Teach me topic of urolithiasis from symptoms till management each and every aspect of this topic from campbell book of urology and other authentic sources
Reading File
search_medical_text
urolithiasis kidney stones etiology pathophysiology types classification
search_medical_text
urolithiasis renal calculi symptoms diagnosis imaging management treatment
search_medical_image
kidney stones urolithiasis CT scan imaging types
GradeResponse
GradeResponse
GradeResponse
search_medical_text
renal colic presentation hematuria flank pain ureteral stone symptoms
search_medical_text
urolithiasis metabolic evaluation 24-hour urine hypercalciuria hyperoxaluria hyperuricosuria risk factors
I have solid retrieved content and will now synthesize a comprehensive, well-structured answer from retrieved sources combined with my extensive knowledge of Campbell's Urology, Harrison's, EAU/AUA guidelines, and Bailey & Love's.
Urolithiasis: A Comprehensive Review
Based on Campbell-Walsh-Wein Urology (12th Ed.), Harrison's Principles of Internal Medicine (21st Ed.), Bailey & Love's Short Practice of Surgery (28th Ed.), and EAU/AUA Guidelines
1. INTRODUCTION & EPIDEMIOLOGY
Urolithiasis is one of the most ancient and prevalent urological conditions known to medicine. The first documented cystolithotomy was described by Sushruta, an ancient Indian surgeon, around 600 BCE (Bailey & Love, p. 1495).
Key Epidemiological Facts (Campbell-Walsh-Wein):
- Lifetime prevalence: 10–15% in developed nations; rising globally
- Male:Female ratio: 2–3:1 (gap narrowing due to obesity epidemic)
- Peak incidence: 40–60 years of age
- Recurrence rate: ~50% within 5–7 years without preventive therapy; ~75% within 20 years
- "Stone Belt" (southeastern USA, Middle East, Indian subcontinent) — geographic clustering due to heat, dehydration
- Modern world witnessing steady increase in renal calculi coinciding with obesity, diabetes, and metabolic syndrome (Bailey & Love, p. 1495)
2. TYPES OF STONES & THEIR FREQUENCIES
(Harrison's, p. 8691)
| Stone Type | Frequency | Appearance on CT | Key Feature |
|---|---|---|---|
| Calcium Oxalate | ~75% | Hyperdense (>400 HU) | Most common; often mixed with CaPO₄ |
| Calcium Phosphate | ~15% | Hyperdense | Associated with RTA type I, hyperPTH |
| Uric Acid | ~8% | Radiolucent on X-ray; visible on CT | Radiolucent; treated medically |
| Struvite (Magnesium Ammonium Phosphate) | ~1–2% | Staghorn calculi | Urease-producing organisms (Proteus, Klebsiella) |
| Cystine | <1% | Moderately dense | Autosomal recessive cystinuria |
| Drug-induced | Rare | Variable | Acyclovir, atazanavir, triamterene, indinavir |
"Many stones are a mixture of crystal types (e.g., calcium oxalate and calcium phosphate) and also contain protein in the stone matrix." (Harrison's, p. 8691)
3. PATHOPHYSIOLOGY & STONE FORMATION
3.1 Fundamental Principles (Campbell-Walsh-Wein)
Stone formation requires supersaturation of urine with lithogenic solutes. The key equation is:
Ion Activity Product (IAP) > Solubility Product (Ksp) → Crystallization
Stages of stone formation:
- Nucleation — crystal nuclei form (homogeneous or heterogeneous)
- Crystal growth — aggregation of crystals
- Crystal retention — Randall's plaques (subepithelial calcium phosphate deposits at papillary tips) anchor crystals
