Prophylactic anti epileptic in hemorrhagic stroke
Reading File
Finding Sources
Finding Sources
Searching PubMed
prophylactic antiepileptic drugs intracerebral hemorrhage
Reading Article
PMID: 39707127
Reading Article
PMID: 36337029
Finding Sources
Finding Sources
Reading File
Reading Article
PMID: 34286461
I now have sufficient, high-quality evidence to deliver a comprehensive answer.
Prophylactic Antiepileptic Drugs in Hemorrhagic Stroke (ICH)
Current Recommendation: Avoid Routine Prophylaxis
The evidence strongly and consistently argues against routine prophylactic antiseizure medication (ASM) in spontaneous intracerebral hemorrhage (ICH):
- The 2025 Neurocritical Care Society (NCS) Clinical Practice Guideline (Frontera et al., PMID 39707127) — the most current authoritative guidance — conducted a systematic review and meta-analysis across 15 studies and concluded:
"We suggest avoidance of prophylactic ASM in hospitalized adult patients with acute nontraumatic ICH." (Weak recommendation, very low quality of evidence)
- Meta-analyses showed no significant reduction in early seizures (≤14 days), late seizures (>14 days), or mortality with prophylactic ASM.
- Prophylactic ASMs were associated with increased adverse events and a higher relative risk of poor functional outcomes at 90 days.
This is corroborated by Rosen's Emergency Medicine, which states: "In ICH, the prophylactic use of anticonvulsants has been associated with worse neurologic outcomes, and we concur with current guidelines that do not recommend their routine use." — Rosen's Emergency Medicine
If Prophylaxis Is Used Despite the Above
The 2025 NCS guidelines provide conditional guidance for situations where a clinician chooses to use ASMs:
| Question | Recommendation |
|---|---|
| Which agent? | Levetiracetam (LEV) preferred over phenytoin/fosphenytoin (PHT/fPHT) (weak recommendation, very low evidence) |
| How long? | Short duration ≤7 days preferred over >7 days (weak recommendation, very low evidence) |
Point estimates in comparisons tended to favor LEV, though no statistically significant difference in early seizures or adverse events was detected between LEV and PHT.
Why LEV Over Phenytoin?
The 2022 meta-analysis by Fang et al. (PMID 34286461, Neurocritical Care) across 7,609 patients found no significant superiority of LEV over other ASMs in ICH specifically, but:
- Phenytoin is associated with worse cognitive outcomes, drug interactions, and a narrow therapeutic window.
- LEV has a more favorable adverse effect profile, fewer drug interactions, and no requirement for therapeutic drug level monitoring.
- A 2023 meta-analysis (Mota Telles et al., PMID 36337029, Int J Stroke) found PASDs reduced seizures only in studies with continuous EEG monitoring (OR 0.36), but this benefit did not translate into improved functional outcomes — even with newer, less toxic drugs.
When Should Treatment (Not Prophylaxis) Be Given?
Seizures that do occur should be treated promptly:
- Lorazepam 0.1 mg/kg IV (max 4 mg) — first-line to abort an acute seizure
- Followed by a loading dose of LEV (preferred), valproic acid, or fosphenytoin as second-line
Special Note: SAH vs ICH
This guidance applies to spontaneous ICH (parenchymal hemorrhage). Subarachnoid hemorrhage (SAH) has a separate (also evolving) evidence base; routine prophylaxis after SAH is similarly being questioned, but the risk of vasospasm-triggered seizures makes management nuances different.
