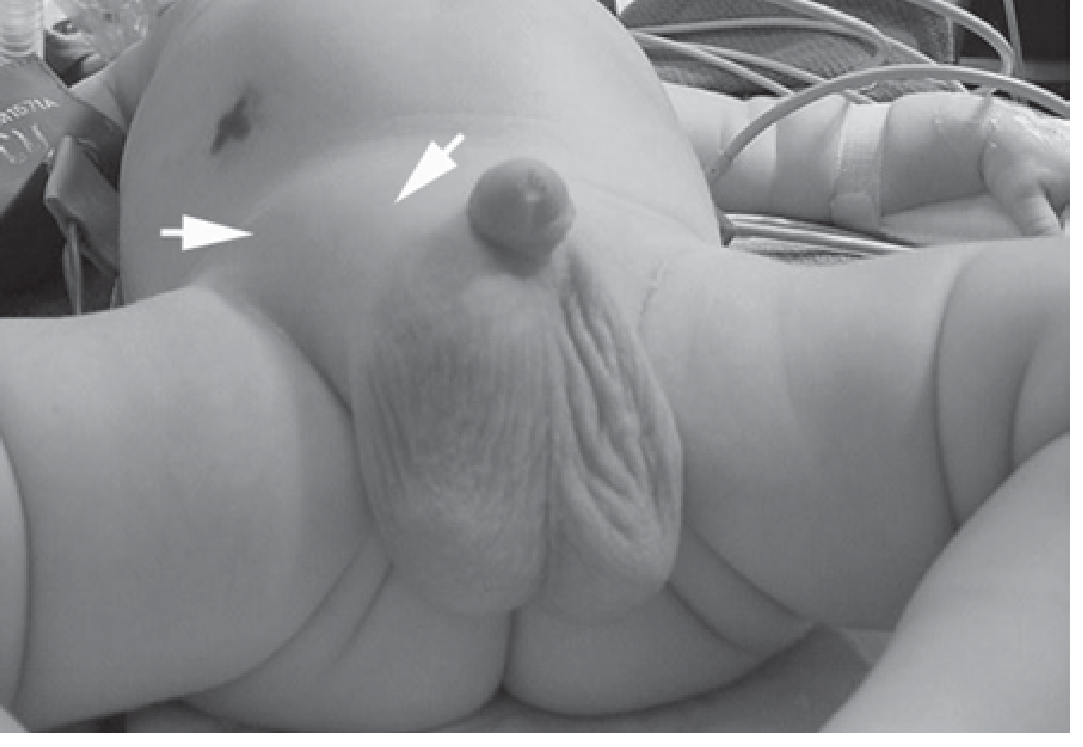
2.2 Inguinal Hernia in an Infant
Figure 12. Right inguinal hernia in a 4-month-old male. Arrows indicate the bulge in the right groin. All hernias in infants are indirect (congenital - patent processus vaginalis). Management = elective herniotomy (sac ligation) without floor repair.
(Schwartz's Principles of Surgery, 11th Edition - Figure 39-35)
Viva Q: Why are infants and premature babies at especially high risk of incarceration?
The inguinal ring in infants is narrow and tight. The geometry of the canal is that of a wide-angle cylinder at birth, becoming a cone with aging. In infants, the narrow ring provides little room for bowel to slide back - once herniated, incarceration and strangulation can develop rapidly. Premature infants have a higher incidence (5-30%) due to incomplete processus vaginalis obliteration.
PART 3: OPERATIVE ANATOMY AND IMAGES
3.1 Bassini's Original Diagram (1890) - Inguinal Canal Anatomy
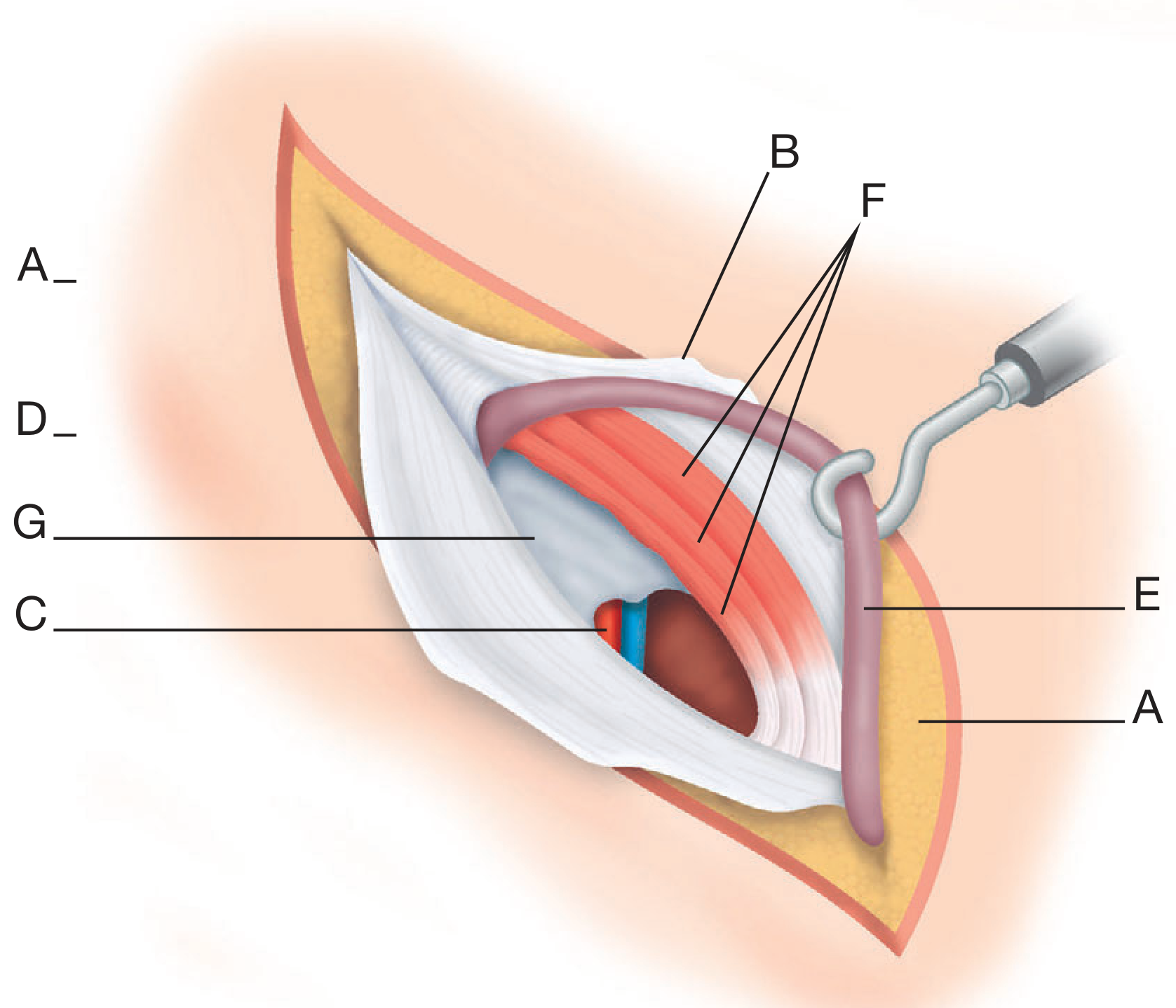
Figure 13. Bassini's original anatomical diagram (1890) showing the layers of the inguinal canal. Labels: A = subcutaneous fat, B = external oblique aponeurosis (opened), C = inferior epigastric vessels, D = Poupart's (inguinal) ligament, E = spermatic cord retracted, F = conjoint tendon, G = transversalis fascia.
(Bailey & Love's Short Practice of Surgery, 28th Edition - Figure 64.14)
Bassini Repair - What He Actually Did:
Bassini's genius was to recognize that the hernia occurred because of weakening of the posterior wall of the inguinal canal. His repair:
- Opens the external oblique aponeurosis to expose the canal
- Performs herniotomy (excises the sac)
- Sutures the triple layer (transversalis fascia + internal oblique + transversus aponeurosis = "conjoint tendon") to the inguinal (Poupart's) ligament
- The spermatic cord is placed on top of this repair before closing the external oblique
The Bassini repair reduced hernia recurrence from 80% (pre-Bassini era) to approximately 10% - a revolutionary achievement in 1890.