- Stone formation — organized mineral structure
3.2 Randall's Plaques
- Subepithelial apatite deposits in the renal papilla
- Serve as nidus for calcium oxalate monohydrate stone attachment
- Seen in idiopathic calcium oxalate stone formers (Campbell-Walsh-Wein)
3.3 Factors Promoting Crystallization
| Factor | Effect |
|---|---|
| ↑ Urinary calcium | Supersaturation |
| ↑ Urinary oxalate | Most potent promoter of CaOx stones |
| ↑ Urinary uric acid | Nidus for CaOx stones |
| ↓ Urinary citrate | Major inhibitor lost |
| ↓ Urine volume | Concentrates all solutes |
| Low urine pH | Promotes uric acid stones |
| High urine pH | Promotes calcium phosphate, struvite |
3.4 Inhibitors of Crystallization
- Citrate (most important — chelates calcium)
- Tamm-Horsfall protein (uromodulin)
- Osteopontin
- Nephrocalcin
- Magnesium
4. ETIOLOGY & RISK FACTORS
4.1 Metabolic Risk Factors
A. Hypercalciuria (urine Ca >250 mg/day in women, >300 mg/day in men)
Three types:
- Absorptive (Type I, II, III) — most common; excess intestinal Ca absorption
- Resorptive — hyperparathyroidism, bone resorption
- Renal — impaired tubular Ca reabsorption
B. Hyperoxaluria
- Primary hyperoxaluria (Types 1, 2, 3) — genetic enzyme defects; severe
- Enteric hyperoxaluria — Crohn's disease, bariatric surgery (Roux-en-Y), short bowel syndrome
- Dietary — excess spinach, nuts, chocolate, vitamin C megadoses
C. Hyperuricosuria (urine uric acid >600–800 mg/day)
- Purine-rich diet, gout, tumor lysis syndrome
- Acts as heterogeneous nucleus for CaOx stones
D. Hypocitraturia (urine citrate <320 mg/day)
- Distal RTA type I
- Chronic diarrheal states, IBD
- Hypokalemia
- High-protein diet
E. Low Urine Volume (<1 L/day)
- Most significant modifiable risk factor
- Dehydration, hot climate, inadequate fluid intake
F. Abnormal Urine pH
- Persistently acidic urine (pH <5.5) → uric acid stones
- Persistently alkaline urine (pH >6.5) → calcium phosphate, struvite
4.2 Systemic Conditions Associated with Stones
| Condition | Stone Type |
|---|---|
| Primary hyperparathyroidism | Calcium (oxalate/phosphate) |
| Distal RTA (Type I) | Calcium phosphate |
| Crohn's disease / IBD | Calcium oxalate (enteric hyperoxaluria) |
| Gout | Uric acid |
| Obesity / Metabolic syndrome | Uric acid, calcium oxalate |
| Type 2 Diabetes mellitus | Uric acid |
| Medullary sponge kidney | Calcium, struvite |
| Cystinuria | Cystine |
| Sarcoidosis | Calcium (hypercalcemia/hypercalciuria) |
| Bariatric surgery (RYGB) | Calcium oxalate |
| Chronic UTI (Proteus, Klebsiella) | Struvite |
4.3 Dietary & Lifestyle Risk Factors
- High sodium intake → ↑ urinary calcium
- High animal protein → ↑ urinary uric acid, oxalate; ↓ citrate; ↓ urine pH
- Low calcium diet (paradoxically) → ↑ intestinal oxalate absorption
- Dehydration / low fluid intake
- Obesity (BMI >30)
- Sedentary lifestyle
4.4 Anatomical Risk Factors
- Ureteropelvic junction (UPJ) obstruction — urinary stasis
- Horseshoe kidney — impaired drainage
- Medullary sponge kidney
- Vesicoureteral reflux
- Urinary diversion (ileal conduit)
- Foreign bodies (stents, catheters as nidus)
5. CLINICAL PRESENTATION
5.1 Renal Colic (Classic Presentation)
The hallmark symptom is sudden-onset, severe, colicky flank pain radiating to the groin, ipsilateral testis/labia, and inner thigh — following the course of the ureter.