Summary Table
| Scenario | Recommendation |
|---|---|
| Routine ASM prophylaxis in ICH | Not recommended |
| Drug of choice if ASM used | Levetiracetam |
| Duration if ASM used | ≤7 days |
| Phenytoin/fosphenytoin | Avoid (worse functional outcomes) |
| Treating actual seizures | Benzodiazepine → LEV/valproate |
Key references:
- Frontera JA et al. Neurocrit Care 2025 — NCS 2025 Guideline (PMID 39707127)
- Mota Telles JP et al. Int J Stroke 2023 (PMID 36337029)
- Fang T et al. Neurocrit Care 2022 (PMID 34286461)
Dose of levetiracetam
Finding Sources
Reading File
Reading File
Reading File
Reading File
Levetiracetam Dosing
Adult Dosing by Indication
| Indication | Dose | Route | Notes |
|---|---|---|---|
| Epilepsy (maintenance) | Start 500–1000 mg/day; ↑ by 1000 mg every 2–4 weeks | PO (BD) | Max 3000 mg/day (1500 mg BD) |
| ICH seizure prophylaxis (if used) | 500 mg BD × ≤7 days | PO/IV | Adjust for renal function |
| Status epilepticus (loading) | 20–60 mg/kg IV | IV | Up to max ~4500 mg (Rosen's uses 60 mg/kg max 4500 mg) |
| Status epilepticus (maintenance) | 1000–1500 mg BD | IV/PO | Switch to oral when possible |
Formulations Available
- Oral: Immediate-release tablets (250, 500, 750, 1000 mg), oral solution (100 mg/mL)
- IV: 500 mg/5 mL (100 mg/mL concentrate); infuse over 15 minutes
- Extended-release tablets also available (once-daily dosing)
Renal Dose Adjustment
LEV is 95% renally excreted — dose reduction required in renal impairment:
| CrCl (mL/min) | Dose Adjustment |
|---|---|
| >80 | No change |
| 50–80 | 500–1000 mg BD |
| 30–50 | 250–750 mg BD |
| <30 | 250–500 mg BD |
| Dialysis | Supplemental dose after HD |
Key Pharmacokinetic Points
- Half-life: 6–8 hours (longer in elderly)
- No hepatic metabolism — no CYP interactions, no drug-drug interactions
- Not protein-bound — linear pharmacokinetics across the dosing range
- No need for therapeutic drug level monitoring in routine use (though reference range is ~12–46 mg/L)
— Goodman & Gilman's, Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine 22E
Bp control in ischemic and hemorrhagic stroke
Reading File
Finding Sources
Finding Sources
Searching PubMed
blood pressure management ischemic stroke guidelines
Searching PubMed
blood pressure reduction intracerebral hemorrhage
Finding Sources
Finding Sources
Reading Article
PMID: 40739079
Reading File
Reading File
Reading File
Reading File
Excellent — I now have comprehensive data from multiple sources. Here's the full answer:
Blood Pressure Control in Stroke — Ischemic vs. Hemorrhagic
Part 1: Ischemic Stroke
Pathophysiology of Hypertension in Acute Ischemic Stroke
BP is often reflexively elevated after ischemic stroke as a physiological response to maintain perfusion in the ischemic penumbra. Aggressive lowering is harmful — low BP on arrival (SBP <155, DBP <70, or MAP <100 mmHg) correlates with increased 90-day mortality. Sudden BP reduction can cause neurological deterioration. — Bradley & Daroff's Neurology
Targets
| Clinical Scenario | SBP Target | Action |
|---|---|---|
| Not eligible for thrombolysis/thrombectomy | >220 systolic OR >120 diastolic | Treat only if exceeds these thresholds; reduce by 10–15% initially |
| Eligible for IV thrombolysis (tPA) | Must be <185/110 before giving tPA | Aggressively treat to reach this threshold |
| After IV tPA | Maintain <180/105 for ≥24 hours | Strict control to prevent hemorrhagic transformation |
| After mechanical thrombectomy | <180/105 | Maintain post-procedure |
| DBP >140 mmHg (any situation) | Use IV sodium nitroprusside | Special consideration |
Why Such Permissive Targets Without Thrombolysis?