3.2 Open Anterior Approach - Incision and Layers
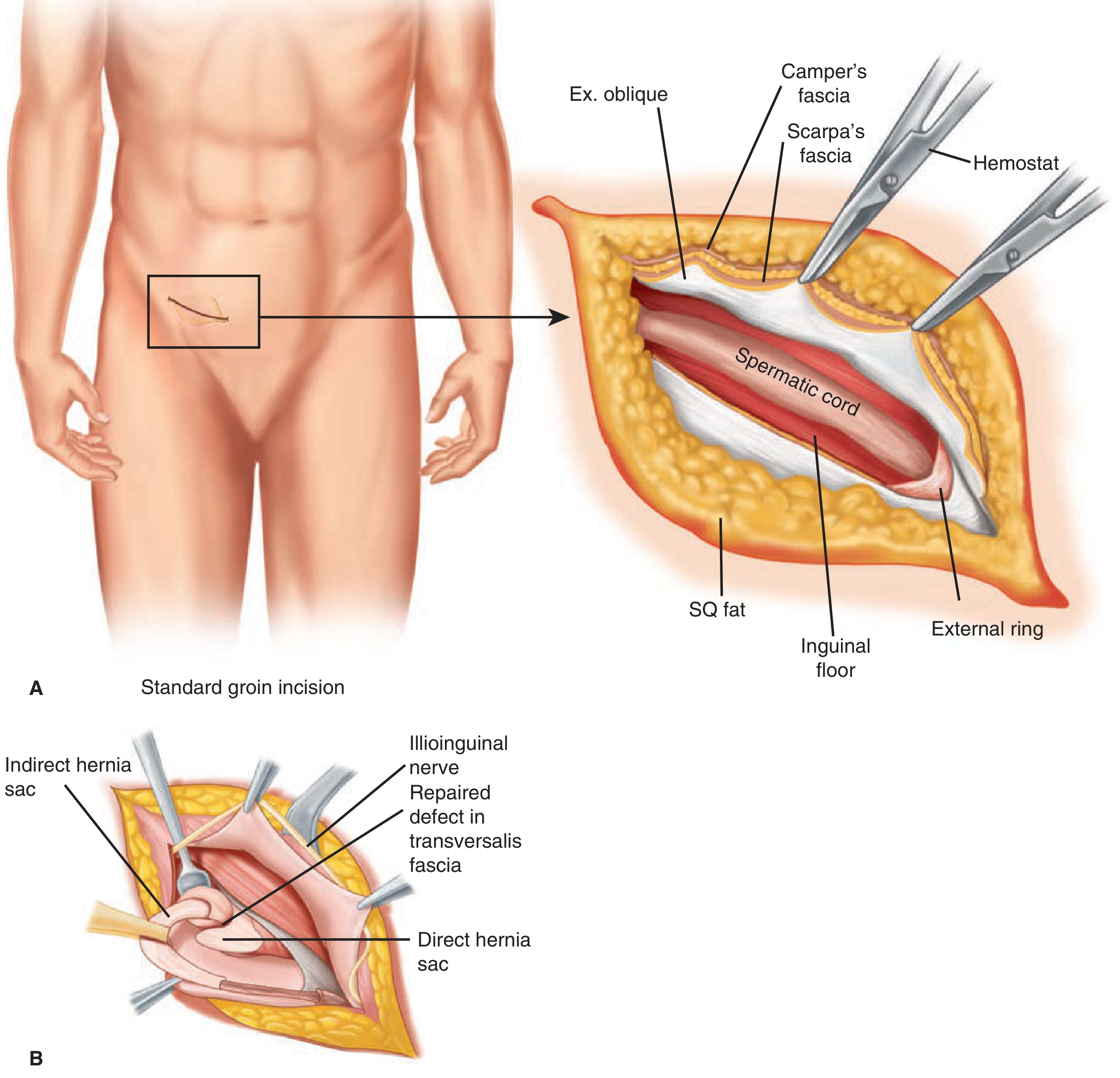
Figure 14. Open anterior approach. A: Layers of the abdominal wall during anterior open hernia repair. B: Identification of indirect (anteromedial to cord) and direct hernia sacs with retraction of the spermatic cord and ilioinguinal nerve.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-13)
Operative Steps for Open Inguinal Hernia Repair:
Incision: 2 cm above and parallel to the inguinal ligament (medial half), in the skin crease - 6-8 cm long.
Layer by layer dissection:
- Skin and subcutaneous fat (Camper's fascia)
- Scarpa's fascia - incise, then use for closure
- External oblique aponeurosis - open along fiber direction from superficial ring toward deep ring
- Identify and protect ilioinguinal nerve (lies just deep to external oblique, on anterior surface of cord)
- Identify iliohypogastric nerve (runs superior and parallel to the incision)
- Mobilize the spermatic cord on a soft Penrose drain or vascular tape
Identify the hernia sac:
- Indirect sac: Anteromedial surface of the cord (lies within cord coverings)
- Direct sac: Posterior to the cord, bulging from the inguinal floor medially
- Both may coexist (pantaloon hernia)
3.3 Shouldice Repair
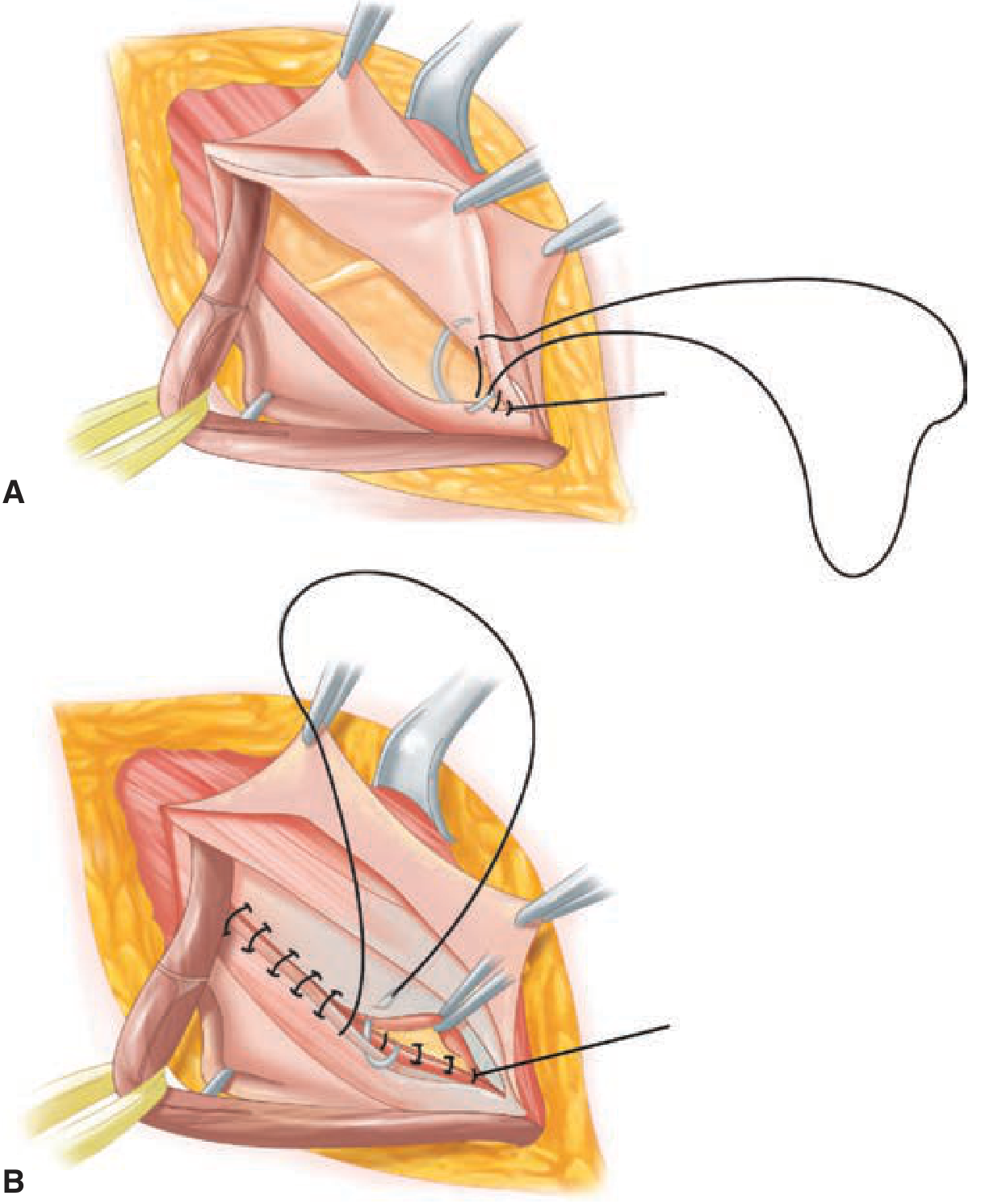
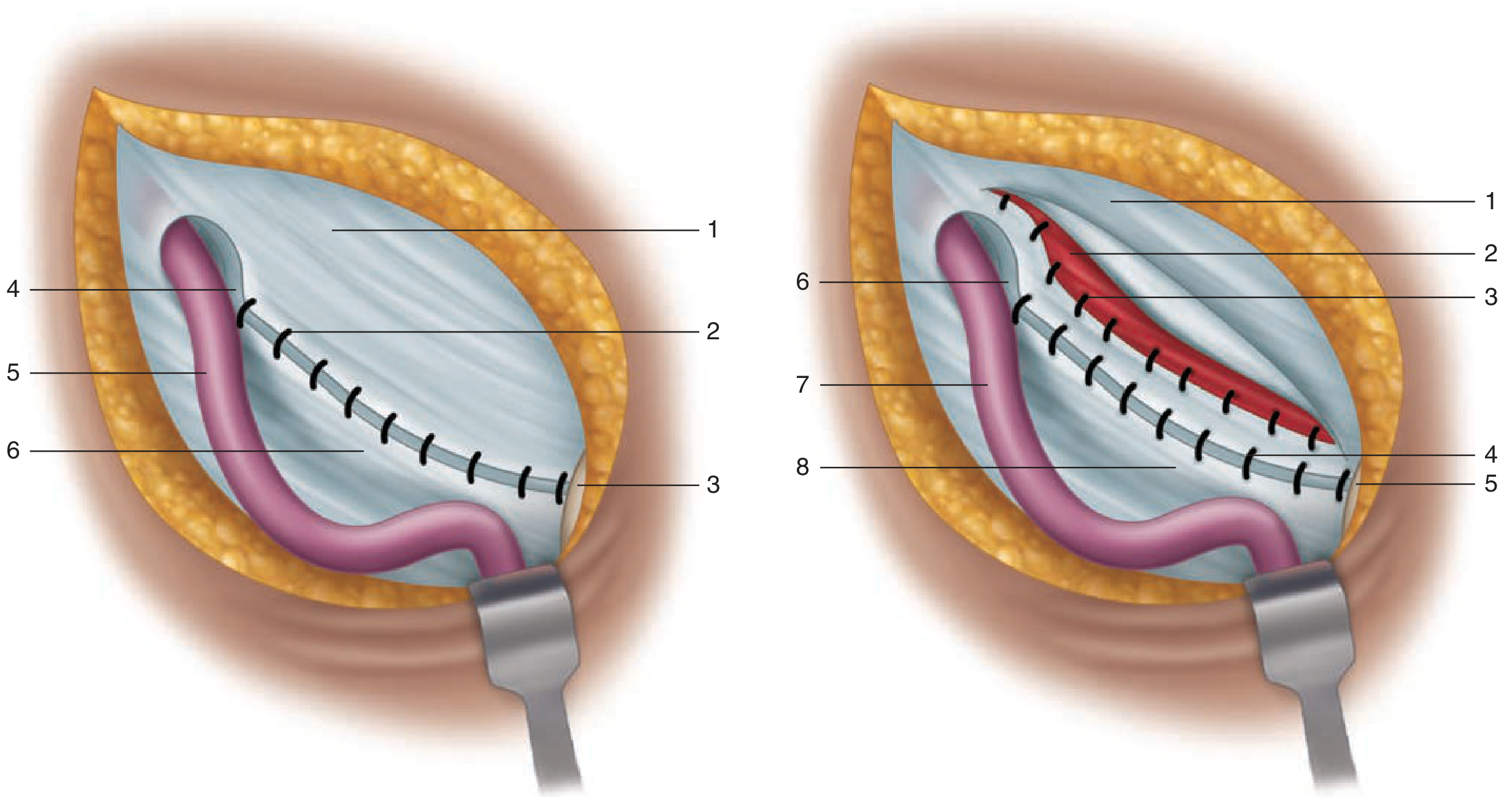
Figure 15. Shouldice repair. A: The iliopubic tract is sutured to the medial flap of the transversalis fascia and the internal oblique/transversus muscles (1st suture line). B: The second suture line reverses back toward the pubic tubercle. Two additional suture lines complete the four-layer repair.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-16)
The Four Layers of Shouldice Repair - Memorize This:
| Layer | What is Sutured | Direction |
|---|
| 1st (most posterior) | Lateral flap of transversalis fascia to medial flap (+ iliopubic tract) | Pubic tubercle → deep ring |