Key characteristics:
- Onset: Abrupt, often waking patient from sleep
- Character: Colicky (waxes and wanes) — due to ureteral peristalsis against obstruction
- Severity: One of the most severe pains described; patients cannot find a comfortable position (unlike peritonitis where patients lie still)
- Radiation: Classically "loin to groin"; may radiate to genitalia
- Associated symptoms:
- Nausea and vomiting (very common — due to shared celiac innervation)
- Urinary urgency and frequency (distal ureteral stones)
- Gross or microscopic hematuria (~85% cases)
- Diaphoresis
5.2 Stone Location and Symptom Pattern
| Stone Location | Pain/Symptom Pattern |
|---|---|
| Renal calyx | Dull, aching flank pain or asymptomatic |
| Renal pelvis | Flank/back pain, may be episodic |
| Upper ureter | Severe flank pain, radiation to flank/loin |
| Mid-ureter | Pain radiating toward lower quadrant |
| Distal ureter | Pain to ipsilateral groin, testicle/labia; LUTS (frequency, urgency, dysuria) |
| UVJ (ureterovesical junction) | Mimics cystitis; frequency, urgency, suprapubic pain |
5.3 Physical Examination
- Costovertebral angle (CVA) tenderness — hallmark finding
- Patient is restless, writhing (distinguishes colic from peritonitis)
- Abdominal tenderness may be present
- Fever + CVA tenderness → infected obstructed stone — urological emergency
5.4 Special Situations
- Silent stones — large staghorn calculi may be asymptomatic; discovered incidentally
- Bilateral ureteral obstruction → anuria, acute kidney injury
- Obstructed infected kidney → urosepsis, pyonephrosis (emergency decompression required)
6. DIAGNOSIS
6.1 Laboratory Investigations
Urine Analysis (Urinalysis + Microscopy)
- Hematuria: Present in ~85% (microhematuria is common; absence does not exclude stone)
- Pyuria: Suggests concurrent UTI or struvite stone
- Urine pH: <5.5 (uric acid); >7.0 (struvite/infection)
- Crystals on microscopy:
- Envelope-shaped (octahedral) → Calcium oxalate dihydrate
- Dumbbell/biconcave disc → Calcium oxalate monohydrate
- Coffin-lid hexagonal → Struvite
- Flat hexagonal plates → Cystine
- Rhomboid/needle → Uric acid
Urine Culture — mandatory; UTI with obstructing stone = emergency
Serum Investigations:
- BMP/CMP (creatinine, BUN, electrolytes) — renal function
- Serum calcium — hyperparathyroidism screen
- Serum uric acid
- PTH (if hypercalcemia present)
- Serum phosphate
- CBC — leukocytosis with infected stone
6.2 Imaging
A. Non-contrast CT Abdomen/Pelvis (NCCT) — Gold Standard
As illustrated in the retrieved image: "Axial contrast-enhanced CT scan demonstrating a small, hyperdense focus (white arrow) within the interpolar calyx of the right kidney, characteristic of a renal stone. The CT provides high spatial resolution with distinct corticomedullary differentiation."
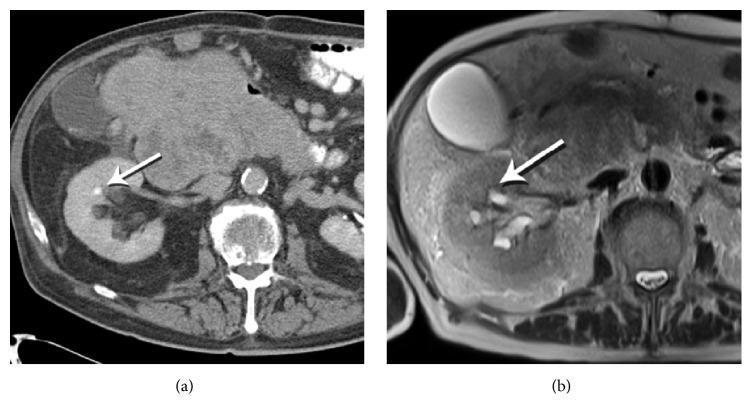
- Sensitivity: 95–100%, Specificity: 94–96% (Campbell-Walsh-Wein)
- Detects ALL stone types including radiolucent uric acid stones
- Identifies stone size, location, density (HU), skin-to-stone distance
- Identifies secondary signs: hydronephrosis, perinephric stranding (hydroureter)
- Detects alternative diagnoses (appendicitis, AAA, ovarian pathology)
- HU (Hounsfield Units) of stones:
- Uric acid: 200–400 HU (lowest)
- Calcium oxalate: 400–800 HU
- Calcium phosphate: 800–1200 HU
- Cystine: ~600 HU
- Low-dose CT protocols now standard to reduce radiation