Multiple major trials (CATIS, ENOS, VENTURE, CHIPIS, COSSACS, INWEST) have all failed to show benefit from BP lowering in acute ischemic stroke without thrombolysis. INWEST even showed harm — higher rates of death/dependency with BP lowering. The permissive approach is justified by the ischemic penumbra concept. — Comprehensive Clinical Nephrology
Preferred Agents (Ischemic Stroke)
- IV labetalol — intermittent bolus (first-line)
- IV nicardipine — continuous infusion (preferred for precise titration)
- IV hydralazine — intermittent doses
- IV sodium nitroprusside — only when DBP >140 mmHg
Avoid: Sublingual nifedipine (unpredictable drops), oral agents with slow onset
Part 2: Hemorrhagic Stroke (ICH)
Why Active BP Lowering IS Indicated
In ICH, elevated BP drives hematoma expansion — the main cause of early neurological deterioration. Active BP reduction limits hematoma growth, reduces perihematomal edema, and improves outcomes.
Targets (AHA/ASA & Current Evidence)
| Scenario | BP Target |
|---|---|
| ICH, SBP 150–220 mmHg, mild–moderate volume (6–19 mL) | Target SBP 140 mmHg |
| ICH, SBP >220 mmHg | Aggressive IV reduction, target SBP 140–180 |
| ICH, very intensive: SBP 110–139 | Not recommended — no added benefit, increased renal adverse events |
| SAH (pre-aneurysm treatment) | SBP <160 mmHg |
| SAH (post-aneurysm treatment) | Do not lower BP |
Goldman-Cecil Medicine: "Systolic blood pressure should be lowered to a target of 140 mmHg to improve 3-month functional outcomes and quality of life. Additional lowering to SBP 110–139 mmHg does not add benefit and is associated with increased renal adverse events."
Key Trial Data (ICH)
| Trial | Target | Patients | Result |
|---|---|---|---|
| INTERACT 2 | SBP <140 vs <180 | 2839 | No significant reduction in death/severe disability; improved functional outcomes on ordinal mRS analysis |
| ATACH 2 | SBP 110–140 vs 140–179 | 1000 | Intensive group had higher renal adverse events, no benefit |
| 2025 Meta-analysis (Reginato et al.) | <140 vs standard | 13,625 (11 RCTs) | Intensive lowering: ↓ poor outcome (mRS 3–6), ↓ mortality, ↓ hematoma enlargement |
The 2025 meta-analysis (PMID 40739079) provides the strongest current evidence supporting intensive BP lowering (target <140 mmHg) in ICH.
Preferred Agents (ICH)
- IV labetalol
- IV nicardipine (preferred — smooth titration, no reflex tachycardia)
- IV clevidipine
- IV enalaprilat
Agents should have rapid onset and short duration to avoid BP lability.
Summary Comparison Table
| Feature | Ischemic Stroke (no thrombolysis) | Ischemic Stroke (+ tPA) | Hemorrhagic Stroke (ICH) |
|---|---|---|---|
| Permissive threshold | >220/120 | >185/110 | Treat if >150 |
| Target | Reduce by 10–15% only | <180/105 after tPA | SBP 140 mmHg |
| Aggressive lowering | Harmful (penumbra) | Required | Beneficial |
| Preferred agent | Labetalol, nicardipine | Labetalol, nicardipine | Nicardipine, labetalol |
| Avoid | Over-lowering | Uncontrolled BP | SBP <110 (renal risk) |
Key references:
- Bradley & Daroff's Neurology in Clinical Practice
- Goldman-Cecil Medicine (22nd Ed.)
- Comprehensive Clinical Nephrology, 7th Ed. — AHA/ASA & ESO guideline comparison table
- Reginato PH et al. Neurocrit Care 2025 (PMID 40739079) — meta-analysis of intensive BP lowering in ICH
Idiopathic intracranial hypertension
Finding Sources
Searching PubMed
idiopathic intracranial hypertension management
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Carotid stenosis and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
carotid stenosis treatment endarterectomy stenting
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data. Let me compile the full answer.