| 2nd | Medial flap of transversalis fascia to lateral (completing double-breasting) | Deep ring → pubic tubercle |
| 3rd | Internal oblique to inguinal ligament | Pubic tubercle → deep ring |
| 4th | Return suture - more of internal oblique to inguinal ligament | Deep ring → pubic tubercle |
All four layers use continuous non-absorbable monofilament (Prolene or Ethilon 2-0) suture.
Why is double-breasting of transversalis fascia important?
The transversalis fascia is the floor of the inguinal canal. Simply suturing it side-to-side creates a single-layer repair that may fail. Overlapping (double-breasting) creates two reinforcing layers, mimicking the way coats are buttoned - each layer supports the other.
3.4 McVay (Cooper's Ligament) Repair
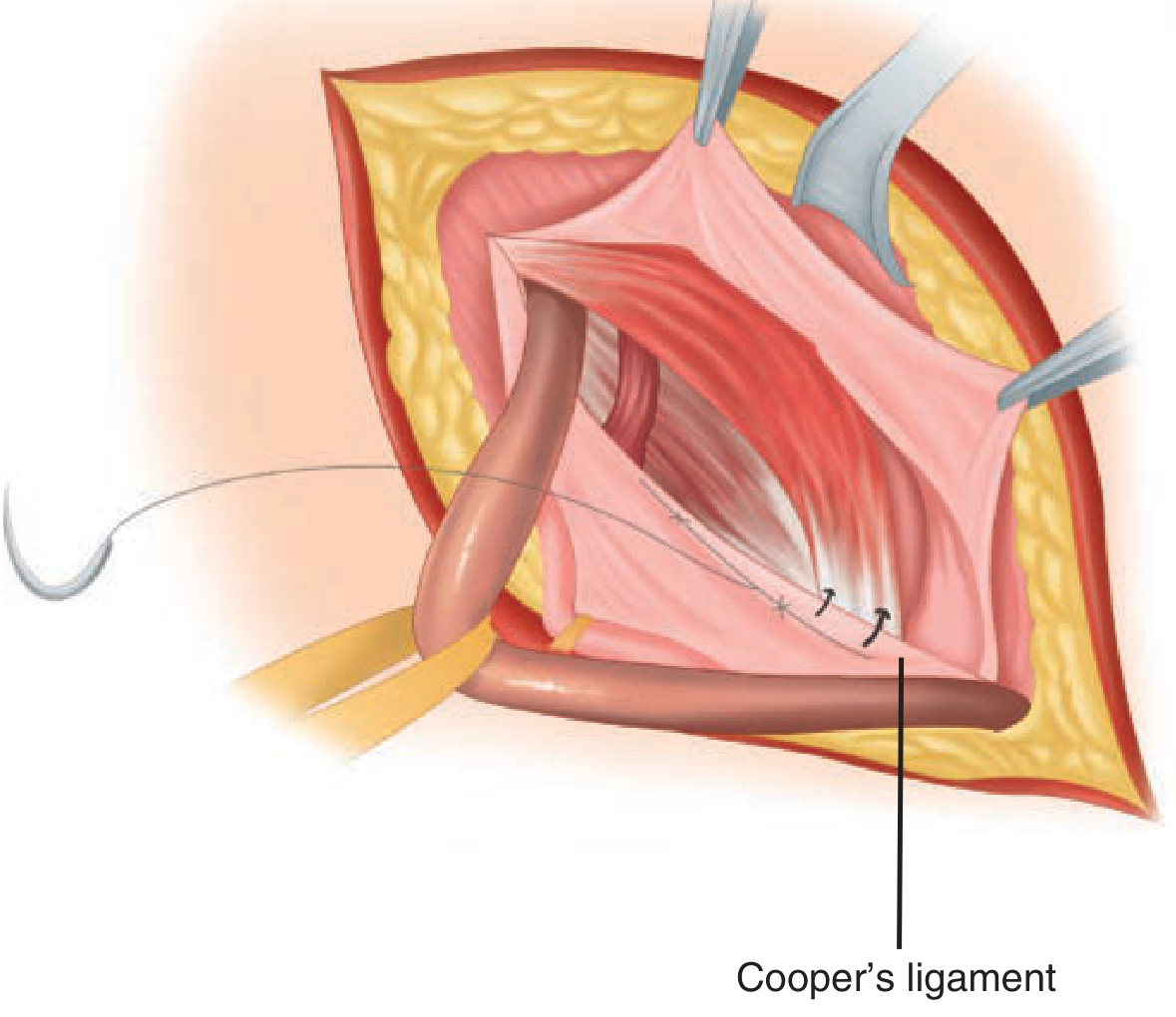
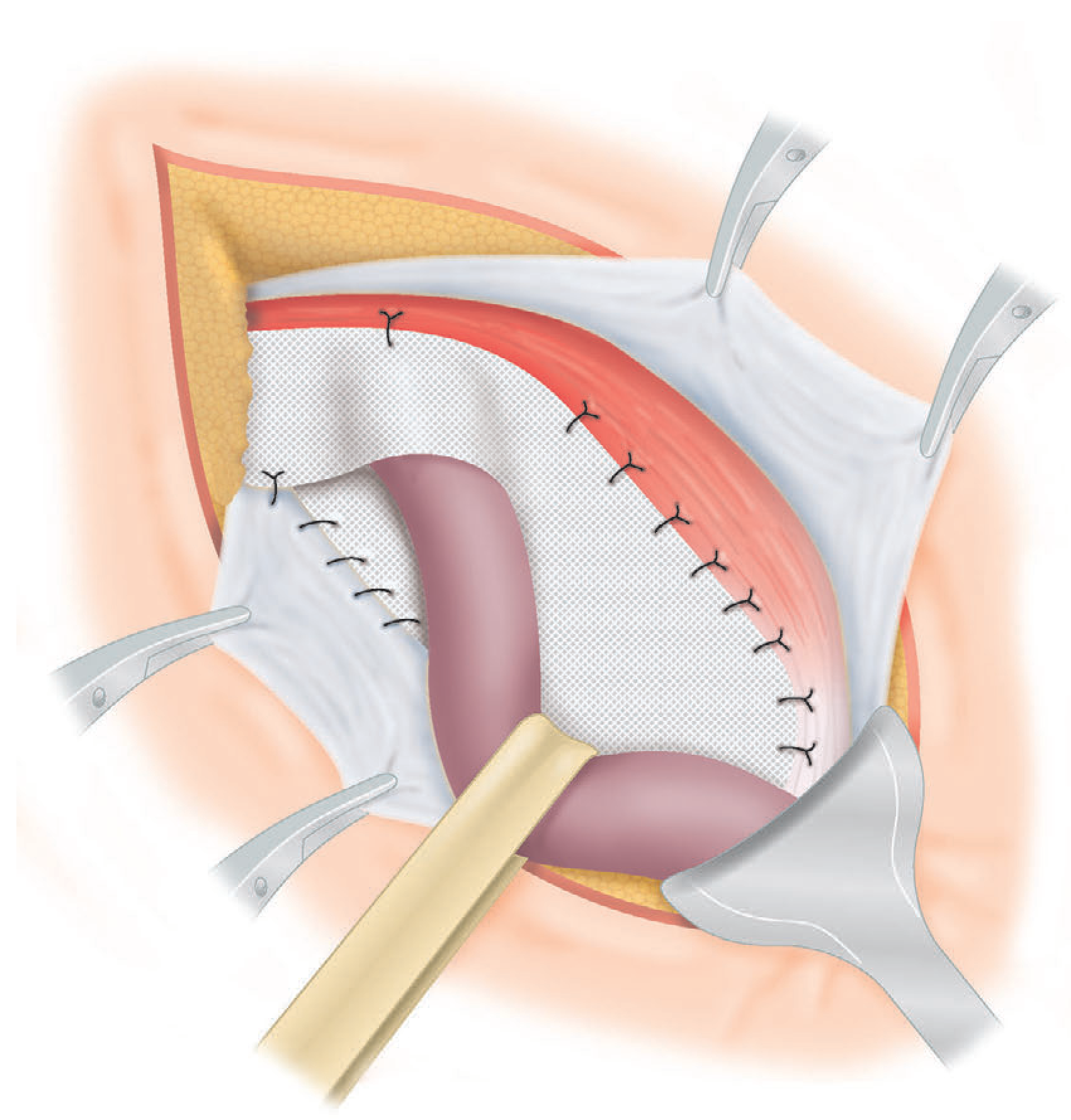
Figure 16. McVay (Cooper's ligament) repair. The conjoint tendon is sutured to the pectineal (Cooper's) ligament on the superior pubic ramus. This is the only suture repair that also closes the femoral ring.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-17)
McVay Repair - Key Points:
| Feature | Detail |
|---|
| Principle | Conjoint tendon → Cooper's (pectineal) ligament (not inguinal ligament) |
| Unique advantage | Closes the femoral ring → repairs femoral hernia |
| Indication | Femoral hernia; large direct hernia; recurrent hernia (open) |
| Limitation | Very high tension → requires mandatory relaxing incision |
| Relaxing incision | Vertical incision in anterior rectus sheath allowing conjoint tendon to slide down. Defect covered by posterior rectus sheath. |
| Transition suture | Between the Cooper's ligament sutures and the inguinal ligament sutures = the "transition suture" that bridges the femoral ring |
Examiner Q: Why must you perform a relaxing incision with McVay's repair?