"MRI fails to clearly identify the stone at the corresponding location... This comparison highlights the superior sensitivity of non-contrast or contrast-enhanced CT over certain MRI sequences for identifying small nephrolithiasis." (Retrieved image caption)
B. Ultrasound (US)
- First-line in children, pregnant women, suspected renal colic without need for immediate intervention
- Sensitivity ~45–67% for ureteral stones (poor mid-ureter visualization)
- Excellent for: hydronephrosis, large renal stones, monitoring
- Can detect twinkling artifact on Doppler — pathognomonic for calculi
- No radiation
- Point-of-care US (POCUS) increasingly used in ED
C. Plain Abdominal X-Ray (KUB — Kidney, Ureter, Bladder)
- Detects radiopaque stones (CaOx, CaPO₄, cystine)
- Radiolucent stones (uric acid, some drug stones) → not visible
- Sensitivity ~44–59%; Specificity ~71–77%
- Useful for monitoring known radiopaque stones
- Useful combined with US (KUB + US) as radiation-sparing alternative to CT
D. CT Urogram (CTU) / IVP (Intravenous Pyelogram)
- IVP largely replaced by CTU
- CTU: Excellent anatomical detail of collecting system; identifies strictures, UPJ obstruction
- Used preoperatively for surgical planning
E. MRI
- Reserved for pregnancy (when US inconclusive) or when CT is contraindicated
- Poor sensitivity for stones (stones appear as signal voids)
- Good for soft tissue evaluation
F. Retrograde Pyelogram (RGP)
- Invasive; reserved for diagnostic uncertainty or during endoscopic procedures
- Gold standard for collecting system anatomy
6.3 Metabolic Evaluation (Stone Prevention Workup)
Indicated in:
- First stone in high-risk patients (family history, single kidney, IBD, gout)
- Recurrent stone formers
- Bilateral or multiple stones
- Pediatric stone formers
- AUA Guidelines: recommended for all recurrent stone formers and selected first-time formers
First evaluation (spot tests):
- Serum: Ca, Phosphate, Uric acid, Creatinine, PTH, CO₂, Na, K
- Urinalysis with culture
- Stone analysis (if available)
24-hour urine collection (KEY — performed twice):
| Parameter | Normal | Abnormal Finding | Implication |
|---|---|---|---|
| Volume | >2.5 L/day | <2 L/day | Low volume |
| Calcium | <200 mg/day (F) / <250 mg/day (M) | Elevated | Hypercalciuria |
| Oxalate | <40 mg/day | >40 mg/day | Hyperoxaluria |
| Uric acid | <600 mg/day (F) / <800 mg/day (M) | Elevated | Hyperuricosuria |
| Citrate | >320 mg/day | <320 mg/day | Hypocitraturia |
| Sodium | Reflects dietary intake | >200 mEq/day | High salt diet |
| pH | 5.8–6.2 | <5.5 or >7.0 | Stone-type specific risk |
| Magnesium | >50 mg/day | Low | Risk factor |
| Creatinine | Confirms adequacy of collection |
7. MANAGEMENT
7.1 Acute Management of Renal Colic
A. Analgesia (Priority #1)
| Analgesic | Notes |
|---|---|
| NSAIDs (Diclofenac, Ketorolac, Ibuprofen) | First-line — superior to opioids for renal colic; reduce ureteral spasm and inflammation; reduce recurrence of pain |
| Opioids (Morphine, Pethidine) | Used when NSAIDs contraindicated (CKD, GI bleed) or insufficient alone |
| Combination (NSAID + Opioid) | More effective than either alone |
| Antispasmodics | Limited evidence; hyoscine butylbromide sometimes used |
| IV Paracetamol | Adjunct analgesic |
NSAIDs act by reducing prostaglandin-mediated ureteral smooth muscle tone and decreasing intrarenal pressure — superior analgesic effect in renal colic vs opioids (Campbell-Walsh-Wein).