Carotid Stenosis — Overview and Treatment
Epidemiology and Clinical Significance
Atherosclerotic carotid artery disease is responsible for 80% of new noncardioembolic ischemic strokes, primarily via plaque rupture and atheroembolization (not occlusion). Key facts:
- 5–10% of patients >65 years have >50% carotid stenosis; ~1% have ≥75%
- Symptomatic patients have a 5–10× increased stroke risk vs asymptomatic; TIA carries a 20% risk of stroke within 90 days
- Asymptomatic patients outnumber symptomatic by 4:1
- ~90% of stroke risk is attributable to modifiable risk factors
— Fuster & Hurst's The Heart, 15th Ed.
Imaging Diagnosis
| Modality | Role |
|---|---|
| Doppler Ultrasound (DUS) | First-line; sensitivity >90%, specificity >85% for >50% stenosis; cost-effective, no radiation |
| CTA / MRA | Second-line; used when DUS findings are discordant or anatomy is complex |
| Catheter angiography | Reserved as problem-solving tool only; 1% periprocedural stroke risk |
Carotid IMT and total plaque area (TPA) on ultrasound are also used for cardiovascular risk stratification — TPA is as predictive as coronary calcium scoring but cheaper and radiation-free.
Grading of Stenosis
Based on the NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria (% reduction in diameter at the ICA relative to the normal distal ICA):
| Grade | % Stenosis |
|---|---|
| Mild | <50% |
| Moderate | 50–69% |
| Severe | 70–99% |
| Occlusion | 100% |
Treatment
1. Guideline-Directed Medical Therapy (GDMT) — Foundation for ALL patients
GDMT is the cornerstone of treatment for both symptomatic and asymptomatic patients:
- Antiplatelet therapy: Aspirin 75–325 mg/day ± clopidogrel
- Statin therapy: High-intensity statin — target LDL <70 mg/dL
- BP control: Target SBP <140 mmHg (<130 in diabetics)
- HbA1c <7.0% in diabetics
- Smoking cessation
- Weight management, exercise (≥30 min moderate activity × 3/week)
With modern GDMT, the annual stroke risk for asymptomatic patients with significant carotid stenosis is estimated at <1% per year.
2. Revascularization — Carotid Endarterectomy (CEA) vs Carotid Artery Stenting (CAS)
Symptomatic Carotid Stenosis
Symptoms include: TIA, ischemic stroke, or amaurosis fugax ipsilateral to the stenosis.
| Stenosis | Recommendation |
|---|---|
| 70–99% | CEA strongly recommended (NASCET, ECST) — major absolute risk reduction |
| 50–69% | CEA beneficial; benefit is modest and depends on patient risk profile |
| <50% | No benefit from surgery; medical therapy alone |
Timing: CEA should be performed within 2 weeks of a TIA or minor stroke for maximum benefit (risk of stroke is highest in this window).
Key trials:
- NASCET: CEA reduced 2-year ipsilateral stroke rate from 26% → 9% for 70–99% stenosis (absolute risk reduction 17%)
- ECST: Confirmed benefit for 70–99% stenosis
- VA Cooperative Study: Corroborated NASCET findings
Asymptomatic Carotid Stenosis
| Stenosis | Recommendation |
|---|---|
| >70% | CEA reasonable if perioperative risk of stroke/MI/death is <3% (AHA/ASA) — but benefit over modern GDMT is uncertain |
| 50–70% | Medical therapy preferred |
CREST-2 (ongoing) is testing CEA + GDMT vs GDMT alone, and CAS + GDMT vs GDMT alone in asymptomatic patients — results awaited.