A: Suturing the conjoint tendon (at a higher level) down to Cooper's ligament (at the pelvic brim) creates extreme tension - sufficient to tear through the suture line. The relaxing incision in the anterior rectus sheath releases this tension by allowing the entire lower portion of the rectus muscle with attached conjoint tendon to slide inferiorly. The defect in the anterior rectus sheath is covered by the strong posterior rectus sheath underneath, so no new hernia is created.
3.5 Desarda Repair
Figure 17. The Desarda repair. A: The medial leaf of external oblique aponeurosis sutured to the inguinal ligament (1=medial leaf, 2=interrupted sutures, 3=pubic tubercle, 4=abdominal ring, 5=spermatic cord, 6=lateral leaf). B: Undetached strip of external oblique aponeurosis forming the new posterior wall - sutures run along both upper and lower borders.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-18)
Concept of Desarda Repair:
- A 1-2 cm strip of external oblique aponeurosis is isolated, kept attached medially (at pubic tubercle) and laterally (beyond deep ring)
- This strip is NOT detached - it remains physiologically active
- The strip is sutured to the conjoint tendon/internal oblique above and the inguinal ligament below
- When the abdominal muscles contract, the strip actively tightens - providing a physiologically dynamic posterior wall
- Equivalent to Shouldice in outcomes (Fischer's Mastery 8th Ed)
- India: increasingly popular in resource-limited settings where mesh is expensive
3.6 Lichtenstein Tension-Free Mesh Repair
Figure 18. Lichtenstein's repair. A mesh is placed behind the spermatic cord over the inguinal floor. The mesh is slit to wrap around the cord at the deep ring. Sutures fix the mesh to the inguinal ligament inferiorly and conjoint tendon superiorly.
(Bailey & Love's Short Practice of Surgery, 28th Edition - Figure 64.15)
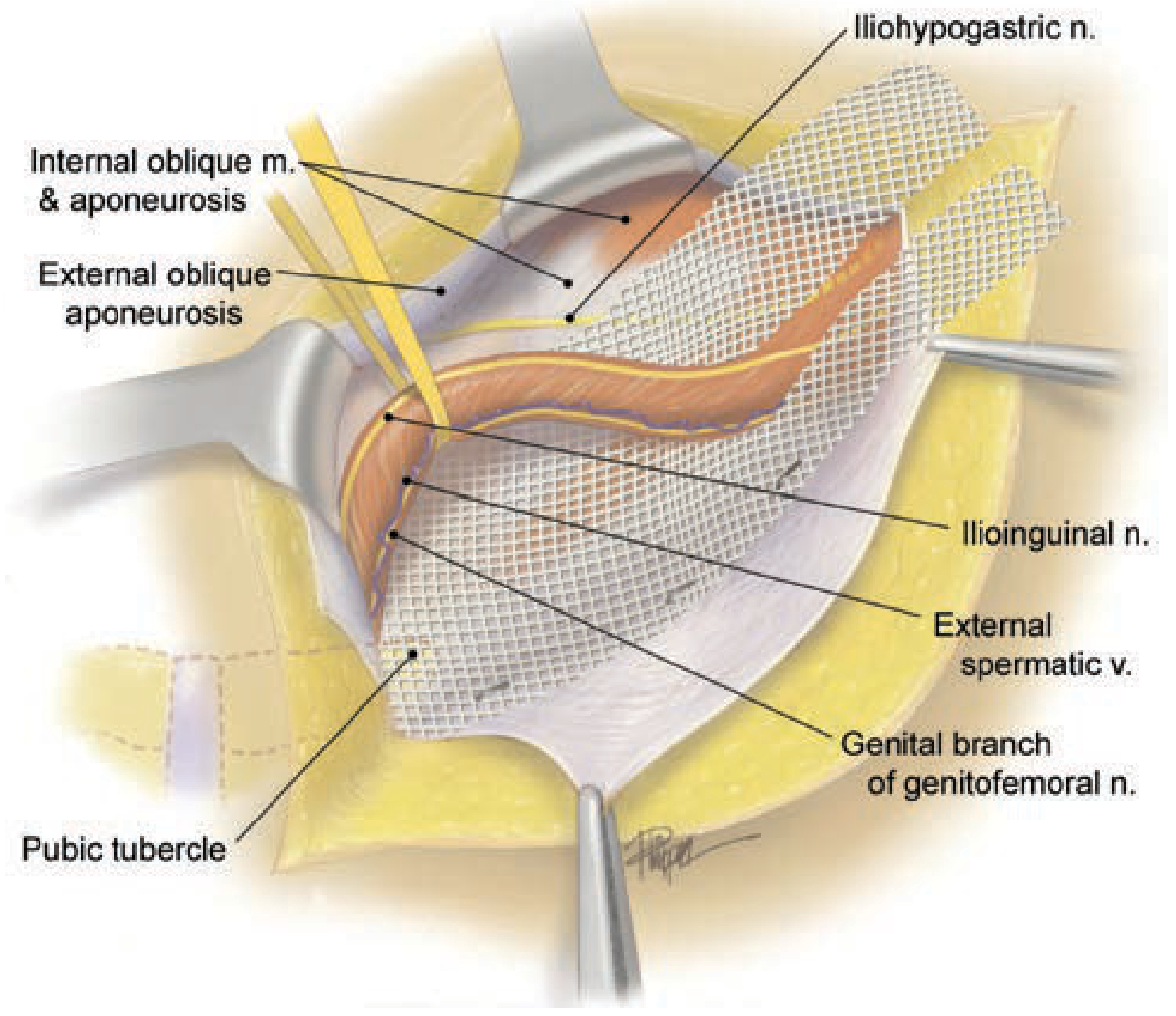
Figure 19. Lichtenstein tension-free hernioplasty. Detailed anatomy showing the mesh position relative to the inguinal ligament, pubic tubercle, cord structures, and Hesselbach's triangle.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-19)
Lichtenstein Mesh - Step-by-Step Operative Notes:
Step 1 - Prepare the mesh:
- Size: Minimum 8×15 cm (ideally 8×15 cm or 7.5×15 cm)