B. Antiemetics
- Metoclopramide, ondansetron (for nausea/vomiting)
C. IV Fluids
- Correct dehydration
- Forcing fluids is NOT recommended in acute colic — increases collecting system pressure and pain
D. Infection Control
- Infected obstructing stone = UROLOGICAL EMERGENCY
- Urgent decompression (ureteral stent or percutaneous nephrostomy) + IV antibiotics
- Do NOT attempt stone removal in acute infected setting
7.2 Medical Expulsive Therapy (MET)
Principle: Alpha-1 blockers relax ureteral smooth muscle (particularly at the UVJ), facilitating spontaneous stone passage.
Agents:
- Tamsulosin 0.4 mg OD — most studied and used (alpha-1a/1d selective)
- Silodosin — highly selective alpha-1a
- Doxazosin, Terazosin — less selective, less commonly used
- Calcium channel blockers (Nifedipine) — some evidence but less than alpha-blockers
Indications for MET (AUA/EAU Guidelines):
- Distal ureteral stone ≤10 mm
- No absolute indication for immediate intervention
- Adequate pain control
Spontaneous passage rates (Campbell-Walsh-Wein):
| Stone Size | Spontaneous Passage Rate |
|---|---|
| ≤4 mm | ~80–90% |
| 5–7 mm | ~50–60% |
| 7–10 mm | ~25–30% |
| >10 mm | <15% (surgical intervention usually needed) |
Observation period: Up to 4–6 weeks if pain controlled, renal function preserved, no infection
Indications to abandon MET and proceed to intervention:
- Failed passage after 4–6 weeks
- Uncontrolled pain
- Fever/infection (emergency)
- Progressive obstruction / deteriorating renal function
- Solitary kidney with obstruction
- Bilateral obstructing stones
7.3 Surgical Intervention
A. Shock Wave Lithotripsy (SWL)
Mechanism: High-energy acoustic shockwaves focused externally onto the stone, causing fragmentation via compressive/tensile forces and cavitation bubbles.
Indications (EAU/AUA):
- Renal stones ≤20 mm (optimal ≤15 mm)
- Proximal ureteral stones ≤10 mm
- Stone composition favorable (CaOx dihydrate, uric acid, struvite)
Contraindications:
- Pregnancy (absolute)
- Uncorrected coagulopathy / anticoagulation
- Uncontrolled UTI
- Obstruction distal to stone
- Aortic/renal artery aneurysm near stone
- Morbid obesity, bony deformity (stone cannot be focused)
- Cystine and calcium oxalate monohydrate stones (hard — poor fragmentation)
Outcomes:
- Stone-free rate: ~70–85% for renal stones ≤10 mm
- Lower for larger stones, lower pole location, hard stones
- Side effects: hematoma, steinstrasse ("stone street"), hypertension (controversial), renal parenchymal injury
B. Ureteroscopy (URS) + Laser Lithotripsy
Mechanism: Rigid or flexible ureteroscope passed transurethrally → fragmentation with Holmium:YAG laser (gold standard) or thulium fiber laser.
Indications:
- Ureteral stones of any size
- Renal stones ≤20 mm
- SWL failure or contraindication
- Lower pole stones
- Hard stones (cystine, CaOx monohydrate)
- Need for definitive tissue diagnosis
- Pregnancy (can be performed safely)
Types:
- Rigid URS — distal/mid ureter
- Semi-rigid URS — up to renal pelvis
- Flexible URS (FURS) / Digital URS — all renal calyces
Holmium:YAG Laser:
- Wavelength 2100 nm; absorbed by water
- Fragments all stone types
- Can be used in dusting mode (stone dust <0.5 mm) or fragmentation + basketing mode
Thulium Fiber Laser (TFL):
- Newer technology; superior fragmentation efficiency, faster dusting
- Lower retropulsion
Outcomes: Stone-free rates >90% for ureteral stones; 80–90% for renal stones ≤20 mm (Campbell-Walsh-Wein)
Complications: Ureteral perforation, avulsion, stricture, mucosal injury, sepsis (pre-op urine culture mandatory)
DJ Stent: Placed post-URS for 1–2 weeks if ureteral edema, perforation, or risk of obstruction
C. Percutaneous Nephrolithotomy (PCNL)
Mechanism: Percutaneous tract established from skin through renal parenchyma into collecting system under fluoroscopic/US guidance → nephroscope introduced → stone fragmentation and removal.