3. CEA vs CAS — Comparative Data
| Feature | CEA | CAS |
|---|---|---|
| Standard of care | Yes — well-established | Alternative in selected patients |
| Periprocedural stroke risk | Lower (CREST: 2.3%) | Higher (CREST: 4.3%) |
| Periprocedural MI risk | Higher (CREST: 2.3%) | Lower (CREST: 1.1%) |
| Age preference | Preferred in older patients (>70 yrs) | Better tolerated in younger patients |
| 4-year composite (CREST) | 6.8% | 7.2% (non-inferior) |
Key trials comparing CEA vs CAS:
| Trial | Finding |
|---|---|
| SAPPHIRE | CAS non-inferior to CEA in high-surgical-risk patients |
| SPACE / EVA-3S (European) | CAS inferior to CEA; controversial due to operator experience issues |
| CREST | No significant difference in composite stroke/MI/death at 4 years; CAS had more strokes, CEA had more MIs |
| ICSS (European) | 30-day stroke risk higher with CAS |
Bottom line: In average-risk symptomatic patients, CEA is preferred. CAS is reserved for patients at high surgical risk or with anatomical contraindications to CEA (high cervical lesions, radiation-induced stenosis, restenosis after prior CEA, severe cardiac comorbidities).
4. Transcarotid Artery Revascularization (TCAR)
A newer hybrid technique — stent delivered via direct surgical carotid access with flow reversal to prevent cerebral embolization. Advantages over transfemoral CAS: lower stroke risk. Currently used in high-surgical-risk patients as an alternative to both standard CEA and transfemoral CAS.
Indications Summary
Symptomatic + 70–99% stenosis → CEA (within 2 weeks)
Symptomatic + 50–69% stenosis → CEA (if perioperative risk <6%)
Symptomatic + <50% stenosis → Medical therapy only
Asymptomatic + >70% stenosis → GDMT ± CEA if periop risk <3%
High surgical risk (any) → Consider CAS or TCAR
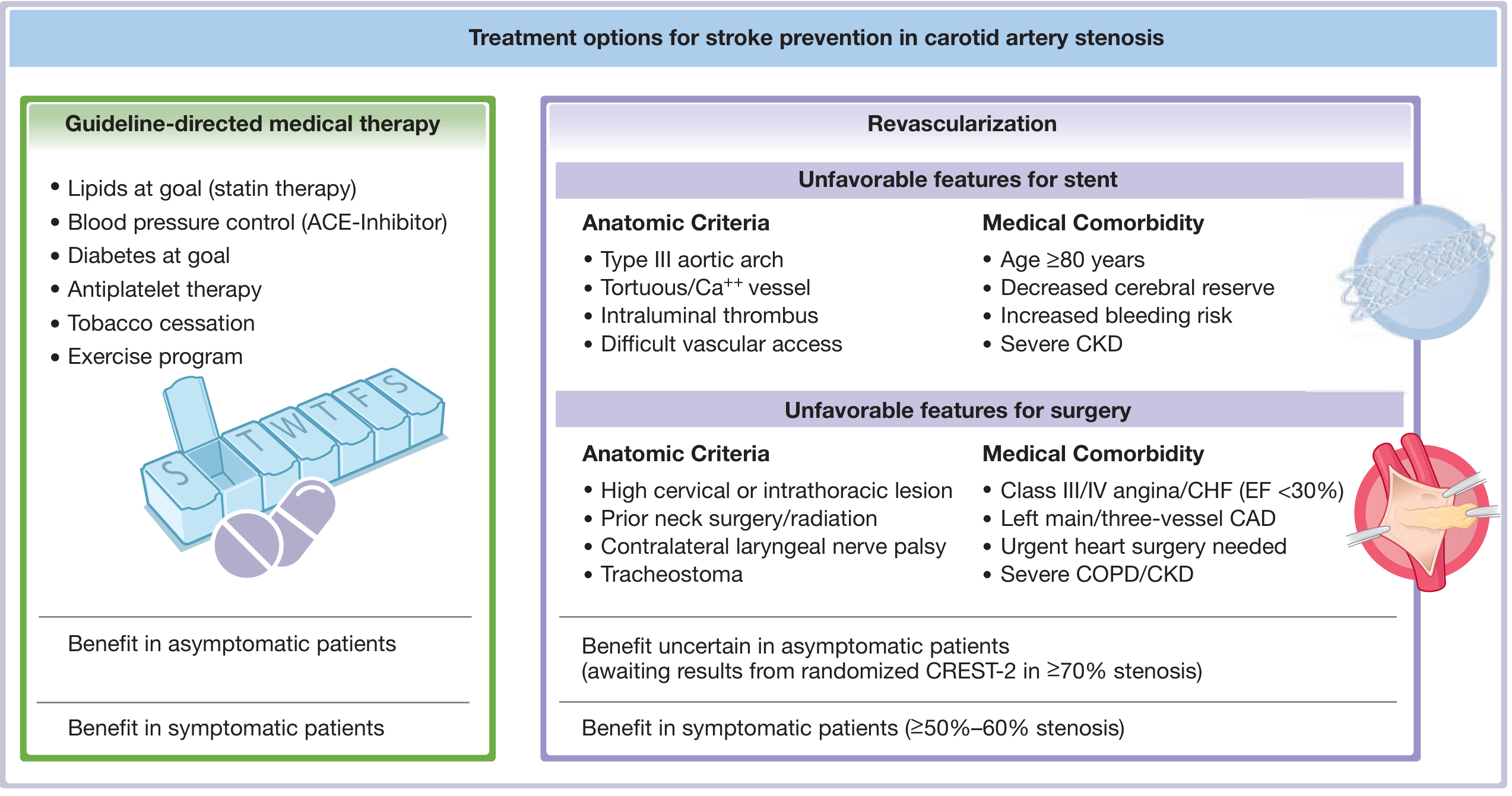