- Make a slit from the lateral end: two tails (upper tail = 2/3 width, lower tail = 1/3 width)
- The slit creates a "V" or "keyhole" for the cord
Step 2 - Position the mesh:
- The mesh slides behind the spermatic cord
- Medial edge is placed BEHIND the anterior rectus sheath, overlapping the pubic tubercle by ≥1.5 cm
- This is the single most important technical point (prevents medial corner recurrence)
Step 3 - Fixation (suture sequence):
MESH FIXATION SEQUENCE (Bailey & Love / EHS 2018):
══════════════════════════════════════════════════
MEDIAL: First suture = medial corner to anterior rectus sheath
(must overlap pubic tubercle by ≥1.5 cm)
↓
INFERIOR: Running suture along inguinal ligament
From pubic tubercle → 2 cm lateral to deep ring
(non-absorbable monofilament = Prolene 2-0)
↓
SUPERIOR: 2-3 interrupted sutures to conjoint tendon/internal oblique
(absorbable suture acceptable here)
↓
LATERAL: Two tails wrap around cord, sutured to each other
New deep ring should admit tip of little finger (~1 cm)
Critical Points:
- ❌ Never suture the mesh to the periosteum of pubic tubercle (pain, osteitis)
- ❌ Never trap the ilioinguinal nerve in a suture
- ❌ Never make the new deep ring too tight (cord ischemia) or too loose (recurrence)
- ✅ Medial corner overlap is the most important single technical detail
3.7 Laparoscopic Repair - Trocar Positions and Mesh Coverage
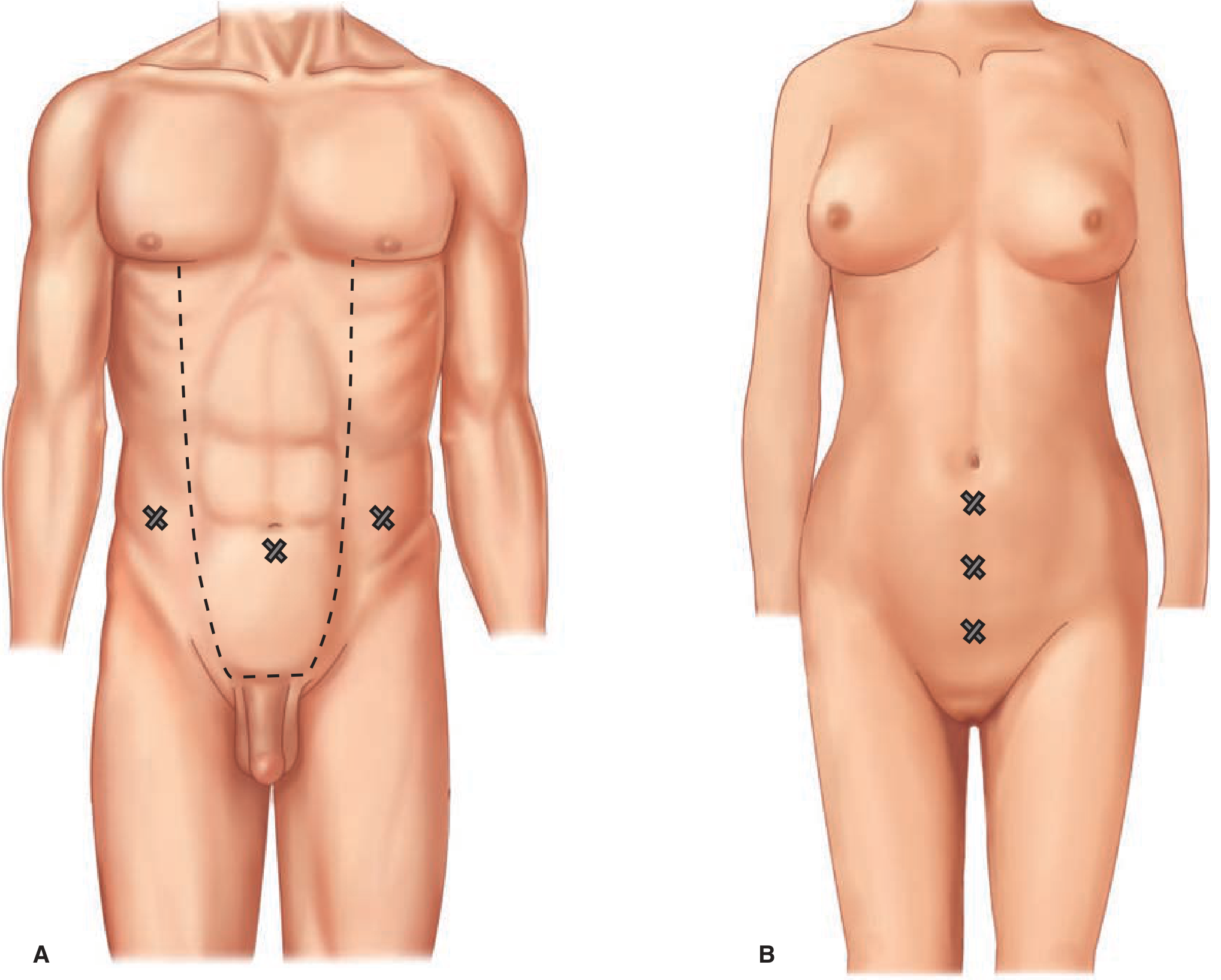
Figure 20. Trocar placement. A: Transabdominal preperitoneal (TAPP) repair - 10 mm umbilical + two 5 mm lateral ports. B: Totally extraperitoneal (TEP) repair - infraumbilical 10-12 mm + midline subumbilical 5 mm + suprapubic 5 mm.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-21)
Figure 21. View of mesh placement in posterior (laparoscopic) repairs. A large mesh (10×15 cm minimum) completely overlaps the entire myopectineal orifice of Fruchaud, covering the sites of direct inguinal, indirect inguinal, and femoral hernias simultaneously.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-22)
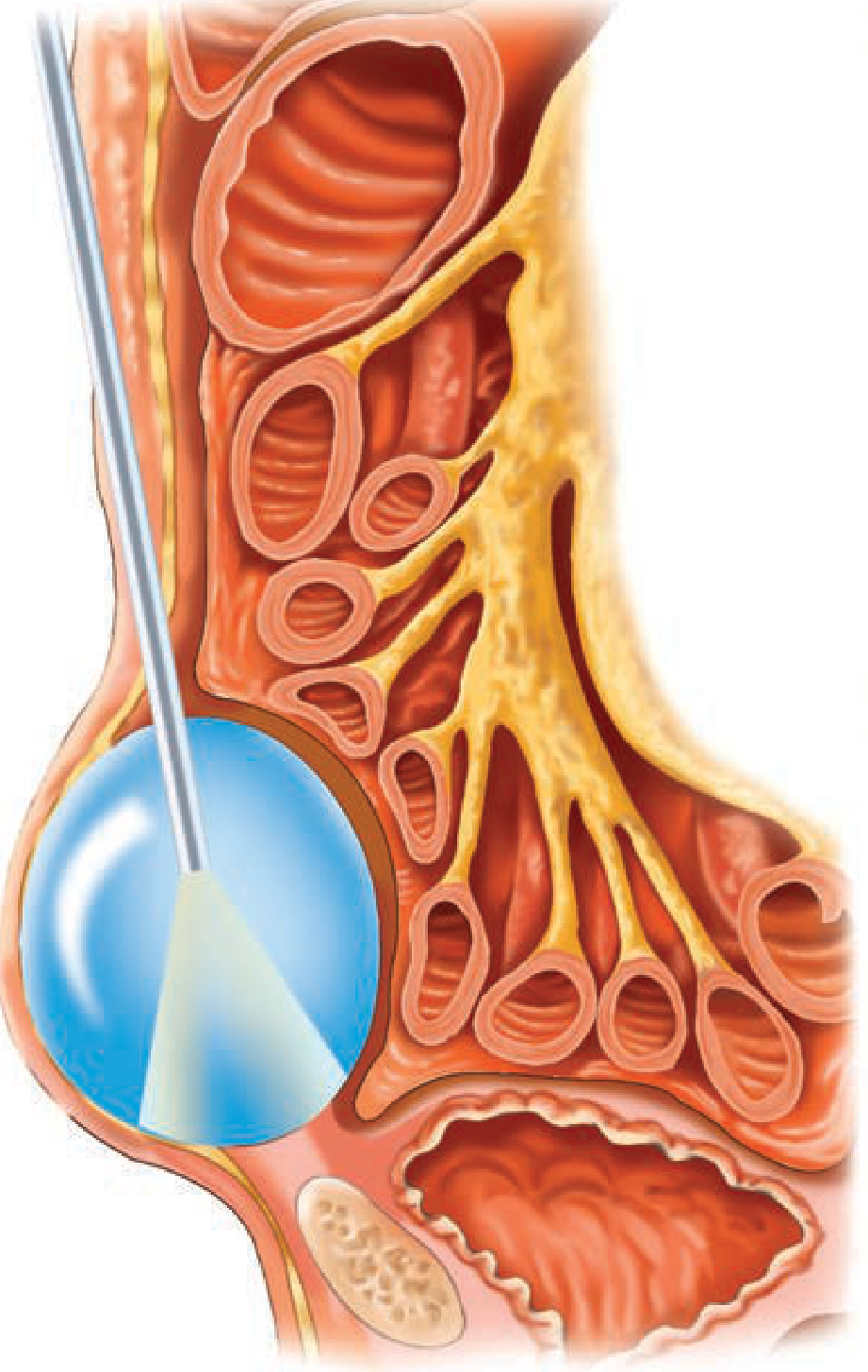
Figure 22. Balloon dissection of the preperitoneal space during TEP repair. The balloon is advanced toward the pubic symphysis under direct laparoscopic vision and inflated to create the working space.