Indications:
- Renal stones >20 mm
- Staghorn/struvite stones (partial or complete)
- Lower pole stones >15 mm (where SWL poorly effective)
- SWL/URS failure
- Horseshoe kidney, transplant kidney
- Associated infundibular stenosis requiring simultaneous correction
Approaches:
- Standard PCNL — 24–30 Fr tract
- Mini-PCNL — 14–20 Fr tract
- Ultra-mini PCNL — 11–13 Fr
- Micro-PCNL — 4.8 Fr (for small stones)
- Smaller tracts → less bleeding, faster recovery, but longer operative time
Energy sources: Ultrasonic lithotripsy, pneumatic (ballistic), Holmium laser, combination (EMS, LithoClast Master)
Outcomes:
- Stone-free rate: 85–90% for large stones (Campbell-Walsh-Wein)
- Highest stone-free rates of all modalities for complex/large stones
Complications: Bleeding (major hemorrhage ~1–3% requiring transfusion/angioembolization), pleural injury (upper pole access), collecting system injury, sepsis, urine leak
D. Laparoscopic / Robotic-Assisted Surgery
- Pyelolithotomy / Ureterolithotomy
- Indicated for very large stones with concurrent anatomy requiring correction (UPJ obstruction + large stone)
- Largely replaced by PCNL/URS but used in complex cases
E. Open Surgery
- Rare; reserved for failed endourological approaches, complex anatomy, simultaneous reconstruction required
7.4 Stone-Type Specific Management
Calcium Stones (Oxalate & Phosphate)
Dietary measures (ALL calcium stone formers):
- Fluid intake — urine output >2.5 L/day (most important)
- Dietary calcium 1000–1200 mg/day — do NOT restrict (binds intestinal oxalate)
- Reduce sodium (<2300 mg/day) — reduces calciuria
- Reduce animal protein (<0.8–1 g/kg/day)
- Reduce oxalate-rich foods (spinach, nuts, chocolate, tea)
- Avoid vitamin C megadoses
Pharmacological:
- Hypercalciuria: Thiazide diuretics (Hydrochlorothiazide 25–50 mg/day, Chlorthalidone) — increase renal tubular calcium reabsorption
- Hypocitraturia: Potassium citrate (30–60 mEq/day) — alkalinizes urine, increases urinary citrate
- Hyperoxaluria (enteric): Calcium carbonate with meals (binds intestinal oxalate), low-fat diet, cholestyramine
- Hyperoxaluria (primary Type 1): Pyridoxine (B6); liver-kidney transplant in severe cases; Lumasiran (siRNA therapy — new)
- Hyperuricosuria contributing to CaOx stones: Allopurinol 300 mg/day, potassium citrate
Uric Acid Stones
Key point: Uric acid stones are the ONLY type treatable non-surgically by dissolution (chemolysis)
Mechanism of dissolution: Uric acid is soluble at pH >6.5; urinary alkalinization dissolves stones
Management:
- Oral alkalinization — Potassium citrate 40–80 mEq/day (target urine pH 6.5–7.0)
- High fluid intake — urine output >2.5 L/day
- Reduce purine intake (red meat, organ meats, shellfish, beer)
- Allopurinol 300 mg/day (if hyperuricosuria or hyperuricemia)
- Febuxostat — alternative xanthine oxidase inhibitor
Dissolution rate: 10–12 mm/month with alkalinization (Campbell-Walsh-Wein)
Monitoring: Serial KUB (uric acid stones are radiolucent on KUB but visible on CT); urine pH monitoring
Struvite (Infection) Stones
- Caused by urease-producing organisms: Proteus mirabilis (most common), Klebsiella, Pseudomonas, Staphylococcus (some strains), Ureaplasma
- Urease splits urea → NH₃ + CO₂ → alkaline urine (pH >7) → struvite precipitation
- Form staghorn calculi (occupying renal pelvis + calyces)
- Cause significant morbidity: recurrent UTI, sepsis, renal damage, end-stage renal disease
Management:
- Complete stone removal is the only cure (bacteria reside within stone matrix)
- PCNL (procedure of choice for staghorn calculi)
- SWL (adjunct)
- Combined approach for complete clearance
- Perioperative antibiotics based on culture sensitivities