Treatment options for carotid artery stenosis — Fuster & Hurst's The Heart
Sources:
- Fuster & Hurst's The Heart, 15th Ed.
- Bradley & Daroff's Neurology in Clinical Practice
- Grainger & Allison's Diagnostic Radiology
- Paraskevas KI et al. J Vasc Surg 2024 (PMID 37939746) — recent advances in asymptomatic carotid stenosis
CAS
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
3 percent ns in suspected csvt in a 13 yr old with intellectual disability
Reading File
Finding Sources
Finding Sources
Searching PubMed
cerebral sinovenous thrombosis children management anticoagulation
Finding Sources
Finding Sources
Searching PubMed
hypertonic saline cerebral venous thrombosis intracranial hypertension
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have sufficient material to give a thorough, clinically focused answer. This is a nuanced question about a specific clinical decision: should 3% hypertonic saline be used in a 13-year-old with suspected CSVT and intellectual disability (ID)?
3% Hypertonic Saline in Suspected CSVT — 13-Year-Old with Intellectual Disability
This is a high-stakes clinical decision requiring careful reasoning. Here's how to approach it:
Understanding the Problem: Why Is 3% NaCl Being Considered?
3% hypertonic saline (HTS) is being considered presumably because of raised intracranial pressure (ICP) — a recognized complication of CSVT. In CSVT, thrombosis of dural sinuses:
- Increases venous back-pressure → impairs CSF absorption
- Elevates cerebral blood volume
- Can cause hemorrhagic venous infarcts and cerebral edema
Signs of raised ICP in CSVT: papilledema, headache, declining GCS, vomiting, sixth nerve palsy. In a child with intellectual disability, verbal reporting is limited — altered behavior, increased agitation, or sudden functional decline may be the only signs.
Role of 3% Hypertonic Saline in CSVT — Is It Appropriate?