(Schwartz's Principles of Surgery, 11th Edition - Figure 37-23)
TEP vs TAPP - Key Comparison:
| Feature | TEP | TAPP |
|---|
| Peritoneal entry | NO | YES |
| Working space | Preperitoneal only | Peritoneal cavity first, then preperitoneal |
| Gas used | CO₂ in preperitoneal space | Standard pneumoperitoneum |
| Conversion | Can convert to TAPP or open | Can convert to open |
| Risk of bowel injury | Lower (no peritoneal entry) | Present |
| Learning curve | Steeper | Slightly easier |
| Bilateral hernia | Both repaired via same 3 ports | Same |
| Large scrotal hernia | More difficult (sac division needed) | Easier (direct visualization) |
| Intra-abdominal findings | Cannot visualize | Can assess incidental findings |
| EHS recommendation | Both equivalent | Both equivalent |
3.8 Laparoscopic View of Direct Inguinal Hernia and Deep Ring
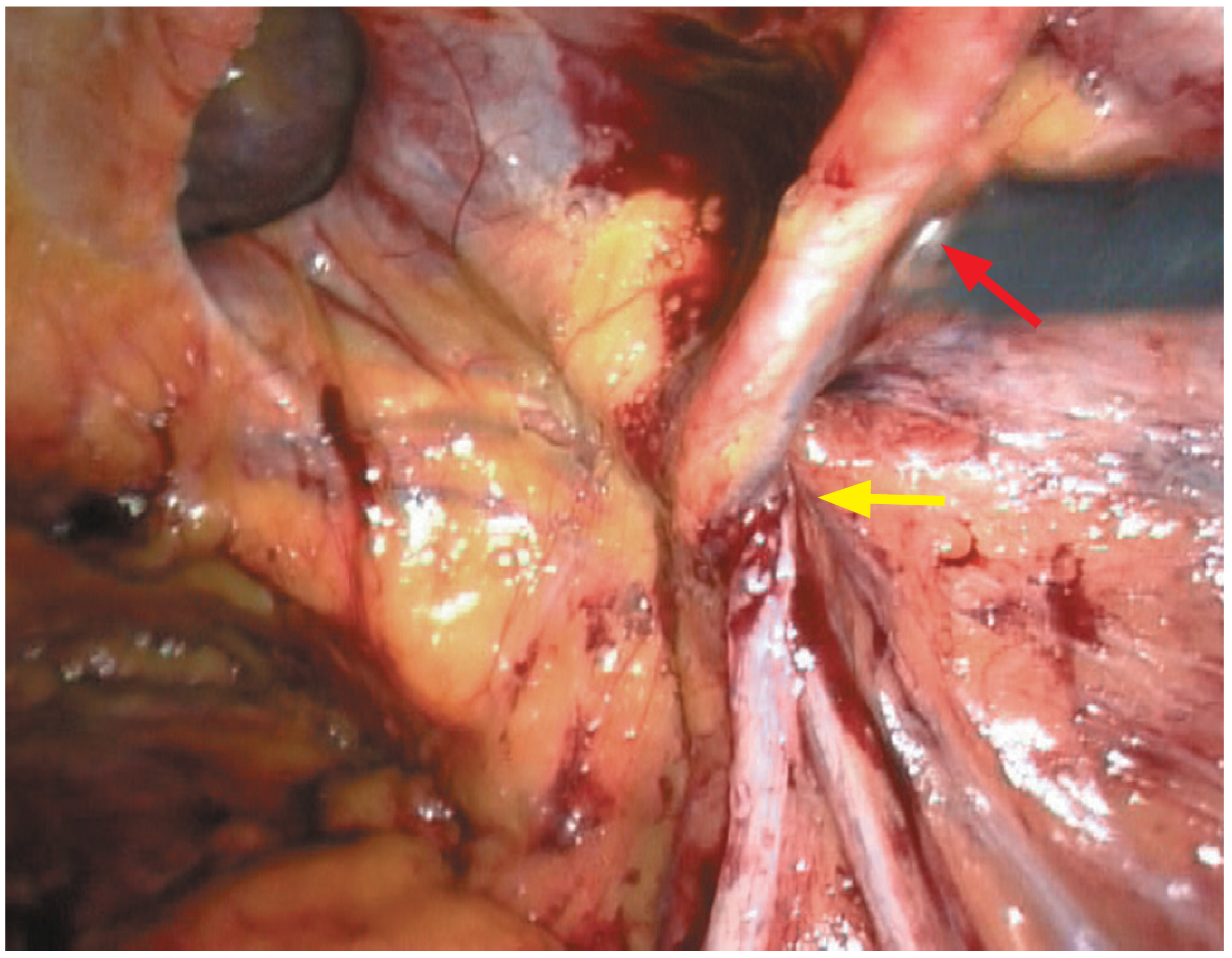
Figure 23. Laparoscopic view of right direct (medial) inguinal hernia. Red arrow = inferior epigastric vessels. Yellow arrow = spermatic cord contents passing through the deep ring laterally. The medial (direct) hernia bulge is clearly medial to the inferior epigastric vessels.
(Bailey & Love's Short Practice of Surgery, 28th Edition - Figure 64.16)
This is the exact laparoscopic view the surgeon sees during TEP/TAPP. The inferior epigastric vessels are the most critical intraoperative landmark. Everything medial to them = direct; everything lateral = indirect.
The Danger Zones in Laparoscopic Hernia Repair (MUST KNOW):
LAPAROSCOPIC VIEW - DANGER ZONES
══════════════════════════════════════════════════════════
PUBIC
SYMPHYSIS
│
COOPER'S LIGAMENT ─────────────────
│ │
╔══════╪═══╗ │
║ DIRECT ║ │
║ HERNIA ║ │
╚══════╪═══╝ │
│ │
INFERIOR ←─────┼─────────┤ ← DEEP RING (indirect)
EPIGASTRIC │ │
VESSELS │ │
│ │
╔═══════════════════════╗
║ TRIANGLE OF DOOM ║
║ (VAS + VESSELS) ║ ← NO TACKS HERE
║ Iliac vessels deep ║ (iliac vessels)
╚═══════════════════════╝
╔══════════════════════════════╗
║ TRIANGLE OF PAIN ║
║ (Lateral, below iliopubic) ║ ← NO TACKS HERE
║ Femoral nerve, LFCN, GF ║ (nerve injury =
╚══════════════════════════════╝ chronic pain)
COOPER'S LIGAMENT: CORONA MORTIS may lie here
→ Never blindly tack Cooper's ligament!
The "Golden Triangle" (safe zone for dissection):
Bounded by the vas deferens medially, the testicular vessels laterally, and the peritoneal reflection superiorly. All important structures converge here - this is where the surgeon must work carefully.
PART 4: FEMORAL RING ANATOMY FOR DIFFERENTIAL DIAGNOSIS
4.1 Femoral Ring Position
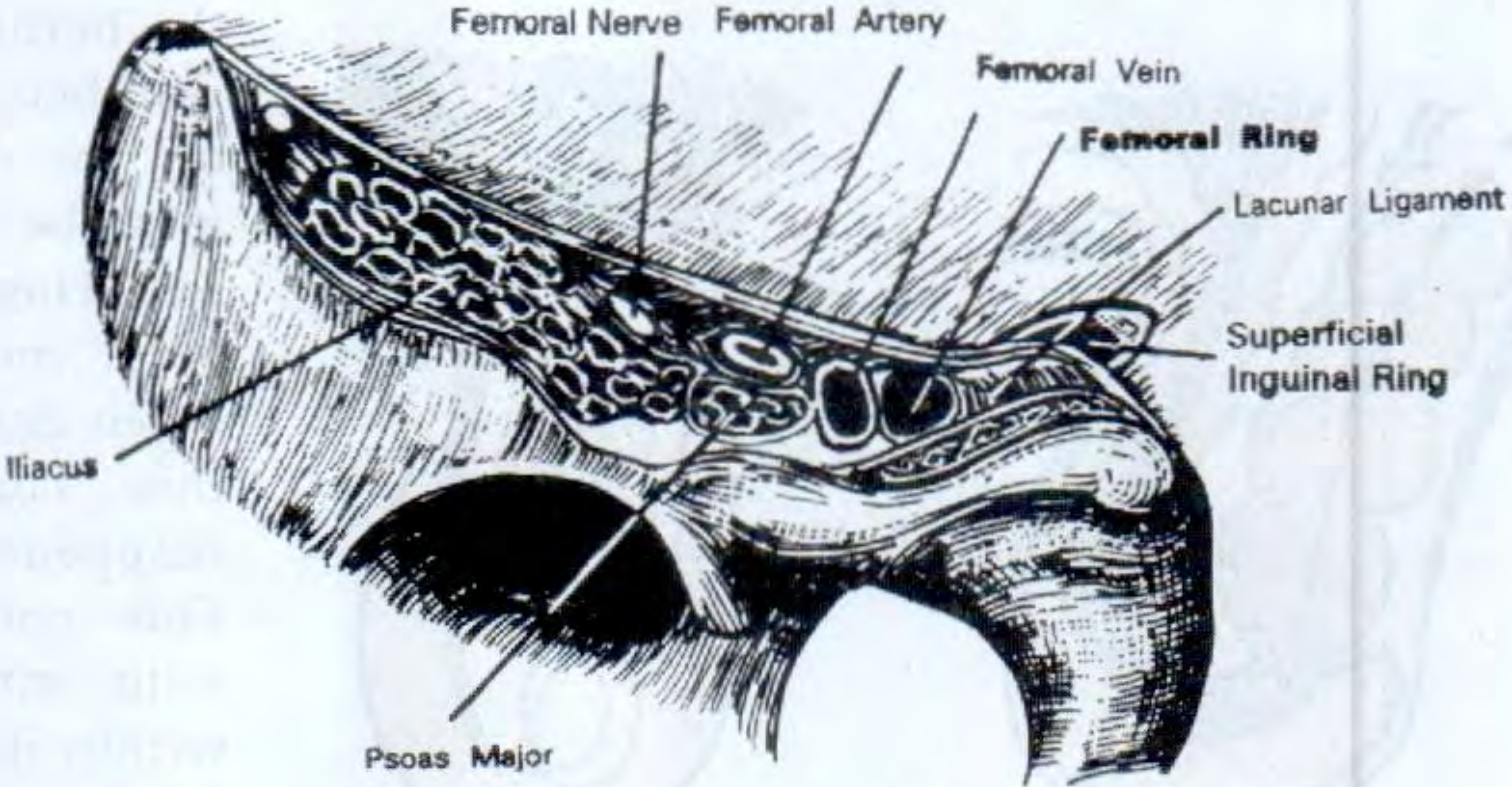
Figure 24. Anatomical representation of the femoral ring position. From lateral to medial: Femoral Nerve - Femoral Artery - Femoral Vein - Femoral Canal (potential space, site of femoral hernia). Mnemonic: NAVY (Nerve-Artery-Vein-Y-fronts/Y-Zone).