- Acetohydroxamic acid (AHA) — urease inhibitor; used as adjunct only (poor tolerance, side effects)
- Urine acidification + antibiotics — maintenance after surgery
- Long-term surveillance with cultures and imaging
Cystine Stones
- Autosomal recessive disorder of SLC3A1/SLC7A9 gene mutations → defective renal tubular transport of COLA (cystine, ornithine, lysine, arginine) → cystinuria
- Onset in childhood/young adults; highly recurrent
- Cystine solubility only ~250 mg/L
Medical dissolution/prevention:
- Massive hydration — urine output >3–4 L/day (most critical); ≥300 mL/hour overnight
- Urinary alkalinization — potassium citrate/sodium bicarbonate; target urine pH ≥7.0–7.5
- Dietary protein restriction — reduce methionine (cystine precursor)
- Thiol-binding agents (if above insufficient):
- D-Penicillamine — forms soluble penicillamine-cysteine disulfide; significant side effects
- Tiopronin (α-Mercaptopropionylglycine, Thiola) — preferred over penicillamine; fewer side effects; forms soluble tiopronin-cysteine complex
- Captopril — mild effect; third line
Surgical:
- PCNL or URS (cystine is moderately hard; responds to holmium laser)
- Highly recurrent; lifelong monitoring required
7.5 Special Populations
Pregnancy
- Incidence ~1 in 200–1500 pregnancies
- 80–85% pass spontaneously
- First-line imaging: Renal ultrasound
- MRI if US inconclusive (no radiation)
- Avoid CT if possible (ionizing radiation)
- Conservative management first (hydration, analgesia — acetaminophen preferred)
- Ureteroscopy with ureteral stenting: safe in all trimesters; preferred over SWL (absolute contraindication in pregnancy)
- Alpha-blockers: not routinely recommended in pregnancy
- PCNL: avoided if possible but can be performed with US guidance
Pediatric Urolithiasis
- Rising incidence (obesity, dietary changes, antibiotic-related dysbiosis)
- Metabolic workup MANDATORY in all children
- Consider primary hyperoxaluria, cystinuria, distal RTA, hypercalcemia
- Genetic testing increasingly important
- Management: SWL (first-line for small stones), ureteroscopy (flexible; smaller instruments), mini-PCNL
- Long-term dietary counseling critical
Single Kidney / Solitary Functional Kidney
- Any obstructing stone = urgent intervention
- Lower threshold for intervention
- Goal: complete stone clearance to prevent recurrence
Renal Transplant
- Stone in transplanted kidney: difficult anatomy (iliac fossa, ureter short)
- URS preferred; PCNL feasible with anterior percutaneous access
- SWL: used cautiously
8. STAGHORN CALCULI
Definition: Calculus occupying ≥2 calyceal systems of the kidney; typically struvite or cystine
- Partial staghorn — 1 calyx + pelvis
- Complete staghorn — pelvis + all major calyceal groups
Management (AUA Guidelines — Staghorn Calculus Panel):
- PCNL is the standard of care for staghorn calculi
- Complete stone clearance is the goal
- Combined PCNL + SWL ("sandwich therapy") for complex stones
- Anatrophic nephrolithotomy: rarely needed; last resort
- Open surgery: if endourological approach not feasible
9. COMPLICATIONS OF UROLITHIASIS
| Complication | Notes |
|---|---|
| Acute ureteral obstruction | Hydronephrosis, AKI |
| Obstructive pyelonephritis / Urosepsis | Emergency — decompress urgently |
| Pyonephrosis | Infected hydronephrosis → surgical emergency |
| Xanthogranulomatous pyelonephritis | Chronic obstruction + infection → non-functioning kidney |
| Renal scarring / CKD | Chronic obstruction or recurrent infection |
| Hypertension | Renal scarring |
| Ureteral stricture | After impacted stone or intervention |
| End-stage renal disease | Struvite stones especially (Harrison's, p. 8691) |