Standard management of raised ICP in CSVT:
Anticoagulation is the cornerstone of CSVT treatment and indirectly reduces ICP by limiting thrombosis progression and allowing recanalization. For acute ICP management, the following are used:
| Intervention | Comment |
|---|---|
| Head elevation (30°) | First-line, always |
| Hypertonic saline / mannitol | For acute ICP crises — short-term bridging only |
| Acetazolamide | Reduces CSF production; used in chronic ICP elevation in CSVT |
| Lumbar puncture / CSF drainage | Both diagnostic and therapeutic in CSVT with isolated ICP |
| Anticoagulation (LMWH/UFH) | Definitive treatment — does NOT worsen hemorrhage risk |
"Treatment must be individualized, but anticoagulation is the cornerstone to prevent progression of thrombosis even in the presence of intracranial hemorrhage. Additional treatment should be directed at the management of secondary effects such as elevated ICP." — Plum & Posner's Diagnosis and Treatment of Stupor and Coma
3% NaCl — Dosing (Pediatric)
From pediatric TBI guidelines (Level II/III evidence — best available for pediatric hyperosmolar therapy):
| Route | Dose |
|---|---|
| Bolus (acute ICP crisis) | 2–5 mL/kg IV over 10–20 minutes; some sources up to 6.5–10 mL/kg |
| Continuous infusion | 0.1–1.0 mL/kg/hour titrated to ICP response |
| Maximum single dose | 500 mL |
Target serum sodium: 145–155 mEq/L (do not exceed 160 mEq/L)
Target serum osmolality: do not exceed 360 mOsm/kg
For a 13-year-old (average ~45–50 kg):
- Bolus: ~90–250 mL of 3% NaCl over 15–20 min (2–5 mL/kg)
- Infusion: 4.5–50 mL/hr titrated to response
Special Considerations: Intellectual Disability
A patient with intellectual disability (ID) presents specific challenges:
- Cannot reliably report headache — ICP may be underrecognized until late
- Baseline neurological exam is altered — detecting clinical deterioration requires familiarity with baseline behavior
- Agitation/behavioral change may be the only sign of worsening ICP or seizure
- Seizure threshold may be lower — CSVT-associated seizures are more likely; continuous EEG monitoring should be considered
- Consent and cooperation — IV access, monitoring, and medications may require additional support
Clinical pearl: In a non-verbal or minimally verbal child with ID, do not wait for the classic triad of raised ICP. Act on behavioral change + fundoscopy findings + imaging.
Important Cautions with 3% NaCl in CSVT Specifically
⚠️ 3% NaCl is a temporizing measure — it does NOT treat CSVT. Key cautions:
- Do not delay anticoagulation in favor of osmotherapy — anticoagulation (LMWH or UFH) should be started promptly once CSVT is confirmed (or strongly suspected) even if hemorrhagic transformation is present
- Avoid hypotonic fluids — they worsen cerebral edema; all maintenance fluids should be isotonic
- Monitor sodium closely — rapid sodium correction carries risk of osmotic demyelination; aim for gradual, controlled rises
- Mannitol is a less preferred alternative in CSVT with raised ICP — it causes osmotic diuresis and can worsen dehydration, which may propagate venous thrombosis. HTS is therefore preferred over mannitol in this specific context.
- Imaging first if time permits: MRI + MRV is gold standard; CT venography is acceptable emergently
Summary Decision Framework
Suspected CSVT + raised ICP signs in 13-yr-old with ID
│
├─ Secure airway/IV access
├─ Urgent MRI-MRV or CT-venography
├─ Head of bed 30°, avoid hypotonic fluids
│
├─ ICP crisis present (GCS drop, herniation signs)?
│ YES → 3% NaCl 2–5 mL/kg IV bolus over 15–20 min
│ Monitor Na+, osmolality; repeat if needed
│ Avoid mannitol (worsens dehydration → propagates CSVT)
│
├─ Start anticoagulation (LMWH preferred) — do NOT delay
│ Even if hemorrhagic infarct present
│
├─ Seizure? → Treat with LEV (preferred)
│ No routine prophylaxis
│
└─ Acetazolamide for chronic ICP elevation (post-acute phase)
Sources: Plum & Posner's Diagnosis & Treatment of Stupor and Coma; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Pediatric TBI Guidelines (Greenfield's Surgery); Mulholland & Greenfield's Surgery
From Victor and Adams
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.