(S. Das Manual on Clinical Surgery, 13th Edition - Figure 38.28)
Figure 25. Internal view showing the deep inguinal ring and femoral ring as seen from inside the abdomen. This is the view during TAPP repair. The inferior epigastric vessels, vas deferens, and testicular vessels are all visible.
(S. Das Manual on Clinical Surgery, 13th Edition - Figure 38.29)
Lateral to Medial Arrangement at the Femoral Triangle:
FEMORAL TRIANGLE CONTENTS (Lateral → Medial):
══════════════════════════════════════════════
NERVE | ARTERY | VEIN | EMPTY SPACE (canal)
(N) (A) (V) (AEL)
Mnemonic: "NAVE" = Nerve-Artery-Vein-Empty canal
The EMPTY space (femoral canal) = site of FEMORAL HERNIA
It is the most MEDIAL structure in the femoral sheath
PART 5: CLASSIFICATION WITH DIAGRAMS
5.1 Complete Visual Classification Tree
╔═══════════════════════════════════════════════════════════════╗
║ INGUINAL HERNIA CLASSIFICATION ║
╠═══════════════════════════════════════════════════════════════╣
║ ║
║ BY TYPE BY EXTENT BY CLINICAL STATE ║
║ ──────────── ────────────── ───────────────────────── ║
║ Indirect Bubonocele Reducible ║
║ (Lateral) ↗ Incomplete ↗ Irreducible ║
║ ↘ Complete ↘ Obstructed ║
║ Direct (scrotal) Strangulated ║
║ (Medial) ║
╠═══════════════════════════════════════════════════════════════╣
║ NYHUS GILBERT EHS ║
║ ──────── ─────── ─── ║
║ I 1 L1 / M1 / F ║
║ IIa 2 L2 / M2 ║
║ IIb 3 L3 / M3 ║
║ IIIa 4 P (primary) ║
║ IIIb 5 R (recurrent) ║
║ IIIc 6 (pantaloon) ║
║ IVa-d 7 (femoral) ║
╠═══════════════════════════════════════════════════════════════╣
║ SPECIAL TYPES ║
║ ───────────────────────────────────────────────────────── ║
║ Sliding hernia = viscus forms sac wall ║
║ Pantaloon = direct + indirect same side (straddle IEA)║
║ Richter's = anti-mesenteric wall trapped (no obstruct)║
║ Maydl's = W-hernia; middle loop in abdomen at risk ║
║ Littre's = Meckel's diverticulum in sac ║
╚═══════════════════════════════════════════════════════════════╝
5.2 Nyhus Classification - Visual Summary
NYHUS CLASSIFICATION
════════════════════════════════════════════════════════
TYPE I │ Indirect │ Deep ring NORMAL │ Children │ Herniotomy only
TYPE IIa │ Indirect │ Ring dilated, posterior wall INTACT│ Herniorrhaphy
TYPE IIb │ Indirect │ Ring dilated, wall ENCROACHED │ Mesh preferred
TYPE IIIa│ Direct │ Floor defect (any size) │ Mesh repair
TYPE IIIb│ Indirect │ Large ring + FLOOR DEFECT │ Mesh (lap pref)
│ │ Sliding + Pantaloon included │
TYPE IIIc│ Femoral │ Through femoral ring │ Mesh (McVay/TEP)
TYPE IV │ Recurrent│ IVa=direct, IVb=indirect, │ Opposite approach
│ │ IVc=femoral, IVd=combination │ (lap after open)
════════════════════════════════════════════════════════
Surgical principle: TYPE I = NO MESH; TYPE II-IV = MESH REPAIR
PART 6: INVESTIGATIONS WITH IMAGES
6.1 Investigation Algorithm
CLINICAL EXAMINATION
│
┌────┴──────────────────────┐
DIAGNOSIS DIAGNOSIS UNCERTAIN
CONFIRMED (occult hernia, atypical)
│ │
No investigation ULTRASOUND (dynamic)
needed for fit │
patient Positive → Confirm
Negative or equivocal
│
CT SCAN (with Valsalva)
│
Still unclear
│
MRI (athletic pubalgia)
Herniography (historical)
6.2 What Ultrasound Shows:
- Bowel loops entering the inguinal canal (peristalsis visible) = enterocele
- Omentum (echogenic fat) = epiplocele
- Patent processus vaginalis = communicating hydrocele / potential hernia
- Dynamic ultrasound with Valsalva/standing increases sensitivity for occult hernia to ~97%
- Differentiates: lipoma of cord (no communication with abdomen), lymph node (solid, no cough impulse on USS), varicocele (venous structures)
6.3 CT Scan Findings in Hernia:
- Bowel or fat in the inguinal canal
- Thickened/edematous hernia sac wall (obstruction)
- Free air (perforation in strangulation)
- "Whirlpool sign" (mesenteric twisting = strangulation)
- Identifies sliding viscus (cecum/sigmoid) to plan operation
PART 7: MANAGEMENT ALGORITHM WITH IMAGES
7.1 Comprehensive Management Flowchart
INGUINAL HERNIA DIAGNOSED
│
┌──────┴───────────┐
ELECTIVE EMERGENCY
│ (obstruction/
│ strangulation)
│ │
├─Asymptomatic ├─RESUSCITATE
│ direct, elderly → │ (IV fluid, NG tube,
│ WATCHFUL WAITING │ antibiotics, catheter)
│ │
└─All others → └─OPEN SURGERY
OPTIMIZE first │
(COPD, BPH, Viable bowel?
constipation, YES → Reduce + repair
DM, smoking) NO → Resect + repair
│ Contaminated?
CHOICE OF OP YES → Non-mesh (Shouldice)
│ NO → Mesh acceptable
┌──────┴─────────────────────────┐
│ │
OPEN LAPAROSCOPIC
│ │
Lichtenstein TEP (no peritoneal entry)
(gold standard) TAPP (enter peritoneum)
│ │
Shouldice INDICATIONS FOR LAPAROSCOPIC:
(non-mesh if • Bilateral (preferred)
infection) • Recurrent after anterior
• Occupation demands quick return
• Obese patient
│
LOCAL ANAESTHESIA → preferred for high-risk/elderly
SPINAL → alternative
GENERAL → mandatory for laparoscopic
PART 8: COMPLICATIONS WITH CLINICAL IMAGES
8.1 Strangulation - Clinical and Pathological Features
STRANGULATION TIMELINE
═══════════════════════════════════════════════════
Hour 0-6: Venous obstruction → congestion → edema
Hour 6-12: Arterial occlusion → ischemia begins
Hour 12-24: Mucosal death → bacterial translocation
Hour 24-48: Full-thickness necrosis → perforation
→ peritonitis → sepsis → death
═══════════════════════════════════════════════════
Clinical Signs (in sequence):
1. Sudden severe pain at hernia site
2. Hernia becomes tense, irreducible
3. Cough impulse disappears
4. Vomiting (reflex then obstructive)
5. Absolute constipation
6. Abdominal distension
7. Fever, tachycardia, hypotension (systemic toxicity)
8. Overlying skin: erythema → dusky → necrosis
═══════════════════════════════════════════════════
NEVER attempt vigorous manual reduction of a
strangulated hernia! Reduction en masse = danger.
Bowel Viability Criteria (Intraoperative):
| Sign | Viable | Non-Viable |
|---|
| Color | Pink/red | Black, green, purple |
| Peristalsis | Present | Absent |
| Mesenteric pulsation | Present | Absent |
| Tissue consistency | Firm | Friable, soft |
| Odor | Normal | Foul/gangrenous |
| After warm saline wrap (5 min) | Improves | No improvement |
Management Principle for Non-Viable Bowel:
Resect with adequate margins (minimum 30 cm from visible ischemia on each side). Maydl's hernia pitfall: Always pull out and inspect the intermediate intra-abdominal loop - it may be gangrenous even if the loops in the sac look pink.
PART 9: COMPLETE VIVA SECTION (IMAGE-BASED)
9.1 Image Viva Questions
Image 1: Show Figure 2 (Direct/Indirect/Femoral Hernia Relationships)
Q: Looking at this image, identify the three types of groin hernia and their exit points.
A:
- Indirect inguinal hernia: Exits through the deep inguinal ring, which is a defect in the transversalis fascia, lateral to the inferior epigastric artery. The hernia follows the path of testicular descent and lies within the coverings of the spermatic cord.