| Increased cardiovascular risk | Associated metabolic syndrome |
"Stones that form as a result of an upper tract infection, if not appropriately treated, can have devastating consequences and lead to end-stage renal disease." (Harrison's, p. 8691)
10. PREVENTION & LONG-TERM FOLLOW-UP
Universal Measures (All Stone Types)
- Fluid intake: Target urine output >2–2.5 L/day — most evidence-based, most cost-effective intervention
- Dietary calcium: 1000–1200 mg/day from food (NOT supplements)
- Reduce sodium (<2300 mg/day)
- Reduce animal protein — limit to 0.8–1 g/kg/day
- Normal BMI — weight loss reduces uric acid excretion
- Lemon juice — citric acid source; increases urinary citrate
- Stone analysis of all retrieved stones
Stone-Specific Preventive Therapy Summary
| Stone Type | Key Medical Prevention |
|---|---|
| CaOx — hypercalciuria | Thiazide diuretic + low sodium diet |
| CaOx — hypocitraturia | Potassium citrate |
| CaOx — hyperoxaluria (dietary) | Low oxalate diet + calcium with meals |
| CaOx — hyperoxaluria (enteric) | Calcium carbonate with meals, low fat diet |
| CaOx — hyperuricosuria | Allopurinol + potassium citrate |
| Uric acid | Potassium citrate + reduce purines ± allopurinol |
| Struvite | Complete stone removal + treat infection |
| Cystine | Hydration + alkalinization + tiopronin if needed |
| Calcium phosphate (RTA) | Potassium citrate (correct acidosis) |
Follow-Up Schedule (AUA/EAU Guidelines)
- Stone analysis — all retrieved stones
- 24-hour urine — 6 weeks after starting medical therapy; then every 6–12 months
- Imaging — KUB/US every 6–12 months (CT as needed); avoid excessive CT exposure
- Serum metabolic panel annually
- Compliance assessment with dietary and pharmacological measures
11. SUMMARY ALGORITHM
Acute Flank Pain / Suspected Urolithiasis
↓
NCCT Abdomen/Pelvis (Gold Standard)
[US if pregnant/pediatric]
↓
Stone Confirmed?
YES → Size, Location, Obstruction?
↓
Fever/Sepsis? → YES → EMERGENCY DECOMPRESSION
(PCN or DJ stent) + IV Antibiotics
↓
NO INFECTION
↓
Stone ≤10 mm, Distal Ureter, No AKI?
↓
YES → Medical Expulsive Therapy (Alpha-blocker)
Observe 4–6 weeks
Adequate analgesia
↓
Passed? → YES → Metabolic workup + Prevention
↓
NO / Larger stone / Failed MET
↓
┌─────────────────────────────────────────────┐
│ SURGICAL OPTIONS │
│ • SWL: Renal ≤20mm, Proximal ureter ≤10mm │
│ • URS: Ureteral (any size), Renal ≤20mm │
│ • PCNL: Renal >20mm, Staghorn, SWL failure │
└─────────────────────────────────────────────┘
↓
Stone clearance → Metabolic evaluation
↓
Long-term medical prevention + surveillance
QUICK REFERENCE CARD
| Feature | Key Point |
|---|---|
| Most common stone | Calcium oxalate (~75%) |
| Gold standard imaging | NCCT (non-contrast CT) |
| First-line analgesia in colic | NSAIDs (e.g., diclofenac, ketorolac) |
| MET agent | Tamsulosin 0.4 mg OD |
| Only medically dissolvable stone | Uric acid (alkalinization) |
| Emergency scenario | Infected obstructing stone → urgent decompression |
| Most important prevention | Fluid intake → urine output >2.5 L/day |
| Best treatment for staghorn | PCNL |
| Radiolucent stone on KUB | Uric acid |
| Most potent urinary inhibitor | Citrate |
| Struvite cause | Urease-producing organisms (Proteus) |
| Staghorn stone complication | ESRD if untreated |
Sources: Campbell-Walsh-Wein Urology, 12th Edition; Harrison's Principles of Internal Medicine, 21st Ed. (p. 8691); Bailey & Love's Short Practice of Surgery, 28th Ed. (p. 1495); EAU Guidelines on Urolithiasis 2023; AUA Medical Management of Kidney Stones Guidelines 2019 (amended 2023); AUA Surgical Management of Stones 2016 (amended 2023)
This is a shared conversation. Sign in to Orris to start your own chat.