- Direct inguinal hernia: Exits through Hesselbach's triangle, directly forward through the posterior wall of the inguinal canal, medial to the inferior epigastric artery. It lies adjacent to but outside the cord.
- Femoral hernia: Exits through the femoral ring, which is below the inguinal ligament, medial to the femoral vein. It is below and lateral to the pubic tubercle.
Image 2: Show Figure 9 (Three-Finger Examination)
Q: Demonstrate this examination technique and explain what each finger position represents.
A: This is Zieman's three-finger test for differentiating groin hernias. Place the thenar eminence on the ASIS. The index finger now points to the deep ring (indirect hernia site), the middle finger to Hesselbach's triangle (direct hernia site), and the ring finger to the femoral ring (femoral hernia site). Ask the patient to cough. The finger that receives the expansile impulse identifies the hernia type.
Image 3: Show Figure 23 (Laparoscopic View of Direct Hernia)
Q: Identify the structures labeled with red and yellow arrows. What operation is being performed?
A: The red arrow points to the inferior epigastric vessels (a key landmark separating direct from indirect hernia). The yellow arrow points to the spermatic cord (testicular vessels and vas deferens) passing through the deep ring laterally. The direct hernia bulge is visible medial to the IEA. This is a laparoscopic view during TEP or TAPP repair - the surgeon is viewing from inside the preperitoneal space looking at the posterior aspect of the anterior abdominal wall.
Image 4: Show Figure 21 (Mesh Covering Myopectineal Orifice)
Q: What is the significance of this mesh position? What principle does it apply?
A: This shows a large mesh (10×15 cm) placed in the preperitoneal space, covering the entire myopectineal orifice of Fruchaud. Fruchaud's concept (1956) was that ALL three types of groin hernia (indirect inguinal, direct inguinal, and femoral) emerge through this single large oval defect in the abdominal wall. By placing one large mesh that covers this entire orifice, the surgeon simultaneously prevents all three types of groin hernia. This is the anatomical basis for TEP and TAPP preperitoneal mesh repair. The mesh is held in place by the intraperitoneal pressure itself (no fixation needed for medium hernias per EHS 2018).
Image 5: Show Figure 22 (Balloon Dissection TEP)
Q: What is happening in this image? What structure is being created?
A: This shows balloon dissection of the preperitoneal space during TEP (totally extraperitoneal) inguinal hernia repair. The balloon dissector has been inserted through the infraumbilical incision, through the anterior rectus sheath, under the rectus muscle, and is being inflated toward the pubic symphysis to bluntly create the preperitoneal working space. The balloon separates the peritoneum from the posterior surface of the anterior abdominal wall, creating the space in which the mesh will be deployed. Once the balloon is removed, CO₂ is insufflated to maintain this space. Trocar placement follows.
9.2 Operative Viva - Step-by-Step Questions
Q: You are about to perform Lichtenstein repair. The patient is draped. Walk me through the operation from incision to closure.
- Incision: Oblique skin crease incision 2 cm above and parallel to medial half of inguinal ligament, 6-8 cm. Deepen through skin and Camper's fascia.
- Scarpa's fascia: Divide, note superficial epigastric vessels (ligate or cauterize if cut).
- External oblique aponeurosis: Identify superficial ring medially. Make a small opening with scissors and extend along fiber direction (downward-medial direction) from lateral to the superficial ring, being careful to open slightly above the inguinal ligament.
- Protect ilioinguinal nerve: Identify it on the anterior surface of the cord - gently sweep it out of the way.
- Identify iliohypogastric nerve: Runs superior to the canal - protect.
- Develop the cord: Pass a finger under the cord at the pubic tubercle, encircle with a Penrose drain. Retract the cord upward.
- Identify the hernia: Inspect both the anteromedial cord surface (indirect sac) and the inguinal floor (direct hernia). Both may coexist.
- Herniotomy (indirect sac): Separate sac from cord by meticulous dissection. Open sac. Reduce contents. Transfixion suture at the neck (deep ring level) with 2-0 Vicryl. Excise excess sac.
- Direct hernia: Invert and suture closed; or simply reduce.
- Place mesh: Cut an 8×15 cm polypropylene mesh. Make a slit 1/3 from the lateral edge (two tails). Slide mesh posterior to cord, medial edge tucked behind the anterior rectus sheath, overlapping pubic tubercle by ≥1.5 cm.
- Fix mesh - inferior edge: Running non-absorbable (Prolene 2-0) from medial to lateral along inguinal ligament to 2 cm lateral to deep ring.
- Fix mesh - superior edge: 2-3 interrupted sutures to conjoint tendon/internal oblique (Vicryl 2-0).
- Reform deep ring: Wrap tails around cord, suture tail to tail; new ring should admit fingertip (~1 cm).
- Cord back in place.
- Close external oblique: Running Vicryl 2-0 from lateral to medial.
- Close Scarpa's fascia: Interrupted Vicryl 3-0.
- Skin closure: Continuous subcuticular Monocryl 3-0 or staples.
9.3 Ward Round Viva
Q: Your patient had a Lichtenstein repair yesterday. He now complains of severe right scrotal swelling and pain at 8 hours post-op. What do you think and what will you do?
Differential diagnosis:
- Reactionary hemorrhage → scrotal hematoma (most common) - swollen, bruised, tense, tender scrotum
- Ischemic orchitis - begins at 24-72 hours, testis swells and becomes tender
- Wound hematoma (separate from scrotal)
Assessment: Vital signs (tachycardia, BP drop = significant hemorrhage). Examine the scrotum: Is it expanding rapidly? Is there a swollen testis?
Management of hematoma:
- Small/moderate: Ice pack, scrotal elevation, close observation, analgesia, IV fluids
- Large/expanding: Return to theater for wound exploration and hemostasis
Ischemic orchitis: Usually begins day 2-3 post-op. Painful tender swollen testis. Due to damage or thrombosis of the cremasteric vessels or pampiniform plexus (often from excessive dissection). Treatment: NSAIDs, elevation, reassurance. Most resolve; ~0.5% progress to testicular atrophy. Inform the patient.
PART 10: RAPID REVISION - IMAGE SUMMARY TABLE
Collected Textbook Images for Examination
| Image | Content | Source | Clinical Relevance |
|---|
| Fig. 1 | All hernia sites | Bailey & Love | Taxonomy of hernias |
| Fig. 2 | Direct/Indirect/Femoral relationships | Bailey & Love | Most important anatomy image |
| Fig. 3A-C | Superficial inguinal dissections (male, female, ligament) | Fischer's Mastery | Canal anatomy at different levels |
| Fig. 4 | Deep inguinal region - serial dissections | Fischer's Mastery | Deep ring, iliopubic tract, layers |
| Fig. 5 | Hesselbach's triangle - hernia types | Fischer's Mastery | Direct vs indirect distinction |
| Fig. 6 | Femoral canal and sheath | Fischer's Mastery | Femoral hernia anatomy |
| Fig. 7 | Corona mortis (anomalous obturator artery) | Fischer's Mastery | Laparoscopic danger zone |
| Fig. 8A | Testicular descent stages | Thieme Atlas | Embryology of indirect hernia |
| Fig. 8B | Spermatic cord coverings | Thieme Atlas | Embryological anatomy |
| Fig. 9 | Zieman's three-finger examination | Thieme Atlas | Clinical examination technique |
| Fig. 10 | Inguinal vs femoral hernia location | Thieme Atlas | Clinical differentiation |
| Fig. 11 | Clinical photograph of inguinal hernia | Bailey & Love | Standing examination |
| Fig. 12 | Infant inguinal hernia | Schwartz | Pediatric hernia |
| Fig. 13 | Bassini's original 1890 diagram | Bailey & Love | Historical operative anatomy |
| Fig. 14 | Open hernia repair layers | Schwartz | Open operative approach |
| Fig. 15 | Shouldice repair - four layers | Schwartz | Non-mesh tissue repair |
| Fig. 16 | McVay Cooper's ligament repair | Schwartz | Femoral hernia repair |
| Fig. 17 | Desarda repair | Schwartz | Physiological tissue repair |
| Fig. 18 | Lichtenstein repair - cross section | Bailey & Love | Gold standard mesh repair |
| Fig. 19 | Lichtenstein hernioplasty - detailed | Schwartz | Mesh fixation technique |
| Fig. 20 | TAPP/TEP trocar placement | Schwartz | Laparoscopic port sites |
| Fig. 21 | Mesh over myopectineal orifice | Schwartz | Fruchaud's principle |
| Fig. 22 | Balloon dissection - TEP | Schwartz | Preperitoneal space creation |
| Fig. 23 | Laparoscopic view - direct hernia | Bailey & Love | Intraoperative anatomy |
| Fig. 24 | Femoral ring - NAVY arrangement | S. Das | Femoral triangle anatomy |
| Fig. 25 | Deep ring + femoral ring - inside view | S. Das | Laparoscopic perspective |
FINAL EXAMINATION CHECKLIST
Before Entering the Examination Hall:
Anatomy (Memorize):
Clinical (Practice):
Classification (Verbatim):
Operations (Step-by-step):
Complications:
Complete image-rich guide compiled from Bailey & Love's Short Practice of Surgery 28th Ed, Schwartz's Principles of Surgery 11th Ed, Fischer's Mastery of Surgery 8th Ed, S. Das Manual on Clinical Surgery 13th Ed, and Thieme General Anatomy & Musculoskeletal System Atlas.